(UroToday.com) The 2026 American Urological Association annual meeting featured the International Prostate Forum and a presentation by Dr. Steven Finkelstein discussing radioligand therapy in 2026 and when we should use 177Lu-PSMA-617 and what other options are on the horizon. To illustrate his points, Dr. Finkelstein used a Top 10 approach.
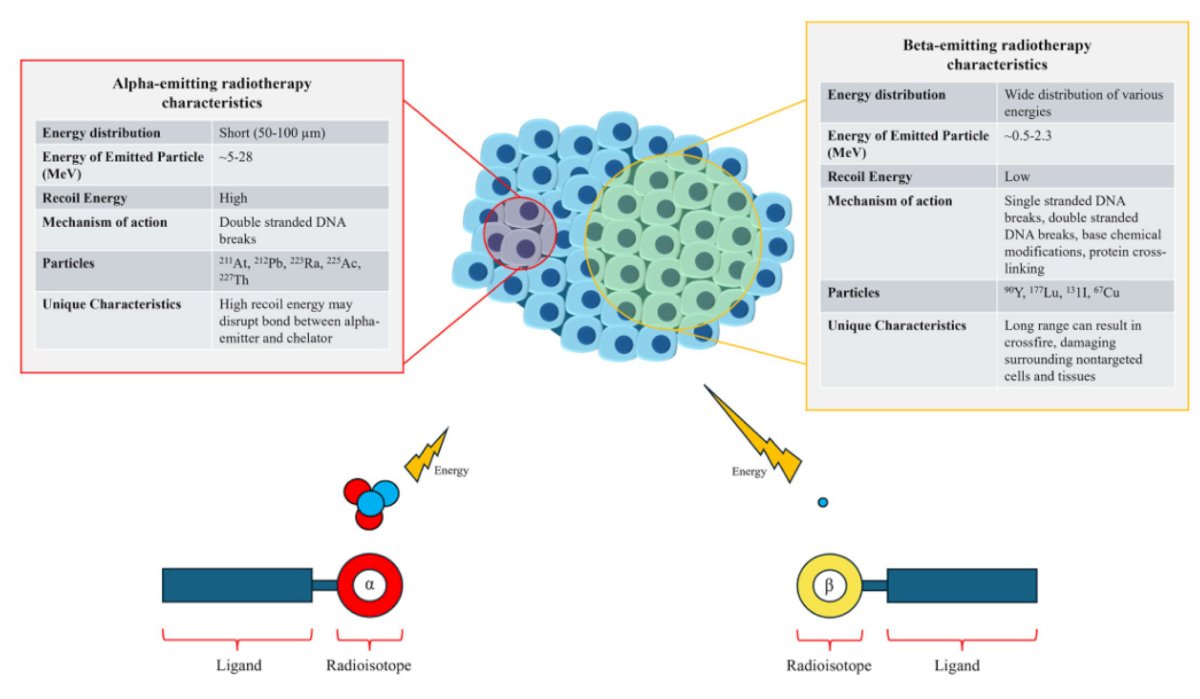
#10: Alpha versus beta emitting theranostics
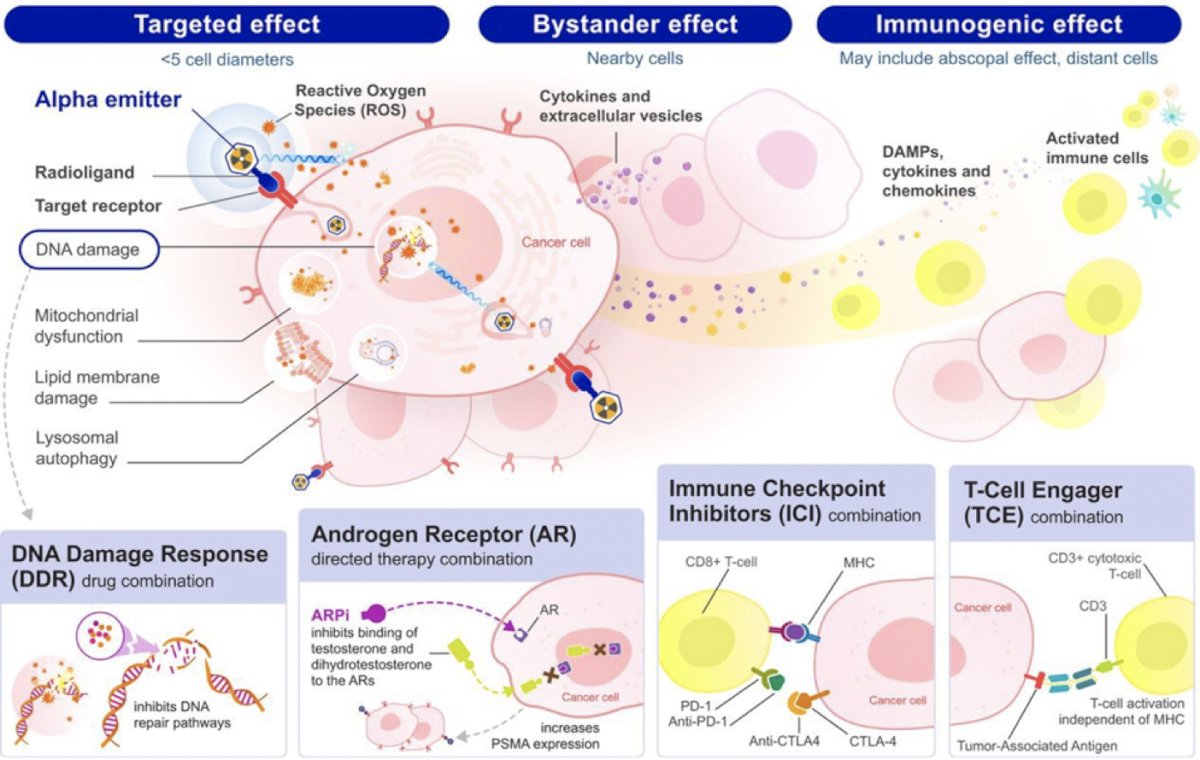
The following figure highlights the characteristics of alpha-emitting versus beta-emitting radiotherapy:
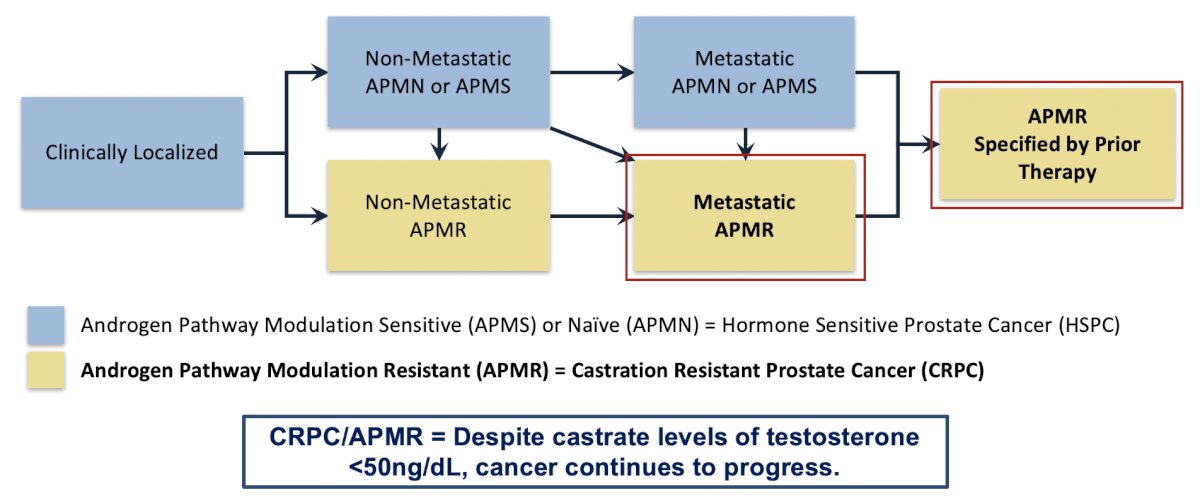
Dr. Finkelstein emphasized that PCWG4 changes the framework of the disease from an endocrinologic basis to a mechanistic one, which includes no use of the term castration.1 A key milestone is the use of prior androgen receptor-directed therapy (ADT alone or androgen receptor pathway inhibitor alone or doublet or triplet with another drug class, or novel androgen receptor-targeted agent, etc):
