(UroToday.com) The 2026 American Urological Association annual meeting featured the International Prostate Forum and a presentation by Dr. Kristine Lacuna discussing how to select the best treatment for each patient in the first-line metastatic castration resistant prostate cancer (mCRPC) setting.
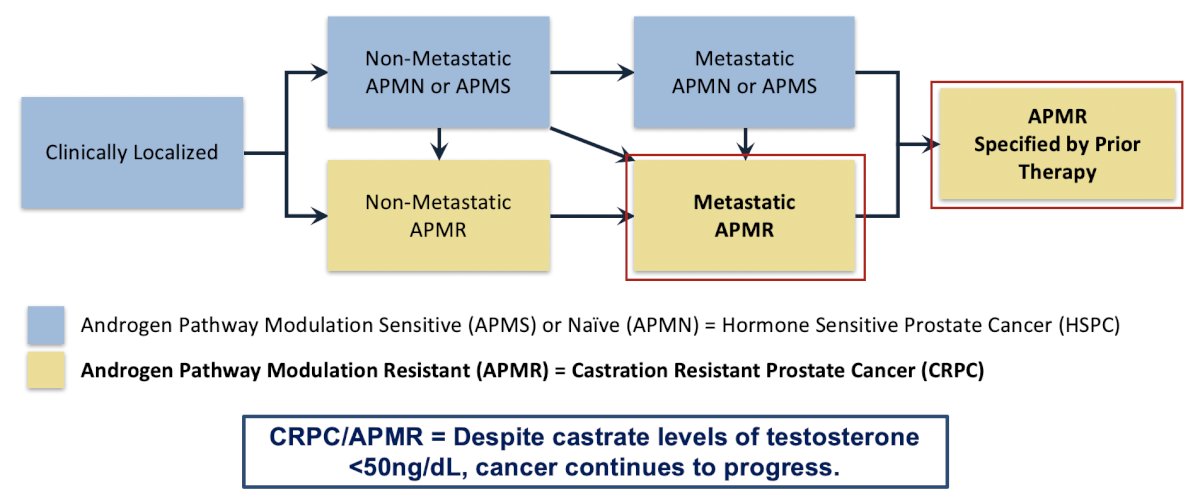
Dr. Lacuna started her presentation by emphasizing that PCWG4 changes the framework of the disease from an endocrinologic basis to a mechanistic one, which includes no use of the term castration.1 A key milestone is the use of prior androgen receptor-directed therapy (ADT alone or androgen receptor pathway inhibitor alone or doublet or triplet with another drug class, or novel androgen receptor targeted agent, etc):
We have many options for first-line mCRPC/APMR, including:
- Androgen receptor pathway inhibitors
- Chemotherapy
