(UroToday.com) The American Urological Association's 2026 Annual Meeting, between May 15 – May 18, 2026 in Washington D.C., was host to the Interactive Poster IP38: Prostate Cancer: Advanced I Session. Dr. Shinro Hata presented interactive poster IP38-14: Dissecting Synergistic vs. Additive Contributions to Survival in the ARASENS Triplet Regimen: A Modeling Analysis
Dr. Hata began by reviewing the evolution of systemic treatment intensification strategies in metastatic hormone-sensitive prostate cancer. He noted that androgen deprivation therapy alone historically represented the standard of care, followed by the introduction of doublet therapy with ADT plus either docetaxel or an ARPI, which demonstrated clear overall survival improvements and became the modern standard treatment approach.
More recently, triplet therapy combining ADT, docetaxel, and an ARPI has demonstrated additional survival gains in selected studies, particularly ARASENS.1 However, Dr. Hata emphasized that an important unanswered question remains whether the observed benefit with triplet therapy reflects true biologic synergy between therapies or simply additive effects of two independently active treatment modalities.
To address this question, the investigators designed a quantitative analysis evaluating whether the survival benefit observed with the ARASENS triplet regimen reflected a synergistic interaction or was instead consistent with additive effects predicted by independent drug activity models.
Overall survival was selected as the primary endpoint, while time to initial subsequent therapy served as a secondary endpoint. Methodologically, the investigators utilized an independent drug action model combined with reconstructed individual patient-level data to estimate whether outcomes with triplet therapy exceeded what would be expected from the independent contributions of docetaxel and ARPI therapy alone.
For the analysis, Kaplan-Meier curves from ARASENS1 and ARANOTE2 were extracted and incorporated into an independent drug action model designed to predict survival outcomes expected from additive therapeutic effects alone. Using this framework, the investigators generated predicted overall survival and time-to-subsequent-therapy probabilities for triplet therapy based on the independent activity of docetaxel and darolutamide combined with ADT.
The investigators then reconstructed individual patient-level data using the Shiny IPDfromKM algorithm and subsequently applied Cox proportional hazards modeling to compare observed versus predicted outcomes. Importantly, outcomes favoring triplet therapy beyond the additive model prediction, defined as a hazard ratio <1.0 with a 95% confidence interval not crossing 1.0, were interpreted as evidence supporting potential therapeutic synergy rather than simple additive effects.

Using this modeling approach, the investigators observed that outcomes with the ARASENS triplet regimen appeared superior to those predicted by additive effects alone. The observed overall survival curve consistently outperformed the expected survival generated by the independent drug action model. Quantitatively, this translated into a hazard ratio of 0.824 (95% CI 0.681–0.998; p=0.047), suggesting approximately an 18% greater survival benefit than would be anticipated if docetaxel and darolutamide were acting independently. According to the investigators’ predefined framework, these findings support the possibility of biologic synergy between the components of triplet therapy rather than purely additive therapeutic effects.

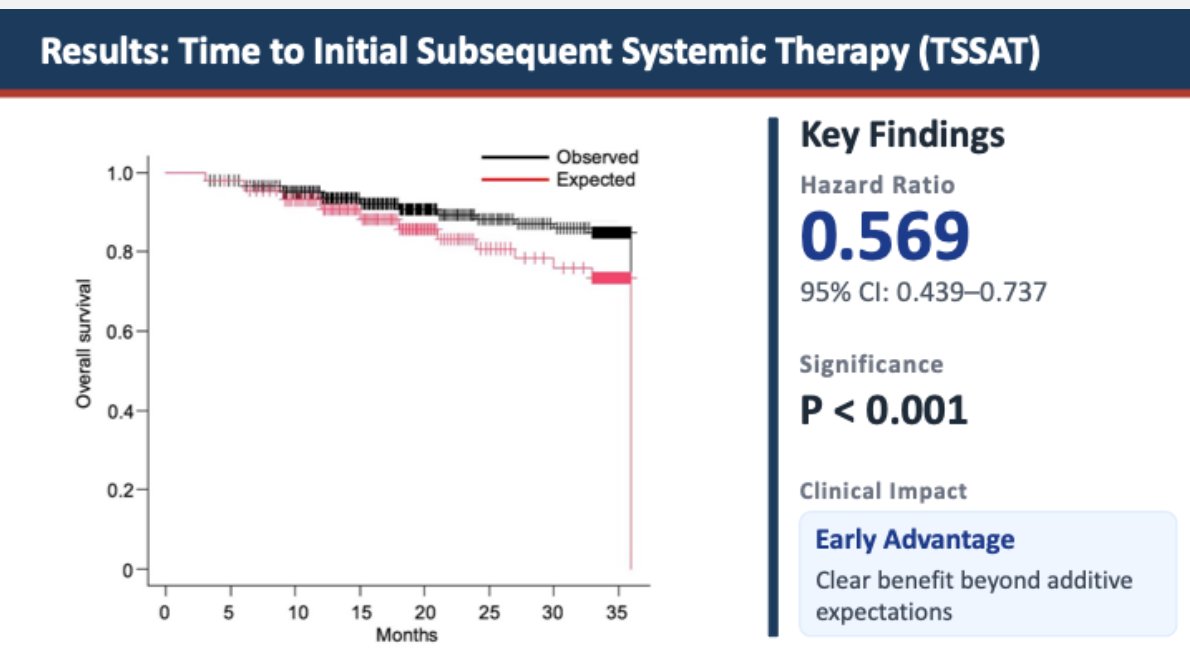
A similar pattern was observed for time to initial subsequent systemic therapy. The observed outcomes with triplet therapy again exceeded those predicted by the independent drug action model, suggesting benefit beyond simple additive effects.