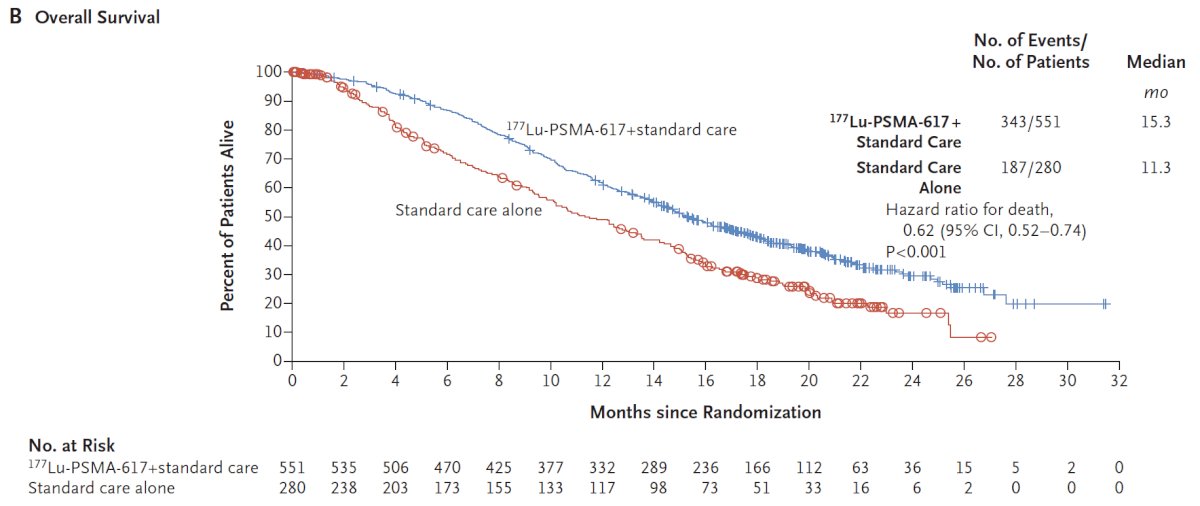
The VISION trial was an international, randomized, open-label phase III study evaluating 177Lu-PSMA-617 in men with PSMA-positive mCRPC who had previously received treatment with a next-generation androgen receptor signaling inhibition (abiraterone, enzalutamide, etc) and one or two prior lines of taxane chemotherapy. Importantly, patients must have had PSMA-positive disease on the basis of a central review of 68Ga-PSMA-11 staging scans. PSMA positivity was defined as uptake greater in metastatic lesions than in the liver. Furthermore, patients could have no PSMA-negative metastatic lesions. Following enrollment, patients were randomized in a 2:1 fashion to receive either 177Lu-PSMA-617 (7.4 GBq every 6 weeks x 6 cycles) plus standard of care or standard of care alone. VISION enrolled 831 patients, and in keeping with the 2:1 randomization schema, 551 