(UroToday.com) The American Urological Association's 2026 Annual Meeting, in Washington D.C., was host to the Interactive Poster IP38: Prostate Cancer: Advanced I Session. Dr. Nadine Adriana Friedrich presented interactive poster IP38-04: Comparison of EMBARK and EAU Criteria to Identify High-Risk Patients with Biochemical Recurrence After Radical Prostatectomy.
Dr. Friedrich began by highlighting that the EMBARK trial demonstrated significant improvements in metastasis-free survival and overall survival with enzalutamide plus ADT in patients with high-risk biochemical recurrence (BCR). In EMBARK, high-risk BCR was defined by a PSA >1 ng/mL and a PSA doubling time ≤9 months.1
She noted, however, that in real-world clinical practice, many clinicians more commonly rely on the European Association of Urology (EAU) definition of high-risk BCR, which includes a PSA doubling time ≤12 months or Grade Group 4–5 disease. In this context, the investigators sought to better understand how patients meeting EAU high-risk criteria compare with those enrolled in EMBARK and whether these definitions identify similar patient populations.
To determine whether patients meeting EAU high-risk criteria have similar risks of progression and mortality as those included in EMBARK, the investigators analyzed 1,415 patients without known metastatic disease who received ADT for biochemical recurrence following radical prostatectomy between 1988 and 2019 within the VA SEARCH database.
Patients were stratified into three clinically relevant groups:
- Those meeting both EAU and EMBARK criteria
- Those meeting only EAU high-risk criteria
- Those meeting neither definition.
Importantly, all patients meeting EMBARK criteria also fulfilled EAU high-risk criteria1,2 due to the PSA doubling time requirement. Cumulative incidence of metastasis and prostate cancer-specific mortality were evaluated using Fine and Gray competing risk analyses.
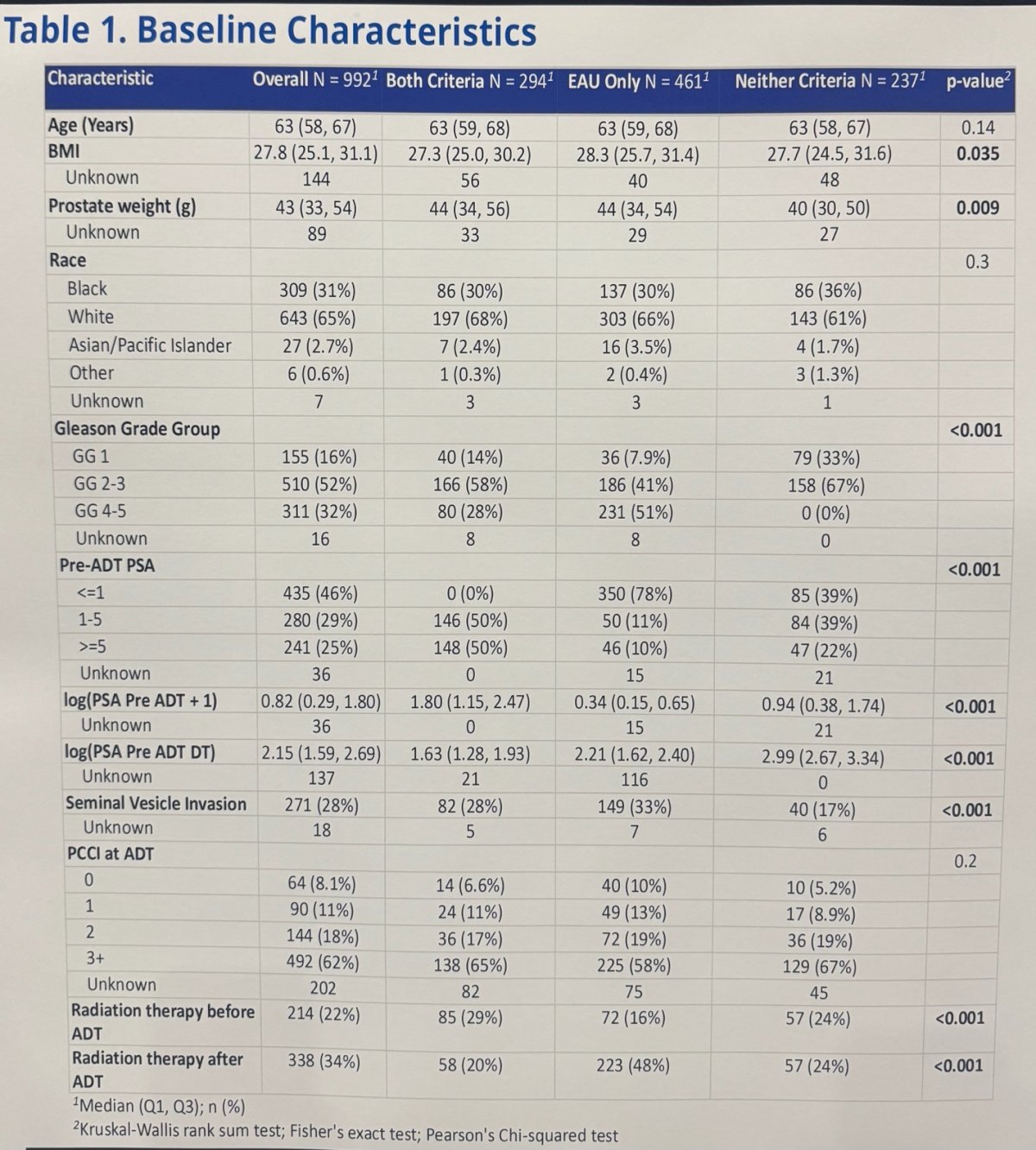
Baseline characteristics varied across the three groups. Patients meeting both EMBARK and EAU criteria had higher pre-ADT PSA values and shorter PSA doubling times, consistent with the EMBARK definition. In contrast, the EAU-only cohort was enriched for adverse pathology, including a higher proportion of GG 4–5 disease and seminal vesicle invasion, despite having lower pre-ADT PSA levels. Patients meeting neither definition had no GG 4–5 disease by definition and generally had longer PSA doubling times.