- Biomarker-driven agents
- HRR: PARP inhibitors
- MSI-H/dMMR, TMB-high: pembrolizumab
- Radioligand therapies/bone targeting agents:
- 177Lu-PSMA-617
- Radium-223

When selecting a patient’s first-line treatment for mCRPC/APMR, there are several factors to consider:
- Prior systemic therapy for HSPC/APMS will guide subsequent therapy used for mCRPC/APMR
- Early genomic testing (germline and somatic) is crucial for selecting treatment
- One size does not fit all – limited data exists for optimal sequencing of therapies. Treatment selection should be personalized and integrate disease burden, imaging characteristics, toxicity, and clinical context
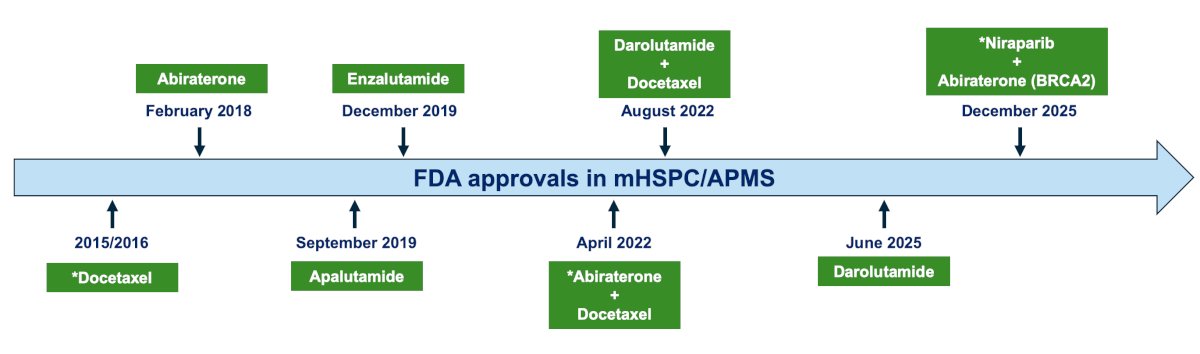
Dr. Lacuna emphasized that in contemporary times, escalation of therapy is recommended in mHSPC/APMS, with the following FDA approvals in this disease state:
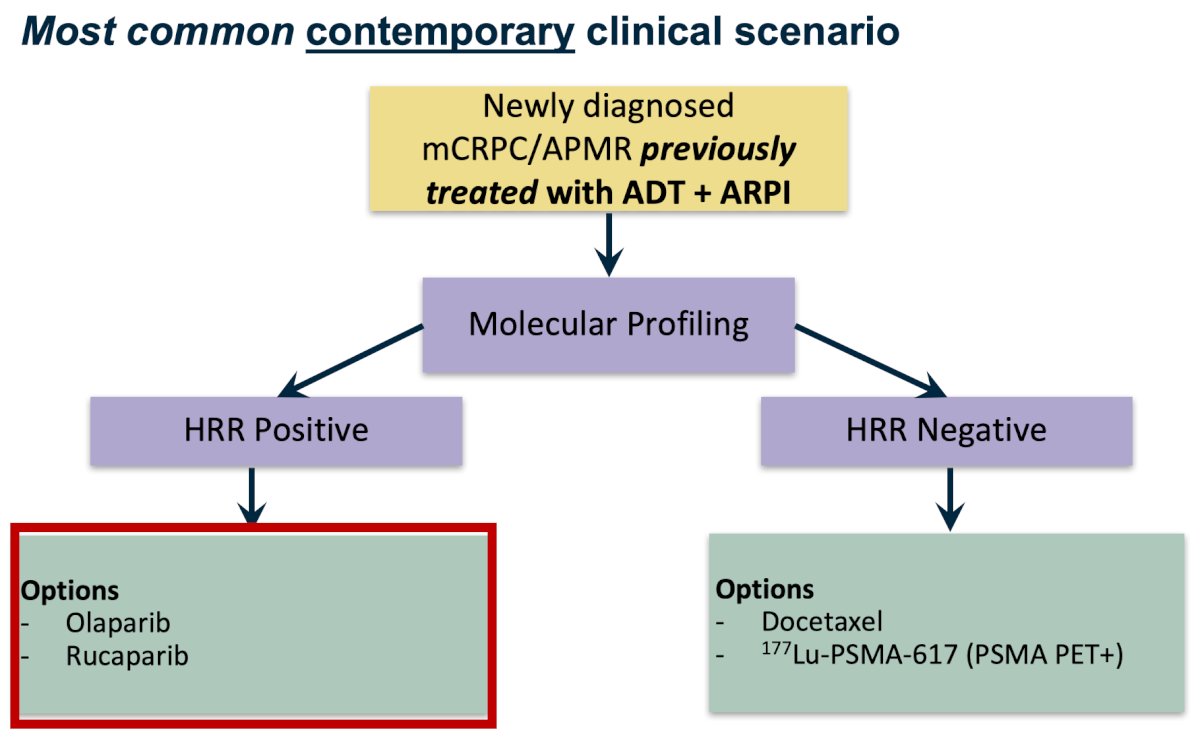