patients were allocated to 177Lu-PSMA-617 + standard of care, and 280 were allocated to standard of care only. Over a median study follow-up of 20.9 months, treatment with 177Lu-PSMA-617 + standard of care significantly improved overall survival by a median of 4.0 months (median OS: 15.3 vs 11.3 months; HR 0.62, 95% CI 0.52 to 0.74; p < 0.001, one-sided), compared to standard of care alone, in the overall cohort of all randomized patients:
PSMAfore3 assessed whether we can use 177Lu-PSMA-617 before chemotherapy. Eligible adults for PSMAfore had mCRPC, were candidates for androgen receptor pathway inhibitor change after one progression on prior androgen receptor pathway inhibitor, and had ≥1 PSMA-positive lesion and no exclusionary PSMA-negative lesions by 68Ga-PSMA-11 PET/CT. Candidates for PARP inhibition and patients with prior systemic radiotherapy (<6 months ago), immunotherapy (except sipuleucel-T), or chemotherapy (except [neo]adjuvant >12 months ago) were ineligible. Dr. Finkelstein noted several characteristics of patients enrolled in the PSMAfore trial:
- Median age of 72 years old
- 99% of patients had a performance status of 0-1, with 62% in the 177Lu-PSMA-617 arm having an ECOG status of 0
- 71% were asymptomatic or mildly symptomatic
- Patients in the 177Lu-PSMA-617 arm received subsequent therapies after initial disease progression in PSMAfore
- 47% of these patients were able to receive subsequent chemotherapy
- Additional subsequent treatments included radiotherapy (19%), hormonal therapy (13%), and other anticancer therapies (<5%)
When are patients considered eligible for a delay in chemotherapy? Looking specifically at PSMAfore, there was no defined specific patient criteria needed to delay chemotherapy; it was based on the treating physician’s discretion and clinical experience.
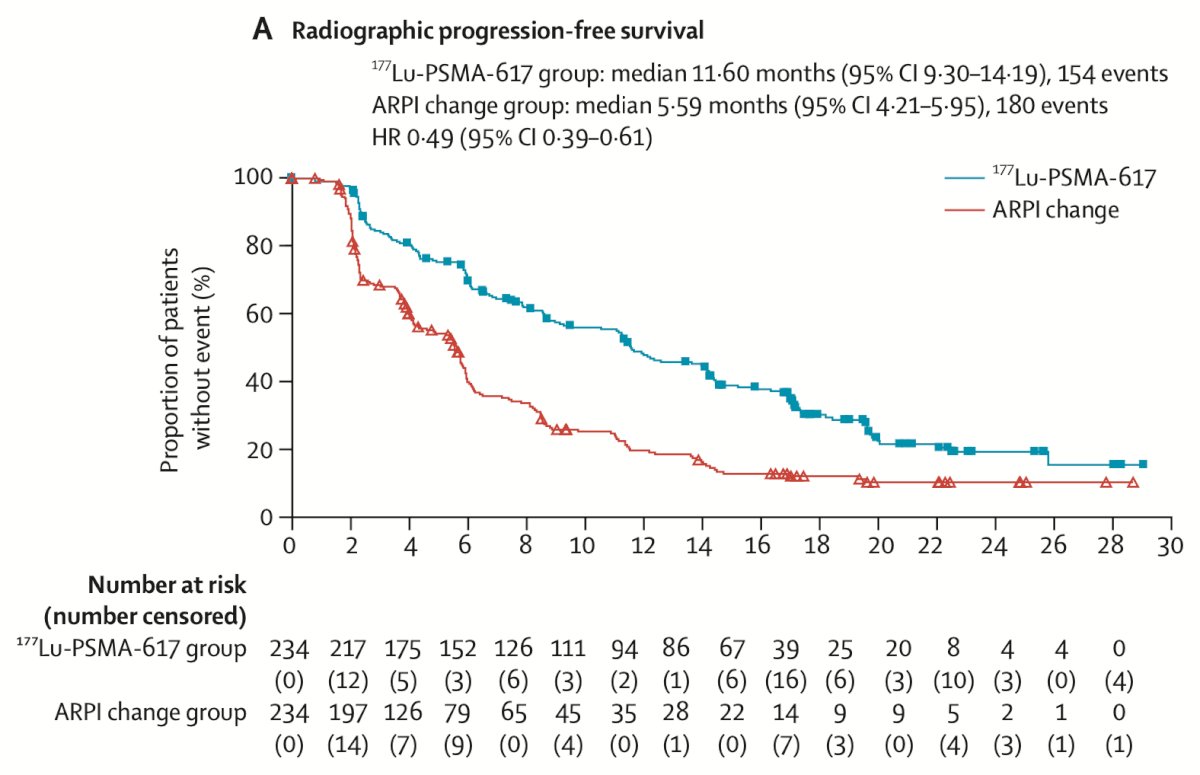
#8: What is the primary endpoint in the PSMAfore trial?
