(UroToday.com) The 2026 AUA annual meeting featured the International Prostate Forum and a presentation by Dr. Kelvin Moses discussing toxicities and adverse events, and what to know for metastatic hormone sensitive prostate cancer (mHSPC) treatment intensification. Dr. Moses started his presentation by emphasizing that early intensification of treatment for eligible mHSPC patients improves radiographic progression free survival and overall survival. However, with the efficacy gains of triplets (ADT + docetaxel + androgen receptor pathway inhibitor) versus doublets (ADT + androgen receptor pathway inhibitor), there is added toxicity for the patient.
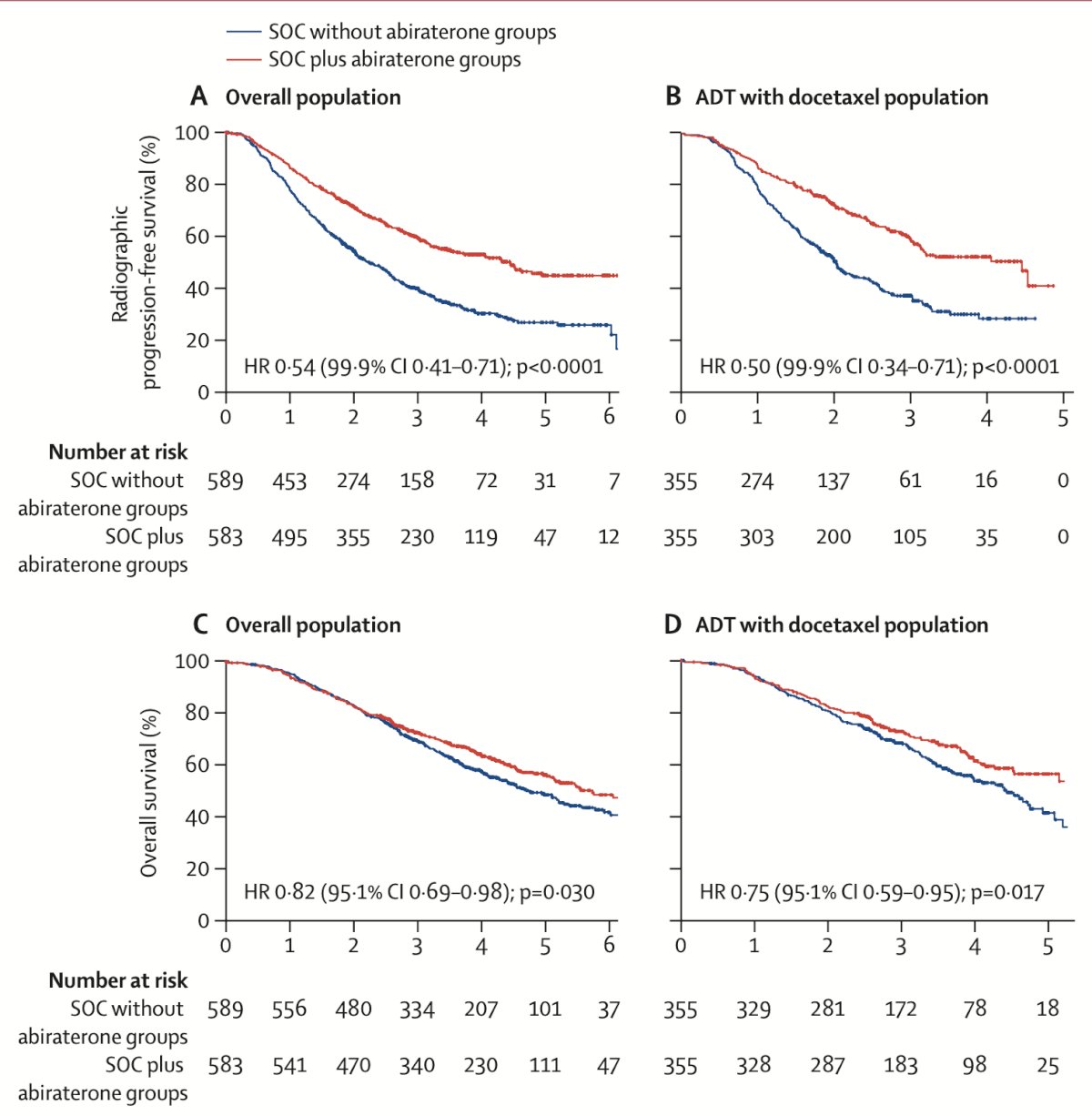
PEACE-11 was an open label, 2x2, phase III randomized trial of men with de novo mHSPC randomized 1:1:1:1 to standard of care (ADT +/- docetaxel) versus standard of care +/- radiotherapy versus standard of care + abiraterone versus standard of care + abiraterone + radiotherapy. Patients assigned to receive abiraterone had longer radiographic progression free survival (HR 0.54, 99.9% CI 0.41-0.71, p < 0.0001) and overall survival (HR 0.82, 95.1% CI 0.69-0.98, p = 0.030) than patients who did not receive abiraterone:
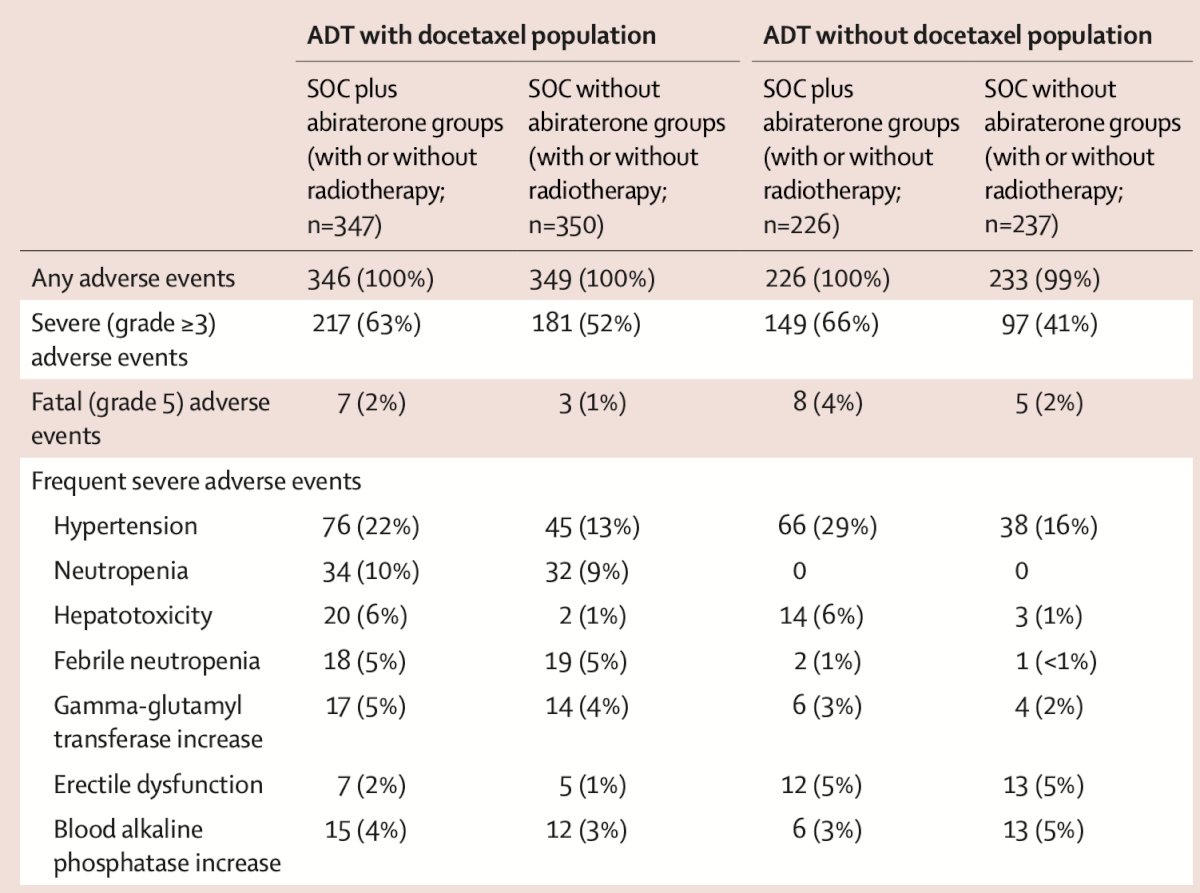
Grade 3 or worse adverse events occurred in 63% of patients who received abiraterone compared to 52% of those who did not receive abiraterone. Hypertension showed the greatest difference between groups:
Dr. Moses provided the following points for mitigating toxicity in the PEACE-1 patient population:
- Hematologic (docetaxel)
- Neutropenia/febrile neutropenia – consider primary or secondary G-CSF
- Mineralocorticoid excess
- Hypertension, hypokalemia, and edema – monitor blood pressure and potassium, and potentially consider eplerenone
- Hepatic
- Transaminase elevations – monitor liver function tests and consider treatment holds or reductions per the label
- Steroid effects
- Fluid retention, glycemic impact – minimize prednisone and provide patient counselling
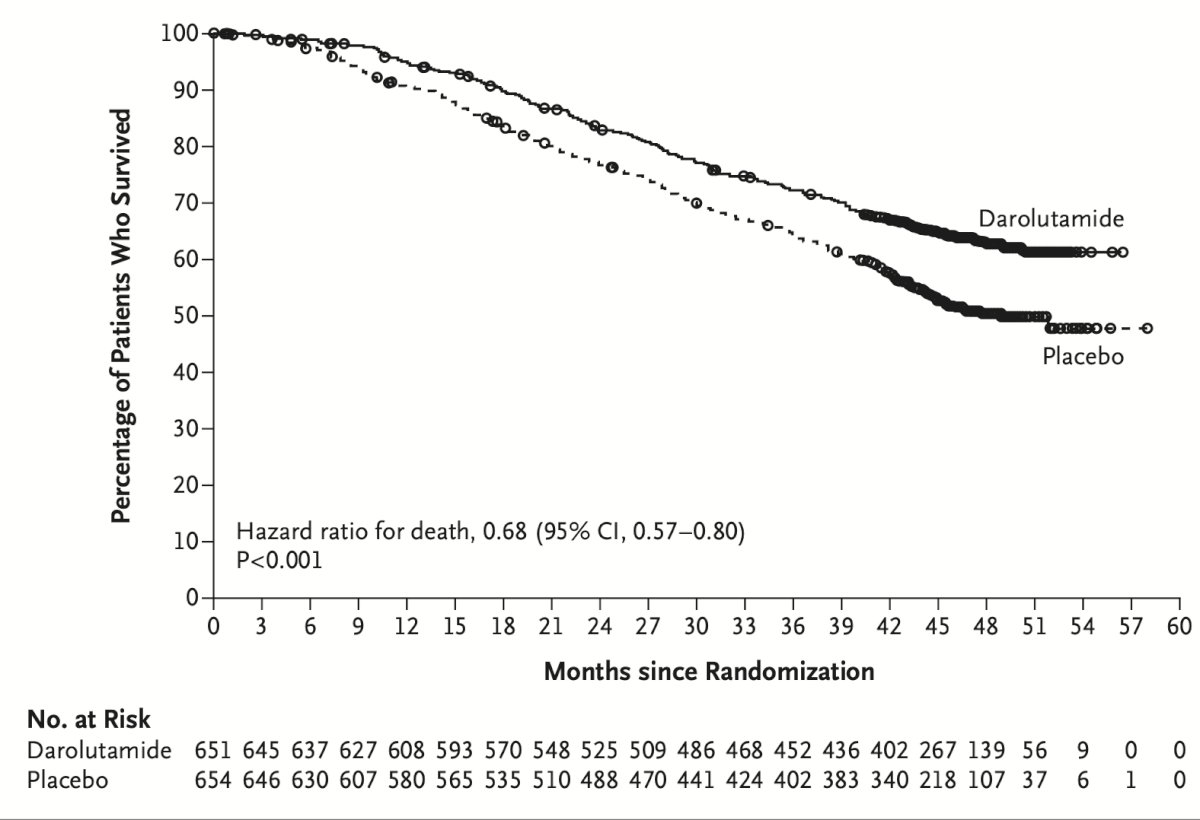