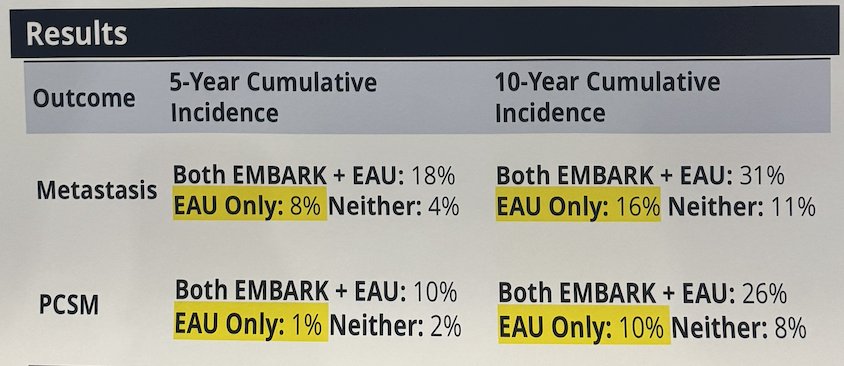
Importantly, patients meeting both EMBARK and EAU criteria demonstrated the highest risk of metastasis and prostate cancer-specific mortality over time. At 5 years, cumulative incidence of metastasis was 18% in the combined EMBARK/EAU group compared with 8% in the EAU-only cohort and 4% in patients meeting neither definition. Similarly, 10-year metastasis rates were 31%, 16%, and 11%, respectively. A similar pattern was observed for prostate cancer-specific mortality, with 10-year PCSM rates of 26% in patients meeting both criteria compared with 10% in the EAU-only group and 8% in patients meeting neither definition.
Lastly, cumulative incidence analyses demonstrated clear separation between risk groups for both metastasis and prostate cancer-specific mortality over time. Patients meeting both EMBARK and EAU high-risk criteria consistently experienced the highest risk of adverse oncologic outcomes, while those meeting only EAU criteria had intermediate risk and patients meeting neither definition had the most favorable outcomes as illustrated in the cumulative incidence of metastasis curves below. Dr. Friedrich noted that these findings support the prognostic value of the stricter EMBARK definition in identifying patients at greatest risk for disease progression and prostate cancer-related death following biochemical recurrence.

Dr. Friedrich concluded her presentation with the following key points:
- Poor oncologic outcomes among patients meeting EAU high-risk criteria appeared to be largely driven by the subset of patients who also fulfilled EMBARK criteria
- The EMBARK definition more precisely identifies patients with truly high-risk biochemical recurrence
- These findings suggest that EMBARK criteria may better identify patients most likely to benefit from earlier treatment intensification with ADT-based strategies
Presented by: Nadine Adriana Friedrich, MD, Postdoctoral Research Fellow, Cedars-Sinai Medical Center, Los Angeles, CA
Written by: Julian Chavarriaga, MD, Clinical Assistant Professor, Urologic Oncologist, Department of Urology at Penn State Health @chavarriagaj on Twitter during the American Urological Association (AUA) 2026 Annual Meeting, Washington, DC, Fri, May 15 – Mon, May 18, 2026.
Reference:
- Shore ND, Luz MA, De Giorgi U, Gleave M, Gotto GT, Pieczonka CM, Haas GP, Kim CS, Ramirez-Backhaus M, Rannikko A, Kalac M, Sridharan S, Rosales M, Tang Y, Tutrone RF Jr, Venugopal B, Villers A, Woo HH, Wang F, Freedland SJ. Improved Survival with Enzalutamide in Biochemically Recurrent Prostate Cancer. N Engl J Med. 2026 Feb 5;394(6):563-575. doi: 10.1056/NEJMoa2510310. Epub 2025 Oct 19. PMID: 41124201.
- Van den Broeck T, van den Bergh RCN, Briers E, Cornford P, Cumberbatch M, Tilki D, De Santis M, Fanti S, Fossati N, Gillessen S, Grummet JP, Henry AM, Lardas M, Liew M, Mason M, Moris L, Schoots IG, van der Kwast T, van der Poel H, Wiegel T, Willemse PM, Rouvière O, Lam TB, Mottet N. Biochemical Recurrence in Prostate Cancer: The European Association of Urology Prostate Cancer Guidelines Panel Recommendations. Eur Urol Focus. 2020 Mar 15;6(2):231-234. doi: 10.1016/j.euf.2019.06.004. Epub 2019 Jun 24. PMID: 31248850.