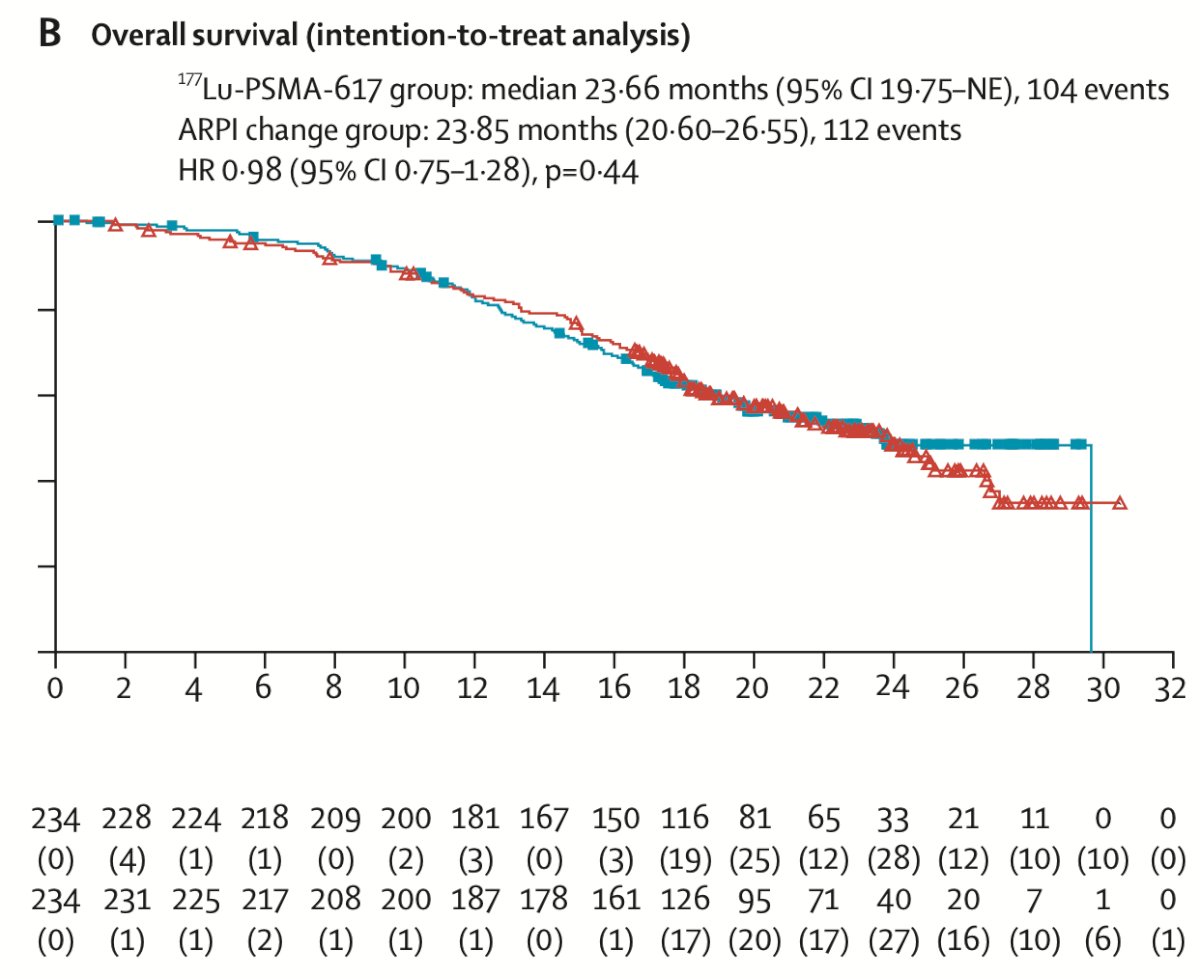
The primary analysis was a pre-planned evaluation of radiographic progression-free survival as the primary end point. At the first data cutoff of October 2, 2022, 177Lu-PSMA-617 demonstrated a median radiographic progression-free survival of 9.3 months versus 5.6 months with a change in androgen receptor pathway inhibitor (HR 0.41, 95% CI, 0.29-0.56). The updated analyses of radiographic progression-free survival could occur as exploratory analyses at the time of the second and third data cutoffs. At the third data cutoff of February 27, 2024, 177Lu-PSMA-617 demonstrated a median radiographic progression-free survival of 11.6 months versus 5.6 months with a change in androgen receptor pathway inhibitor (HR 0.49, 95% CI 0.39-0.61):
For overall survival, there was no difference between the groups (HR 0.98, 95% CI 0.75-1.28), most likely secondary to 57.3% of patients crossing over in the androgen receptor pathway inhibitor change group and crossing over occurring among 77.5% of eligible patients:
The recommended dosage for 177Lu-PSMA-617 is 7.4 GBq (200 mCi) IV every 6 weeks for 6 doses, or until disease progression, or unacceptable toxicity. The dose and frequency of 177Lu-PSMA-617 administration for the PSMAfore trial (7.4 GBq every 6 weeks for 6 cycles) were informed by published clinical studies characterizing the safety, efficacy, and radiation dosimetry profile of 177Lu-PSMA-617. Clinical studies have reported that > 4 cycles of 177Lu-PSMA-617 could be administered safely to maximize the benefit to the patient, and at the time of the third interim analysis of PSMAfore, 63% of patients had received 6 cycles of 177Lu-PSMA-617. In the VISION trial, patients were treated with 177Lu-PSMA-617 7.4 GBq every 6 weeks for 4 cycles. In patients who had evidence of a response, treating physicians could administer an additional 2 cycles (up to 6 cycles in total).
#6: Can patients receive chemotherapy after receiving 177Lu-PSMA-617?