The next study Dr. Moses discussed was the ARASENS trial,2 which was an international phase III trial randomizing men with mHSPC 1:1 to ADT + docetaxel +/- darolutamide, with a primary endpoint of overall survival. This trial noted a 32.5% reduction in risk of death for the darolutamide group (HR 0.68, 95% CI 0.57-0.80, p < 0.001):
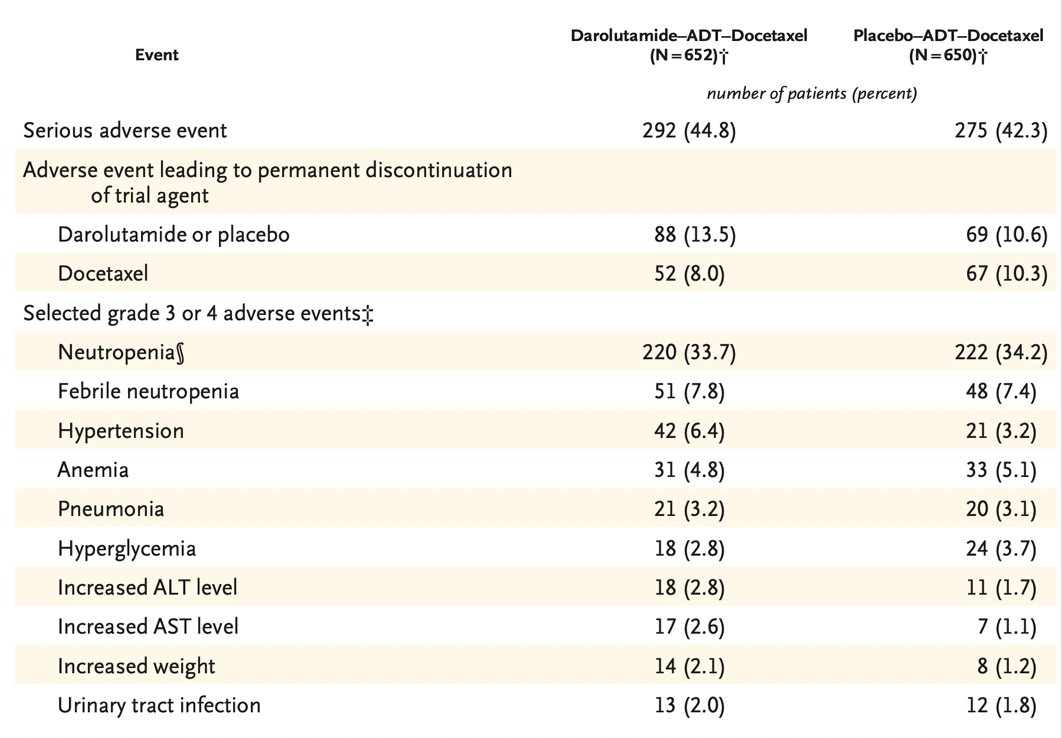
Additionally, there was an improvement in time to mCRPC and time to pain progression noted in the darolutamide arm. The frequency of grade 3 or 4 adverse events was 66.1% versus 63.5% in the placebo group. Neutropenia was the most common grade 3-4 adverse event (33.7% versus 34.2%):
Dr. Moses provided the following points for mitigating toxicity in the ARASENS patient population:
- Hematologic
- Darolutamide class adverse events
- Fatigue, rash, hypertension – there is fewer falls and CNS effects versus some of the other androgen receptor pathway inhibitors
- Hepatic/renal
- Dose adjust for severe renal/hepatic impairment – check periodic liver function tests
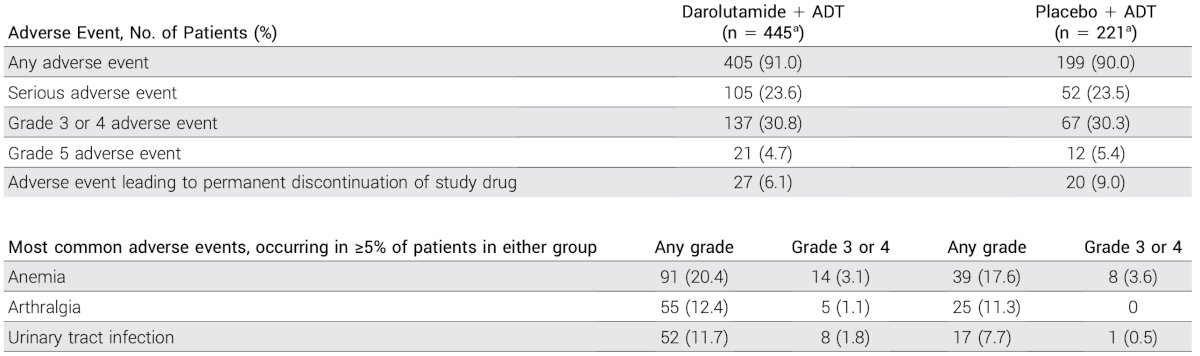