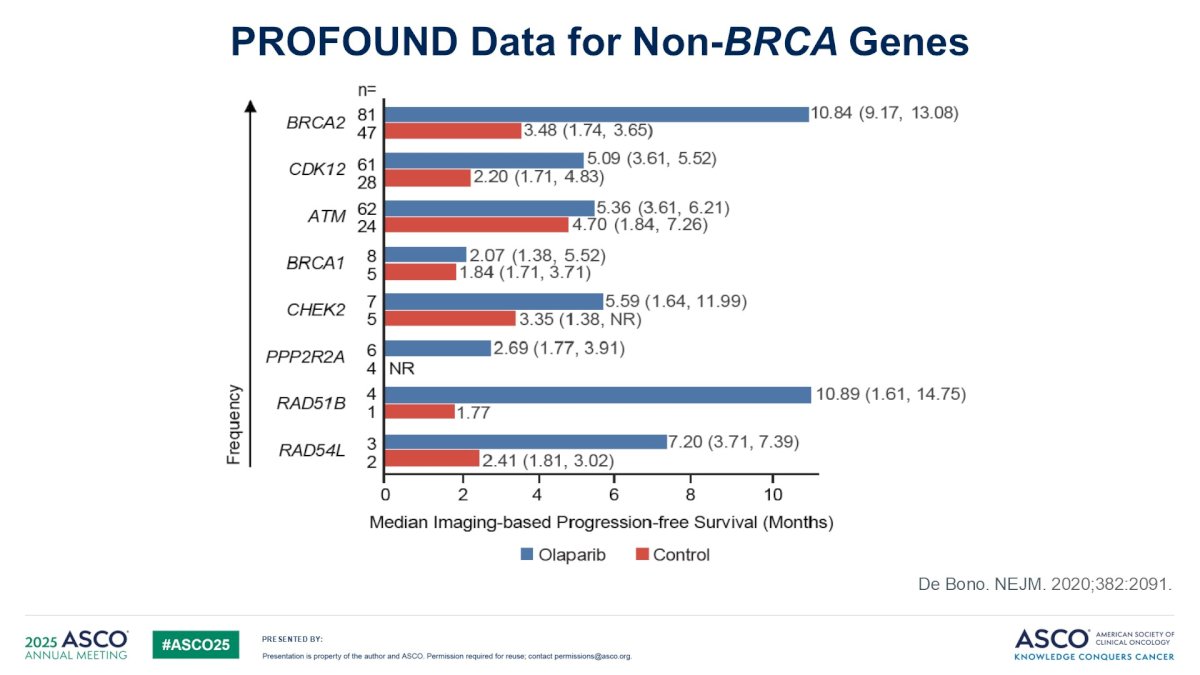
The most common contemporary clinical scenario is that newly diagnosed mCRPC/APMR patients will have previously been treated with ADT + an androgen receptor pathway inhibitor. They will subsequently undergo molecular profiling, and those that are HRR positive will receive olaparib (based on the PROfound trial2) or rucaparib (based on the TRITON3 trial3 ):
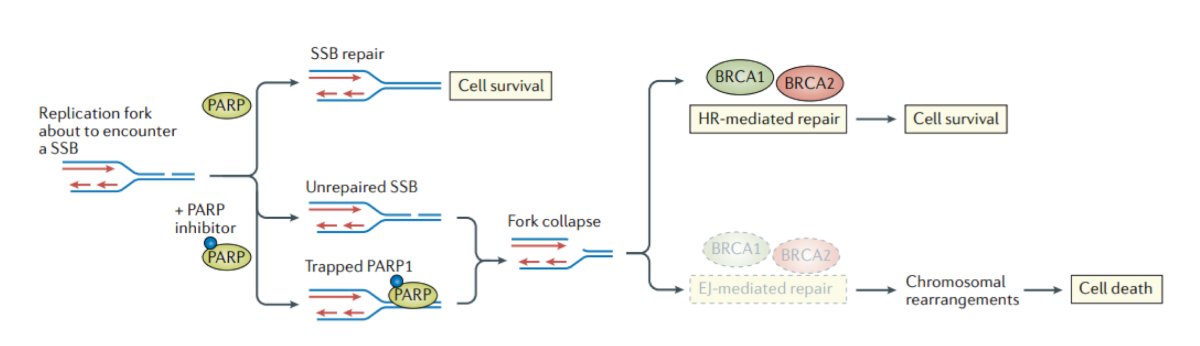
PARP inhibitors induce synthetic lethality, resulting in cell death, targeting cells with pre-existing DNA repair defects (ie. alterations in HRR):
Dr. Lacuna emphasized that, based on data from PROfound, radiographic progression-free survival based on HRR mutation suggests that not all HRR mutations are created equal: the benefit is greatest in patients with BRCA2 and BRCA-related alterations, with no clear benefit with ATM mutations.