Yes, patients are able to receive subsequent therapies, including chemotherapy, after treatment with 177Lu-PSMA-617. Based on the PSMAfore trial, after discontinuation of 177Lu-PSMA-617, 47% (n = 110/234) received chemotherapy as a post-protocol anticancer therapy. If patients receive 177Lu-PSMA-617, will it affect their bone marrow to make them ineligible for chemotherapy after? To enroll in the PSMAfore trial, patients were required to have an adequate bone marrow reserve, defined as:
• ANC ≥1.5 x 10⁹ /L
• Platelets ≥100 x 10⁹ /L
• Hemoglobin ≥9 g/dL
In the PSMAfore, bone marrow failure was considered a clinically relevant adverse reaction (<10%) with 177Lu-PSMA-617. The following grade 3 or 4 adverse reactions occurred in patients treated with 177Lu-PSMA-617: anemia (7%), leukopenia (4.4%), neutropenia (3.5%), and thrombocytopenia (2.7%). Myelosuppression can be managed by withholding 177Lu-PSMA-617 until improvement (grade 2), withholding or dose reducing (grade ≥3), or permanently discontinuing (recurrent grade ≥3 myelosuppression after 1 dose reduction).
Why are the adverse events with 177Lu-PSMA-617 different between the PSMAfore and VISION trials? The PSMAfore trial evaluated 177Lu-PSMA-617 alone, whereas the VISION trial evaluated 177Lu-PSMA-617 in combination with the best standard of care. The addition of the best standard of care and other factors may lead to the differences in adverse reactions seen from both trials.
#5: Do patients need to have received an androgen receptor pathway inhibitor after mCRPC to receive 177Lu-PSMA-617?Patients can receive 177Lu-PSMA-617 once they have been treated with an androgen receptor pathway inhibitor in their prostate cancer journey, including in the castration sensitive setting. In the PSMAfore trial, 81% of patients in the 177Lu-PSMA-617 arm received an androgen receptor pathway inhibitor in the CRPC setting, and 19% received an androgen receptor pathway inhibitor in the HSPC setting.