ARANOTE3 was an international phase III trial in men with mHSPC randomized 2:1 to ADT +/- darolutamide, with a primary endpoint of radiographic progression free survival. ARANOTE reported a 46% decreased risk of radiological progression or death (HR 0.54, 95% CI 0.41-0.71) for those receiving darolutamide + ADT versus ADT alone:
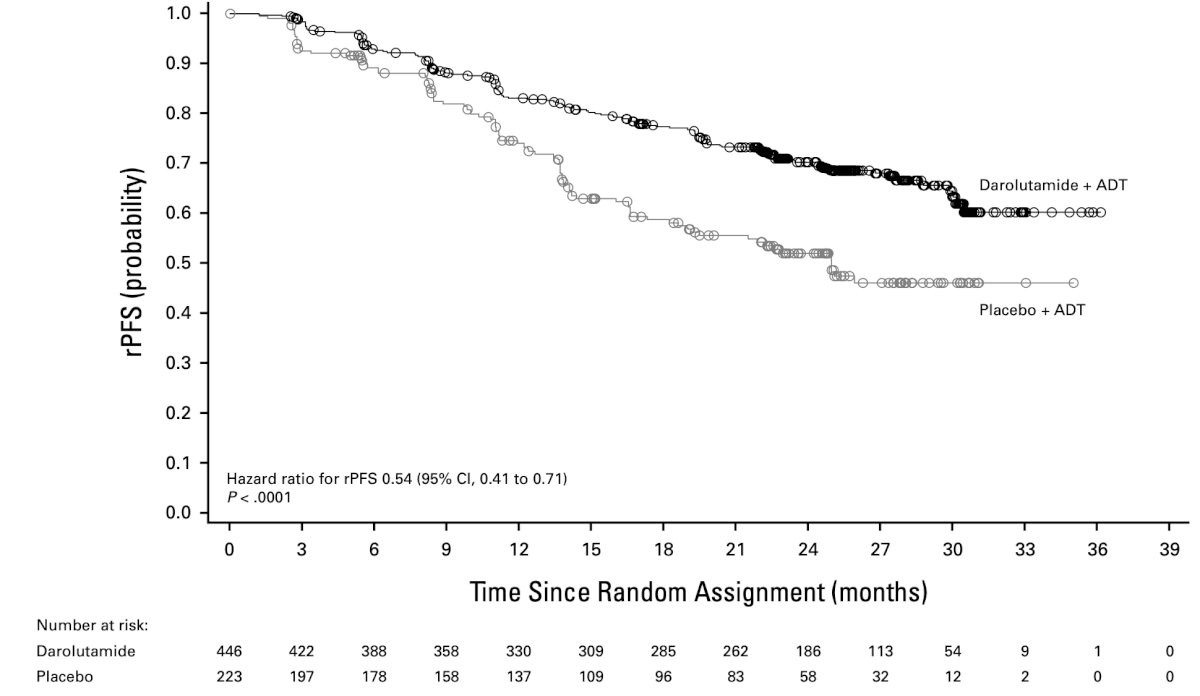
There was also an improved time to mCRPC and time to pain progression, with a trend towards improved overall survival. In ARANOTE, adverse events were comparable between the two groups (~30% versus ~30%), with the most common adverse events being fatigue, hypertension, rash (mostly grade 1-2), with lower discontinuation in the treatment arm. The incidence of fatigue was also lower in patients receiving darolutamide (5.6% versus 8.1%):
For the comparison of PEACE-1, ARASENS, and ARANOTE trial adverse events, Dr. Moses provided the following key points:
- Myelosuppression is highest with docetaxel triplets (PEACE-1 and ARASENS)
- Cardiometabolic adverse events (hypertension, hypokalemia, edema) are higher with abiraterone (PEACE-1)
- Hepatic enzyme elevations: abiraterone > darolutamide, which are manageable with monitoring