For the patients that undergo molecular profiling and are HRR negative, patients can receive docetaxel (based on the TAX327 trial4) or 177Lu-PSMA-617 (based on the PSMAfore trial5). PSMAfore was a phase III randomized study of 177Lu-PSMA-617 versus an androgen receptor pathway inhibitor change for taxane-naïve mCRPC, post androgen receptor pathway inhibitor (not eligible for a PARP inhibitor), reporting a radiographic progression-free survival benefit for 177Lu-PSMA-617 (HR 0.49; 11.6 months versus 5.59 months), but without a reported overall survival benefit (HR 0.98, 23.66 months versus 23.85 months):
![For the patients that undergo molecular profiling and are HRR negative, patients can receive docetaxel (based on the TAX327 trial [4]) or 177Lu-PSMA-617 (based on the PSMAfore trial5). PSMAfore was a phase III randomized study of 177Lu-PSMA-617 versus an androgen receptor pathway inhibitor change for taxane-naïve mCRPC, post androgen receptor pathway inhibitor (not eligible for a PARP inhibitor), reporting a radiographic progression-free survival benefit for 177Lu-PSMA-617 (HR 0.49; 11.6 months versus 5.59 months), but without a reported overall survival benefit (HR 0.98, 23.66 months versus 23.85 months):](/images/com-doc-importer/263-aua-2026/aua-2026-advanced-prostate-cancer-first-line-mcrpc-apmr-how-do-i-select-the-best-treatment-for-my-patient/image-6.jpg)
How do we sequence 177Lu-PSMA-617 versus docetaxel? Although there is no “right” sequence, patient-centered factors are important. The PR21 trial gives us some insight, which looked at docetaxel versus 177Lu-PSMA-617 in patients with mCRPC, showing no difference in radiographic progression-free survival. However, overall survival favored patients treated with docetaxel, although crossover was allowed, potentially affecting outcomes.
Regarding mCRPC/APMR first-line therapy among patients previously treated with ADT + androgen receptor pathway inhibitors, Dr. Lacuna provided the following key takeaway points:
- In contemporary times, most patients with mCRPC/APMR have already received ADT + an androgen receptor pathway inhibitor
- If a patient has an HRR mutation (especially BRCA), consider leveraging PARP inhibitors first
- If there is no actionable mutation, most clinicians are choosing between first-line docetaxel versus 177Lu-PSMA-617:
- For 177Lu-PSMA-617, patients must be PSMA-PET positive
- There is a potentially better quality of life with 177Lu-PSMA-617
- There is no “right” sequence. Most patients will receive both therapies in their lifetime
