(UroToday.com) The American Urological Association's 2026 Annual Meeting, between May 15 – May 18, 2026 in Washington D.C., was host to the Interactive Poster IP38: Prostate Cancer: Advanced I Session. Dr. Neal D. Shore presented interactive poster IP38-10: Referral from urology to oncology practices for patients with metastatic prostate cancer (mPC) in the real world: a PRostatE Cancer dISease observatION (PRECISION) data platform analysis.
Dr. Shore began by highlighting the rapidly evolving treatment landscape for metastatic prostate cancer, emphasizing that the expanding availability of systemic therapies has significantly changed how these patients are managed in clinical practice. Historically, patients diagnosed with metastatic prostate cancer in urology practices were routinely referred to medical oncology for treatment initiation and longitudinal care.1,2
However, he noted that the growing use of oral systemic therapies, alongside the incorporation of services such as radiotherapy and immunotherapy within urology practices, has expanded the role of urologists in the management of metastatic disease. As a result, determining which patients should be referred to oncology specialists, and at what point in their disease course, has become increasingly complex.1,2
Despite these changes, Dr. Shore emphasized that limited data exist regarding real-world referral patterns for patients with metastatic prostate cancer. Accordingly, the investigators sought to evaluate referral practices among patients diagnosed with metastatic prostate cancer in community urology settings across the United States.
This was a retrospective observational study utilizing data from the PRECISION data platform, a harmonized real-world dataset integrating electronic health records, registries, and claims data from patients with advanced prostate cancer treated across multiple clinical settings in the United States.
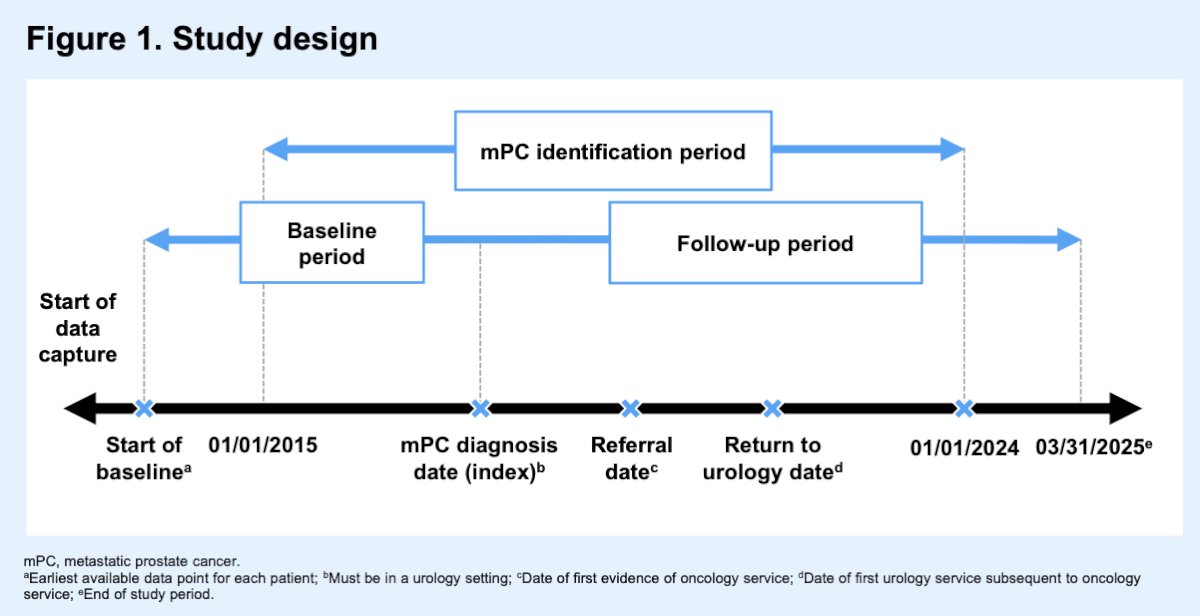
The investigators included men aged ≥18 years diagnosed with metastatic prostate cancer in community urology practices between January 1, 2015, and January 1, 2024. As illustrated in the study schema, the date of metastatic prostate cancer diagnosis served as the index date, followed by longitudinal assessment of referrals to oncology services and subsequent return to urology care when applicable. Separate subgroup analyses were also performed for patients with metastatic hormone-sensitive prostate cancer and metastatic castration-resistant prostate cancer, using the date of mHSPC or mCRPC diagnosis as the subgroup-specific index date. The study design is shown below.
The primary objective of the study was to characterize referral patterns between urology and oncology providers. Referral rates were analyzed descriptively, while cumulative incidence curves were used to evaluate time from diagnosis to referral. The investigators additionally characterized demographic and treatment-related features of referred patients, including treatment patterns before and after oncology referral. Finally, referred and non-referred patients were compared using nested case-control and propensity-score matched analyses to better understand factors associated with referral practices in real-world community settings.
