(UroToday.com) The 2026 American Urologic Association (AUA) Annual Meeting was host to a prostate cancer clinical trials-in-progress session. Dr. Neal Shore presented CA071-1000 – rechARge, an ongoing phase III trial evaluating BMS-986365, an androgen receptor ligand-directed degrader, versus investigator’s choice in patients with metastatic castration-resistant prostate cancer (mCRPC).
Prostate cancer relies on the androgen receptor (AR) pathway as a key oncogenic driver. AR pathway inhibitors (ARPIs) prolong survival in patients with metastatic prostate cancer in both the castration-sensitive and castration-resistant states. However, ARPIs remain non-curative, and nearly all patients eventually develop disease progression. Overcoming mechanisms of ARPI resistance at the mCRPC stage has emerged as a key clinical challenge.
Significantly, the majority of mCRPC likely remains AR-dependent even if resistant to ARPIs. Mechanisms of AR re-activation include mutations in the AR ligand-binding domain (LBD) and over-expression of the wildtype (WT) receptor.
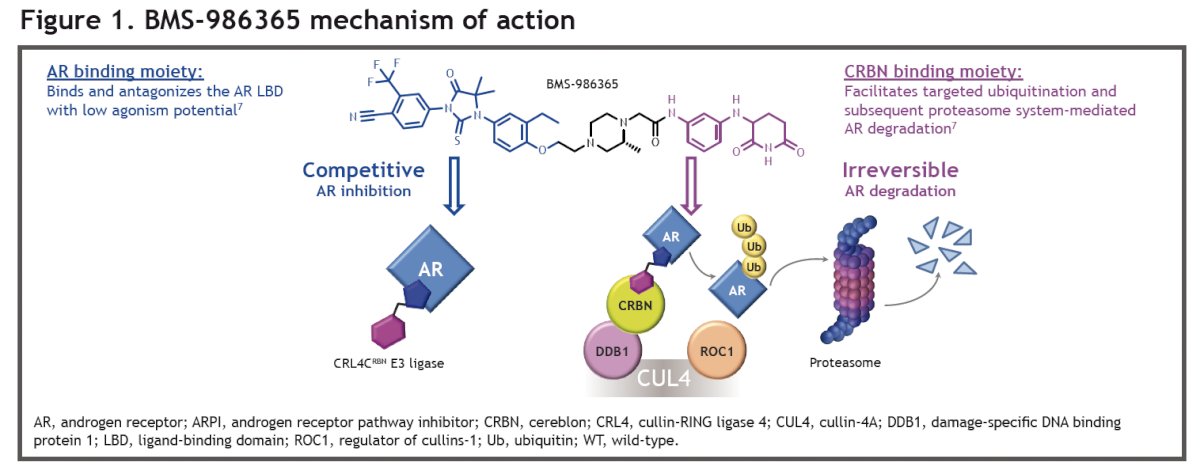
BMS-986365 is a heterobifunctional, orally bioavailable, ligand-directed degrader that targets the AR via a first-in-class dual mechanism of AR degradation and antagonism. BMS-986365 has two binding moieties: an AR binding moiety and a cereblon binding moiety. The binding to cereblon facilitates targeted ubiquitination and subsequent AR degradation. The AR binding moiety attaches to the ligand-binding domain of the AR, resulting in competitive AR inhibition. This dual mechanism of action ensures that any AR not eliminated by degradation remains in an inhibited state.
Results from the first-in-human phase 1 study CC-94676-PCA-001 (NCT04428788) demonstrated that BMS-986365 was well tolerated, had a manageable safety profile, and exhibited anti-tumor activity in heavily pretreated mCRPC patients (including ≥1 prior ARPI).1,2 The maximum tolerated dose was not reached. The most common treatment-related adverse events were prolonged corrected QT interval (QTc) and bradycardia, both of which were asymptomatic. Most cases of prolonged QTc occurred during the first two cycles and resolved with dose modification.