- CNS/falls: lower with darolutamide, and it is important to maintain fall-risk checks in frail patients
Dr. Moses concluded his presentation discussing toxicities and adverse events and what to know for mHSPC treatment intensification with his prevention and management playbook:
- Before treatment: baseline CBC, CMP, LFTs, blood pressure check, glucose/lipid check. Vaccinate as necessary and educate the patient and family regarding the importance of febrile neutropenia
- During docetaxel:
- Primary G-CSF if the patient is high risk, or secondary G-CSF after an episode of febrile neutropenia – early antibiotics for fever
- Cycle holds and reductions should be used per ANC/platelet thresholds, while always maintaining infection vigilance
- With abiraterone:
- Blood pressure and potassium monitoring every 2-4 weeks initially – add eplerenone if needed
- LFTs every 2-4 weeks initially and then every 8-12 weeks, and hold doses if they are elevated
- With darolutamide:
- Check drug-drug interactions
- Periodic blood pressure and LFT monitoring
- Dose adjust for patients with severe renal or hepatic impairment
- Counsel with regards to fatigue and falls
Presented by: Kelvin Moses, MD, PhD, Vanderbilt University, Nashville, TN
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the American Urological Association (AUA) 2026 Annual Meeting, Washington, DC, Fri, May 15 – Mon, May 18, 2026.
References:
- Fizazi K, Foulon S, Carles J, Roubaud G, et al. Abiraterone plus prednisone added to androgen deprivation therapy and docetaxel in de novo metastatic castration-sensitive prostate cancer (PEACE-1): A multicentre, open-label, randomized, phase 3 study with a 2 x 2 factorial design. Lancet. 2022 Apr 30;399(10336):1695-1707.
- Smith MR, Hussain M, Saad F, et al. Darolutamide and Survival in Metastatic, Hormone-Sensitive Prostate Cancer. N Engl J Med. 2022 Mar 24;386(12):1132-1142.
- Saad F, Vjaters E, Shore N, et al. Darolutamide in Combination with Androgen-Deprivation Therapy in Patients with Metastatic Hormone-Sensitive Prostate Cancer From the Phase III ARANOTE Trial. J Clin Oncol. 2024 Dec 20;42(36):4271-4281.