#4: Can we use 177Lu-PSMA-617 and an androgen receptor pathway inhibitor together?
In the PSMAfore trial, 177Lu-PSMA-617 was studied against a change of androgen receptor pathway inhibitor, whereas in the VISION trial, 177Lu-PSMA-617 + best standard of care was studied against best standard of care. In the VISION trial, 52.6% of patients in the 177Lu-PSMA-617 + best standard of care arm received concomitant treatment with an androgen receptor pathway inhibitor. Overall survival was an alternate primary endpoint in the VISION trial, and in this trial, 177Lu-PSMA-617 achieved statistically significant overall survival: 38% reduction in the risk of death with 177Lu-PSMA-617 + best standard of care versus best standard of care alone. Median overall survival was 15.3 months with 177Lu-PSMA-617 + best standard of care, versus 11.3 months with best standard of care alone (HR 0.62, 95% CI, 0.52-0.74; p < 0.001)
#3: How long were patients on 177Lu-PSMA-617, and what was the duration of exposure to 177Lu-PSMA-617 in the PSMAfore and VISION trials?
In the PSMAfore trial, the median duration of exposure to 177Lu-PSMA-617 was 8.4 months, with patients receiving a median of 6 doses. In the VISION trial, the median duration of exposure to 177Lu-PSMA-617 was 6.9 months, with patients receiving a median of 5 doses
#2: How should we monitor patients while on 177Lu-PSMA-617?
In the PSMAfore and VISION trials, patients received 177Lu-PSMA-617 until imaging-documented disease progression was detected, an unacceptable level of toxic effects occurred, a determined lack of clinical benefit was recognized, or a prohibited treatment was deemed to be necessary. Imaging-based progression-free survival was defined at the time from randomization to independently centrally reviewed disease progression (defined according to the PCWG3 criteria) or death. In both trials, patients underwent imaging at the following intervals
• Baseline
• Every 8 weeks for the first 24 weeks of treatment
• Every 12 weeks during treatment thereafter, until the end of treatment
Every 3 months during follow-up, PSA levels were also assessed at baseline and before each dose of 177Lu-PSMA-617. In addition, monitoring before and during treatment for potential adverse reactions is advised: hematology (complete blood counts), kidney function (serum creatinine and calculated creatinine clearance), and liver function. Additional tests may be required based on individual patient assessments. Monitoring for and reporting adverse reactions is also advised, and we must also monitor for myelosuppression, renal toxicity, dry mouth, gastrointestinal toxicity, fatigue, electrolyte or metabolic abnormalities, AST or ALT elevation, and other hematologic toxicity.
How should we handle fluctuating PSA levels in some patients after only a few doses? In both the PSMAfore and VISION trials, patients continued to receive treatment until imaging documented disease progression was detected, an unacceptable level of toxic effects occurred, a determined lack of clinical benefit was recognized, or a prohibited treatment was deemed to be necessary. In PSMAfore, PSA progression was a select additional endpoint, and PSA levels were assessed at baseline and consistently throughout treatment. In VISION, PSA progression was a secondary efficacy endpoint, and PSA levels were assessed at baseline and before each dose of 177Lu-PSMA-617. In both trials, investigators monitored PSA and continued treatment with 177Lu-PSMA-617 through early rises of PSA for a minimum of 12 weeks unless there was other evidence of progression, and ignored early rises (before 12 weeks) in determining PSA response.
#1: Key final thoughts on when and how to use 177Lu-PSMA-617
Approximately half of mCRPC patients do not live long enough to receive a second treatment, highlighting the need for earlier use of effective therapies with demonstrated tolerability. Dr. Finkelstein emphasized that 177Lu-PSMA-617 significantly reduced the risk of progression or death by 59% and more than doubled the median radiographic progression free survival versus the change in androgen receptor pathway inhibitor in PSMAfore. So, what’s next?