Clinical responses and PSA declines were observed in patients with and without AR gene LBD mutations. In post-hoc analyses, longer radiographic progression-free survival (rPFS) was seen in patients not exposed to prior chemotherapy compared to those with prior chemotherapy, and in those not receiving opioid therapy compared to those receiving opioid therapy
rechARge (NCT06764485), is a global phase III, 2-part, randomized, open-label, adaptive trial evaluating the efficacy and safety of BMS-986365 versus investigator’s choice of ARPI or docetaxel in patients with mCRPC who have failed treatment with 1 prior ARPI.The study design for rechARge is illustrated below:
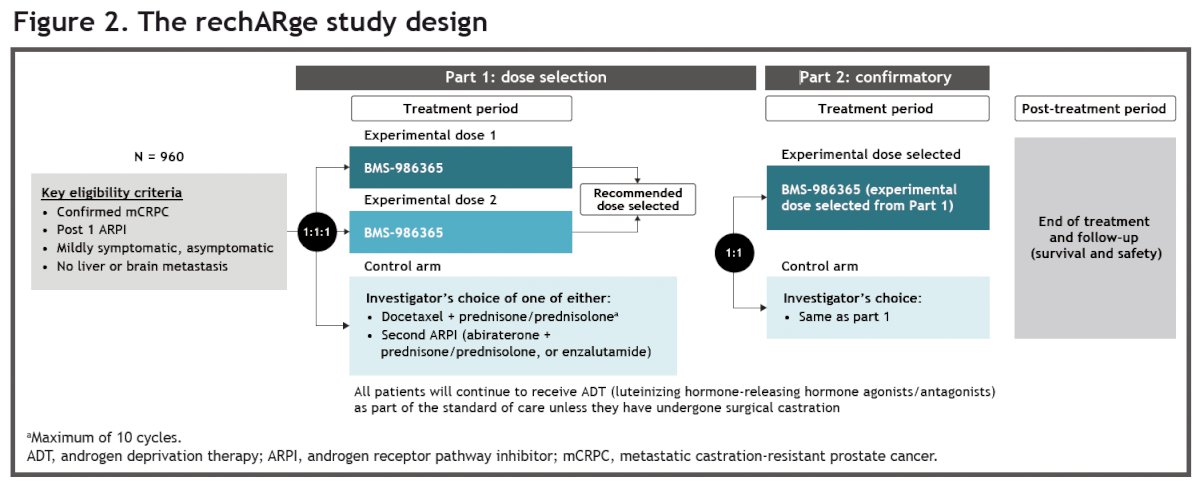
Approximately 960 patients will be randomized in this two-part, phase III trial.
- Part 1 (dose selection): Patients will be randomized 1:1:1 to receive either BMS-986365 400 or 300 mg twice daily every 28 days or investigator’s choice of ARPI (enzalutamide or abiraterone/prednisone or prednisolone) or docetaxel 75 mg/m2 + prednisone/prednisolone up to a maximum of 10 cycles
- Part 2 (confirmatory): Patients will be randomized 1:1 to receive either BMS-986365 (dose determined from Part 1) or investigator’s choice of treatment (same as Part 1)
- Randomization will be stratified by prior type of ARPI and investigator’s treatment choice (second ARPI vs docetaxel)
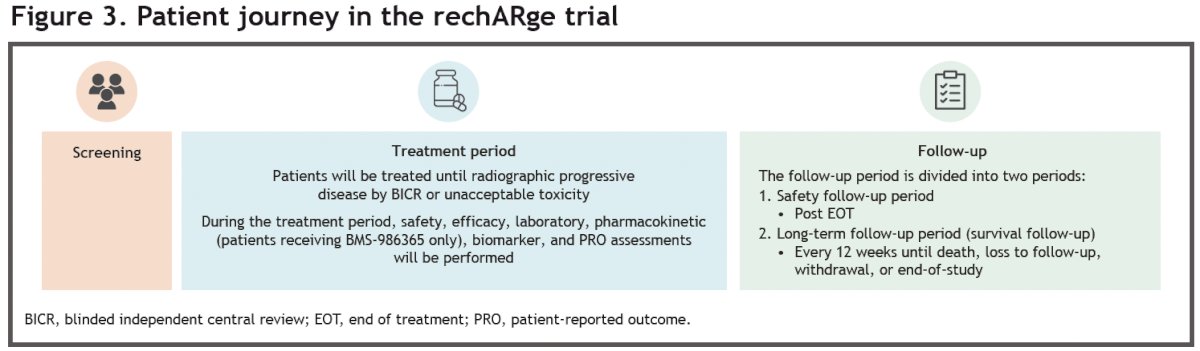
- Patients will be treated until radiographic progressive disease as assessed by blinded independent central review (BICR), unacceptable toxicity, loss to follow-up, or patient withdrawal, except for docetaxel + prednisone/prednisolone, which will be limited to a maximum of 10 cycles; all patients must continue androgen deprivation therapy (ADT) as part of the standard of care
From an eligibility standpoint, patients are required to have confirmed progressive mCRPC, be asymptomatic or mildly symptomatic, and have received no more than 1 previous ARPI and no prior chemotherapy in the mCRPC setting. Patients with brain or liver metastases are not eligible for inclusion.