The less common contemporary clinical scenario is that newly diagnosed mCRPC/APMR patients will not have previously been treated with ADT + an androgen receptor pathway inhibitor. They will subsequently undergo molecular profiling, and those that are HRR positive will receive olaparib + abiraterone for BRCA1/2 mutations (based on the PROpel trial6), or talazoparib + enzalutamide for all HRR mutations (based on the TALAPRO-2 trial7), or niraparib + abiraterone for BRCA1/2 mutations (based on the MAGNITUDE trial8):
![The less common contemporary clinical scenario is that newly diagnosed mCRPC/APMR patients will not have previously been treated with ADT + an androgen receptor pathway inhibitor. They will subsequently undergo molecular profiling, and those that are HRR positive will receive olaparib + abiraterone for BRCA1/2 mutations (based on the PROpel [6] trial), or talazoparib + enzalutamide for all HRR mutations (based on the TALAPRO-2 [7] trial), or niraparib + abiraterone for BRCA1/2 mutations (based on the MAGNITUDE [8] trial):](/images/com-doc-importer/263-aua-2026/aua-2026-advanced-prostate-cancer-first-line-mcrpc-apmr-how-do-i-select-the-best-treatment-for-my-patient/image-7.jpg)
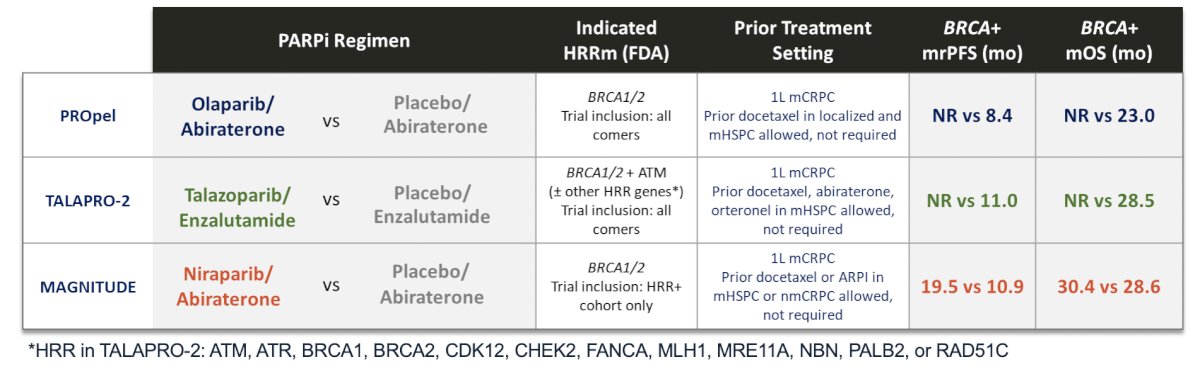
Dr. Lacuna notes that the benefit is unclear in patients previously treated with an androgen receptor pathway inhibitor (<5% prior use), with the greatest benefit in BRCA2 and BRCA-related alterations.
For the patients that are HRR negative, they can receive abiraterone (based on the COU-302 trial9), enzalutamide (based on the PREVAIL trial10), or docetaxel (based on the TAX-327 trial4), or enzalutamide + radium-223 (based on the PEACE-3 trial11). In PEACE-3, radium-223 + enzalutamide significantly improved radiographic progression-free survival and overall survival, with the following comparison of overall survival outcomes between the aforementioned trials:

Regarding mCRPC/APMR first-line therapy among patients not previously treated with ADT + androgen receptor pathway inhibitors, Dr. Lacuna provided the following key takeaway points:
- In contemporary times, it is less common to treat patients with mCRPC/APMR who have not received prior androgen receptor pathway inhibitors, but it happens, and when it does, we need to take advantage
- If a patient has an HRR mutation (especially BRCA), consider leveraging an androgen receptor pathway inhibitor + PARP inhibitors
- If there is no actionable mutation, strongly consider the PEACE-3 regimen of radium-223 + enzalutamide in patients with mCRPC/APMR with bone metastases
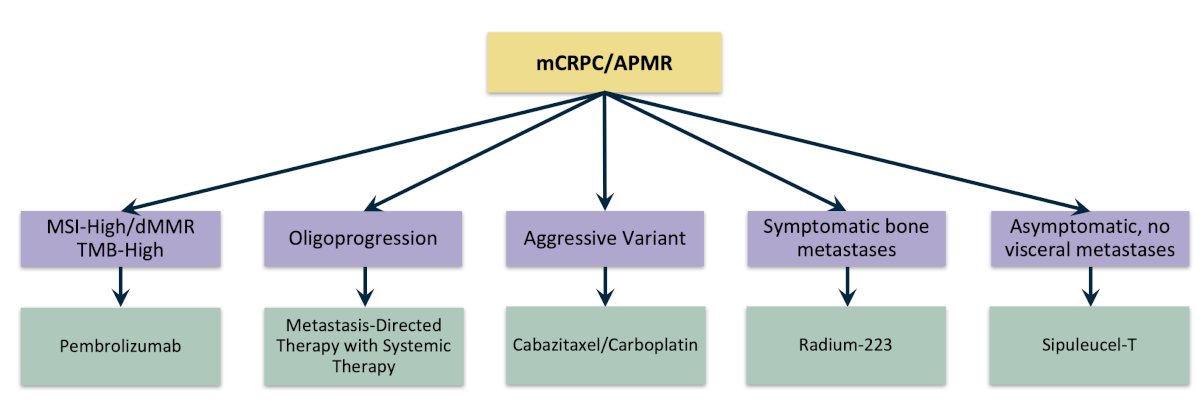
Aside from the aforementioned options, Dr. Lacuna highlighted other options for patients in the first line or beyond lines of therapy for mCRPC/APMR, which may be somewhat special situations:
Dr. Lacuna concluded her presentation discussing how to select the best treatment for each patient in the first-line mCRPC setting with the following take-home points:
- Selecting first-line therapy for mCRPC/APMR is dependent on prior treatments, disease characteristics, and patient factors
- If an HRR alteration is present (especially BRCA), consider leveraging genomically-directed therapy early on
- One size does not fit all – we should select personalized treatment that best fits the patient in front of us
Presented by: Kristine Peregrino Lacuna, MD, Medical Oncologist, Memorial Sloan Kettering Cancer Center, New York, NY
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the American Urological Association (AUA) 2026 Annual Meeting, Washington, DC, Fri, May 15 – Mon, May 18, 2026.
References:
- Armstrong AJ, Morris MJ, Abida W, et al. Trial design and objectives for patients with prostate cancer: Recommendations from the Prostate Cancer Working Group 4. J Clin Oncol. 2026 Feb 26 [Epub ahead of print].
- de Bono J, Mateo J, Fizazi K, et al. Olaparib for Metastatic Castration-Resistant Prostate Cancer. N Engl J Med 2020 May 28;382(22):2091-2102.
- Fizazi K, Piulats JM, Reaume MN, et al. Rucaparib or Physician’s Choice in Metastatic Prostate Cancer. N Engl J Med. 2023 Feb 23;388(8):719-732.
- Tannock IF, de Wit R, Berry WR, et al. Docetaxel plus prednisone or mitoxantrone plus prednisone for advanced prostate cancer. N Engl J Med 2004;351:1502-1512.
- Morris MJ, Castellano D, Herrmann K, et al. 177Lu-PSMA-617 versus a change of androgen receptor pathway inhibitor therapy for taxane-naïve patients with progressive metastatic castration-resistant prostate cancer (PSMAfore): A phase 3, randomized, controlled trial. Lancet 2024 Sep 28;404(10459):1227-1239.
- Saad F, Clarke NW, Oya M, et al. Olaparib plus abiraterone versus placebo plus abiraterone in metastatic castration-resistant prostate cancer (PROpel): final prespecified overall survival results of a randomized, double-blind, phase 3 trial. Lancet Oncol. 2023 Oct;24(10):1094-1108.
- Agarwal N, Azad AA, Carles J, et al. Talazoparib plus enzalutamide in men with first-line metastatic castration-resistant prostate cancer (TALAPRO-2): A randomized, placebo-controlled, phase 3 trial. Lancet. 2023 Jul 22;402(10398):291-303.
- Chi KN, Rathkopf D, Smith MR, et al. Niraparib and abiraterone acetate for metastatic castration-resistant prostate cancer. J Clin Oncol. 2023 Jun 20;41(18):3339-3351.
- Ryan CJ, Smith MR, de Bono JS, et al. Abiraterone in metastatic prostate cancer without previous chemotherapy. N Engl J Med. 2013;368(2):138-148.
- Beer TM, Armstrong AJ, Rathkopf DE, et al. Enzalutamide in metastatic prostate cancer before chemotherapy. N Engl J Med 2014;371(5):424-433.
- Tombal B, Choudhury A, Saad F, et al. Enzalutamide plus radium-223 in metastatic castration-resistant prostate cancer: results of the EORTC 1333/PEACE-3 trial. Ann Oncol. 2025 Sep;36(9):1058-1067.