For TSSAT, the hazard ratio was 0.569 (95% CI 0.439–0.737; p<0.001), indicating a substantial delay in the need for subsequent systemic therapy compared with the expected additive model. Dr. Hata emphasized that this early advantage further supported the hypothesis that the ARASENS triplet regimen may provide synergistic therapeutic activity rather than merely combining independent treatment effects.
Dr. Hata next discussed the potential clinical implications of these findings. He suggested that the observed signal of synergy may support upfront simultaneous administration of all three agents rather than a sequential treatment strategy. Additionally, the improvement in time to subsequent systemic therapy was interpreted as evidence of early synergistic therapeutic activity.
From a biological standpoint, Dr. Hata referenced preclinical data suggesting that darolutamide combined with docetaxel may induce synergistic G1 cell-cycle arrest. However, he emphasized that improved biomarker selection will likely be necessary to better identify patients most likely to benefit from triplet therapy approaches.
The investigators also acknowledged several important limitations of the analysis. These included potential confounding from subsequent therapies, heterogeneity across clinical trials, and the exploratory nature of the modeling approach. Dr. Hata further noted that the observed overall survival finding reached only borderline statistical significance (p=0.047), underscoring that these results should primarily be considered hypothesis-generating rather than definitive proof of biologic synergy.
Dr. Hata concluded with the following key messages:
- This analysis provides the first quantitative clinical evidence suggesting potential synergy within the ARASENS triplet regimen beyond simple additive therapeutic effects
- The strongest signal of greater-than-additive benefit was observed for time to subsequent systemic therapy, suggesting an early treatment interaction prior to disease progression
- These findings support the use of upfront simultaneous triplet therapy in appropriately selected patients with mCSPC
- The observed synergistic effect may not be universal across all patients, highlighting the need for biomarker-driven patient selection strategies in future studies
Presented by: Shinro Hata, MD, Department of Urology, Oita University Faculty of Medicine in Yufu, Japan
Written by: Julian Chavarriaga, MD, Clinical Assistant Professor, Urologic Oncologist, Department of Urology at Penn State Health @chavarriagaj on Twitter during the American Urological Association (AUA) 2026 Annual Meeting, Washington, DC, Fri, May 15 – Mon, May 18, 2026.
References:
- Smith MR, Hussain M, Saad F, Fizazi K, Sternberg CN, Crawford ED, Kopyltsov E, Park CH, Alekseev B, Montesa-Pino Á, Ye D, Parnis F, Cruz F, Tammela TLJ, Suzuki H, Utriainen T, Fu C, Uemura M, Méndez-Vidal MJ, Maughan BL, Joensuu H, Thiele S, Li R, Kuss I, Tombal B; ARASENS Trial Investigators. Darolutamide and Survival in Metastatic, Hormone-Sensitive Prostate Cancer. N Engl J Med. 2022 Mar 24;386(12):1132-1142. doi: 10.1056/NEJMoa2119115. Epub 2022 Feb 17. PMID: 35179323; PMCID: PMC9844551.
- Saad F, Vjaters E, Shore N, Olmos D, Xing N, Pereira de Santana Gomes AJ, Cesar de Andrade Mota A, Salman P, Jievaltas M, Ulys A, Jakubovskis M, Kopyltsov E, Han W, Nevalaita L, Testa I, Le Berre MA, Kuss I, Haresh KP; ARANOTE Study Investigators. Darolutamide in Combination With Androgen-Deprivation Therapy in Patients With Metastatic Hormone-Sensitive Prostate Cancer From the Phase III ARANOTE Trial. J Clin Oncol. 2024 Dec 20;42(36):4271-4281. doi: 10.1200/JCO-24-01798. Epub 2024 Sep 16. PMID: 39279580; PMCID: PMC11654448.