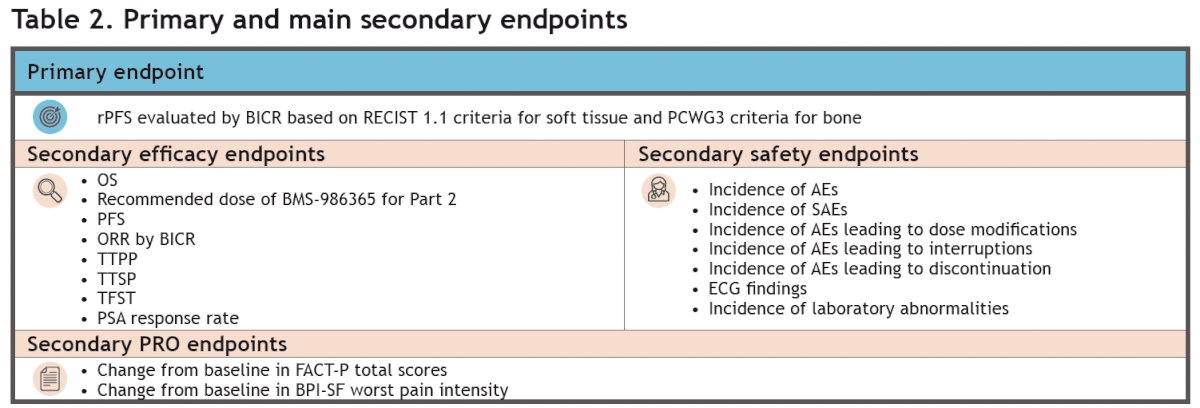
The primary study endpoint is radiographic progression-free survival (rPFS) evaluated by blinded independent central review (BICR), assessed using the Response Evaluation Criteria in Solid Tumors (RECIST) v1.1 criteria for soft tissue and the Prostate Cancer Clinical Trials Working Group 3 (PCWG3) criteria for bone. Other secondary endpoints are shown in the table below.
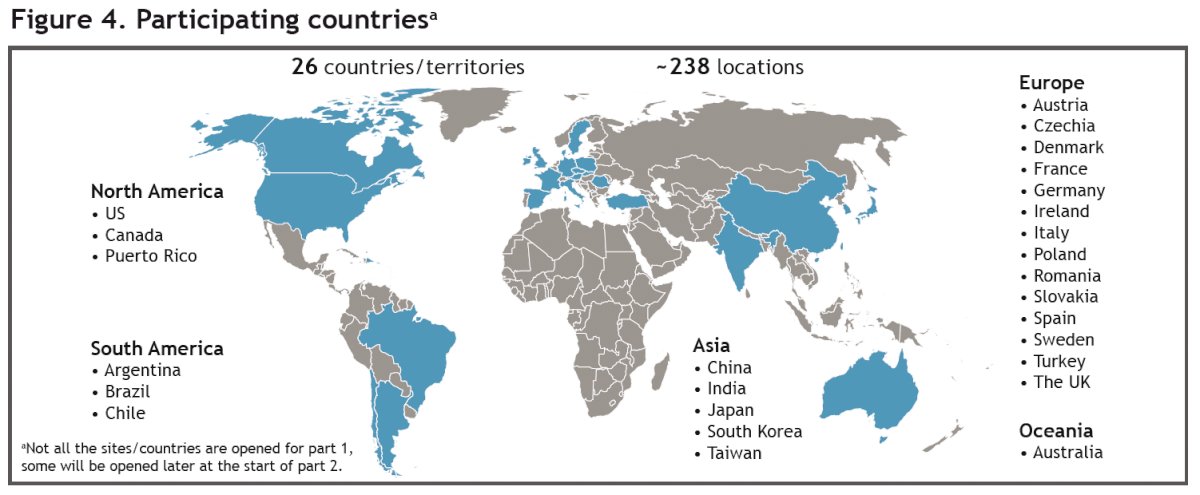
The study is currently recruiting at ~238 sites in 24 countries/territories across North America, Europe, Latin America, and East Asia. The study start date was March 13, 2025. The estimated primary completion date is September 12, 2027. The estimated study completion date is January 19, 2029.
Presented by: Neal Shore, MD, FACS, Urologist, Director, CPI, Carolina Urologic Research Center, Atlantic Urology Clinics, Myrtle Beach, SC
Written by: Rashid K. Sayyid, MD, MSc, Assistant Professor, Urologic Oncologist, Department of Urology at The University of Arizona and Banner University Medical Center, Tucson, AZ – @rksayyid on X during the American Urological Association (AUA) 2026 Annual Meeting, Washington, DC, Fri, May 15 – Mon, May 18, 2026.
References:
- Rathkopf D, Smith MR, Higano CS, et al. Novel hormonal therapies in metastatic castration-resistant prostate cancer: emerging data and future directions. Ann Oncol. 2025;36:76–88.
- Patel MR, Tran B, Garcia JA, et al. BMS-986365 (CC-94676), a dual androgen receptor ligand-directed degrader and antagonist, for heavily pre-treated patients with metastatic castration-resistant prostate cancer: results from additional exploratory analyses. Oral presentation at: American Urological Association (AUA) Annual Meeting; 2025 Apr 26–29; Las Vegas, NV.