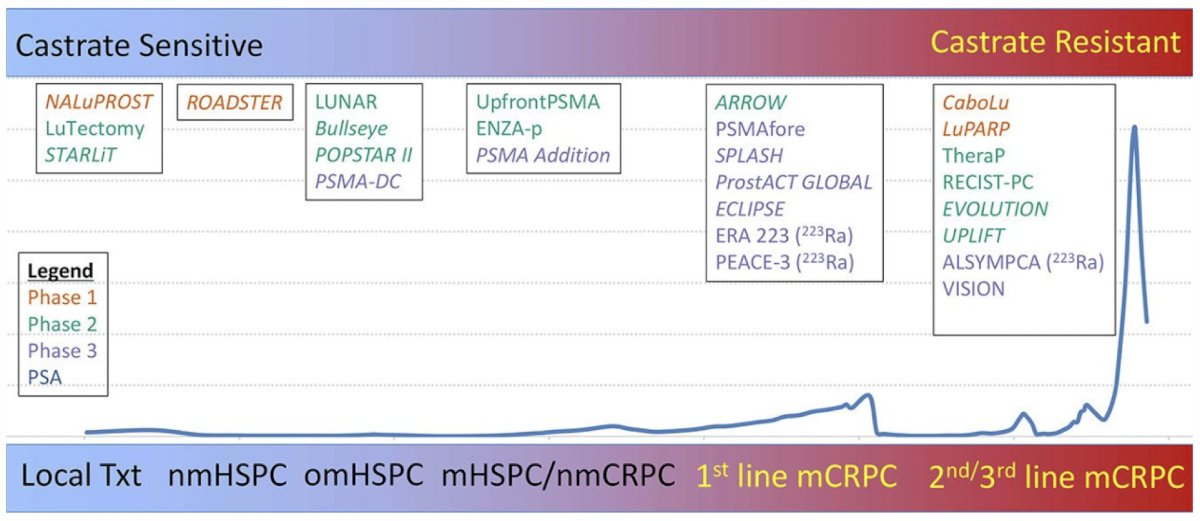
How do we explore or augment radiopharmaceuticals to improve outcomes? Dr. Finkelstein believes this may be a cocktail of radiotherapy, combination therapy with PARP inhibitors/CDK4-6/TKIs, alpha therapy, dose modulation, and immunotherapy:
Dr. Finkelstein concluded his presentation discussing radioligand therapy in 2026 and when we should use 177Lu-PSMA-617 and what other options are on the horizon by emphasizing a multi-disciplinary approach. He and colleagues recently published MD PET 1,4 which highlights this multi-disciplinary framework.
Presented by: Steven Finkelstein, MD, U.S. Urology Partners and Associated Medical Professionals of New York, Syracuse, NY
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the American Urological Association (AUA) 2026 Annual Meeting, Washington, DC, Fri, May 15 – Mon, May 18, 2026.
References:
- Armstrong AJ, Morris MJ, Abida W, et al. Trial design and objectives for patients with prostate cancer: Recommendations from the Prostate Cancer Working Group 4. J Clin Oncol. 2026 Feb 26 [Epub ahead of print].
- Sartor O, de Bono J, Chi KN et al. Lutetium-177-PSMA-617 for Metastatic Castration-Resistant Prostate Cancer. N Engl J Med. 2021 Sep 16;385(12):1091-1103.
- Morris MJ, Castellano D, Herrmann K, et al. 177Lu-PSMA-617 versus a change of androgen receptor pathway inhibitor therapy for taxane-naïve patients with progressive metastatic castration-resistant prostate cancer (PSMAfore): A phase 3, randomized, controlled trial. Lancet 2024 Sep 28;404(10459):1227-1239.
- Morgans AK, Pieczonka CM, Yu EYW, et al. Future opportunities and nuances with the use of PSMA PET in prostate cancer (MD PET 1). Theranostics. 2026;16(11):5816-5829.