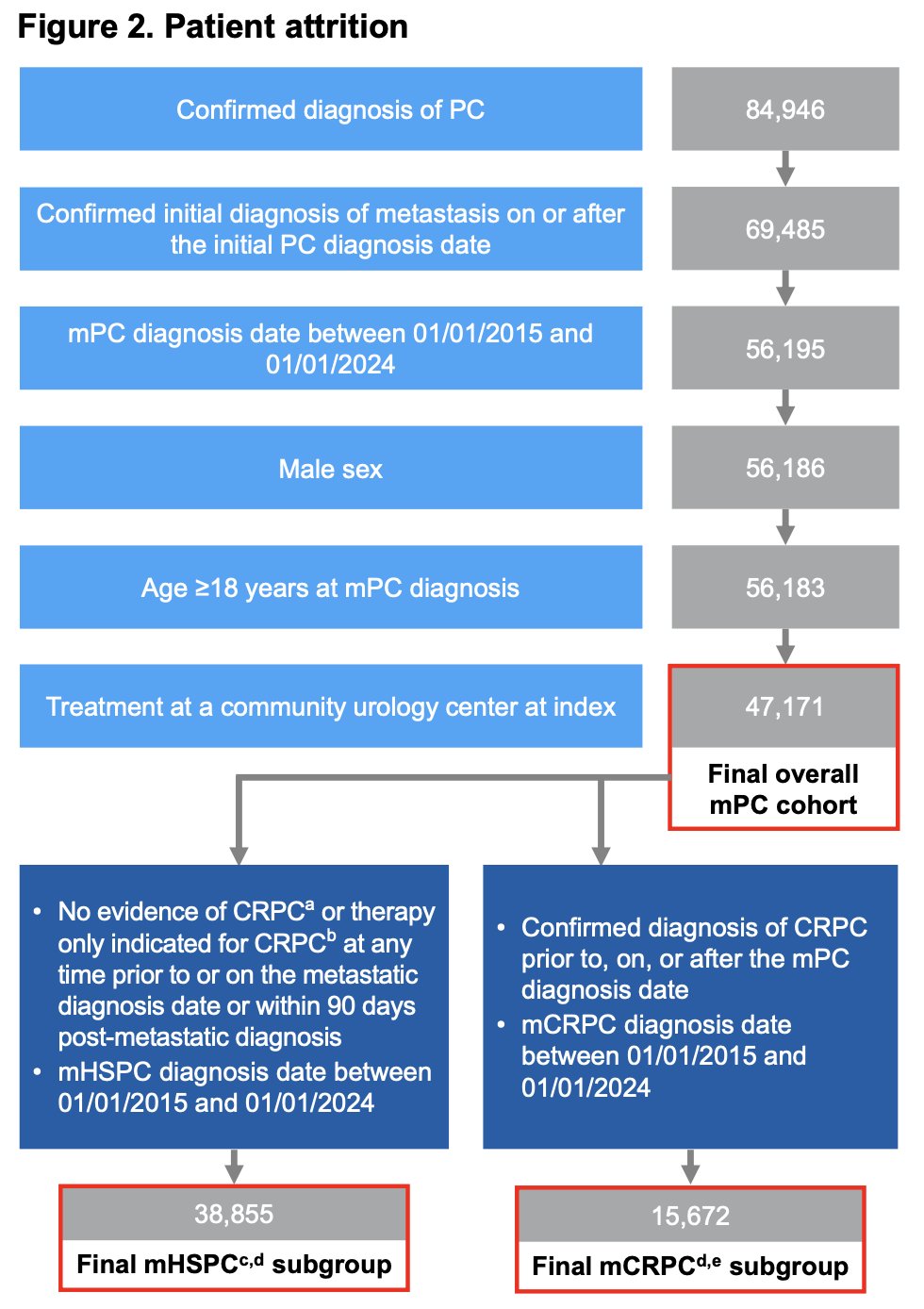
From an initial population of nearly 85,000 patients with confirmed prostate cancer, the investigators identified 47,171 men with metastatic prostate cancer treated in community urology practices who met eligibility criteria for the final overall study cohort. Among these patients, subgroup analyses identified 38,855 patients with metastatic hormone-sensitive prostate cancer and 15,672 patients with metastatic castration-resistant prostate cancer. The mHSPC subgroup included patients without evidence of CRPC or CRPC-directed therapy near the time of metastatic diagnosis, whereas the mCRPC subgroup included patients with confirmed CRPC diagnosed before, at, or after metastatic prostate cancer diagnosis.
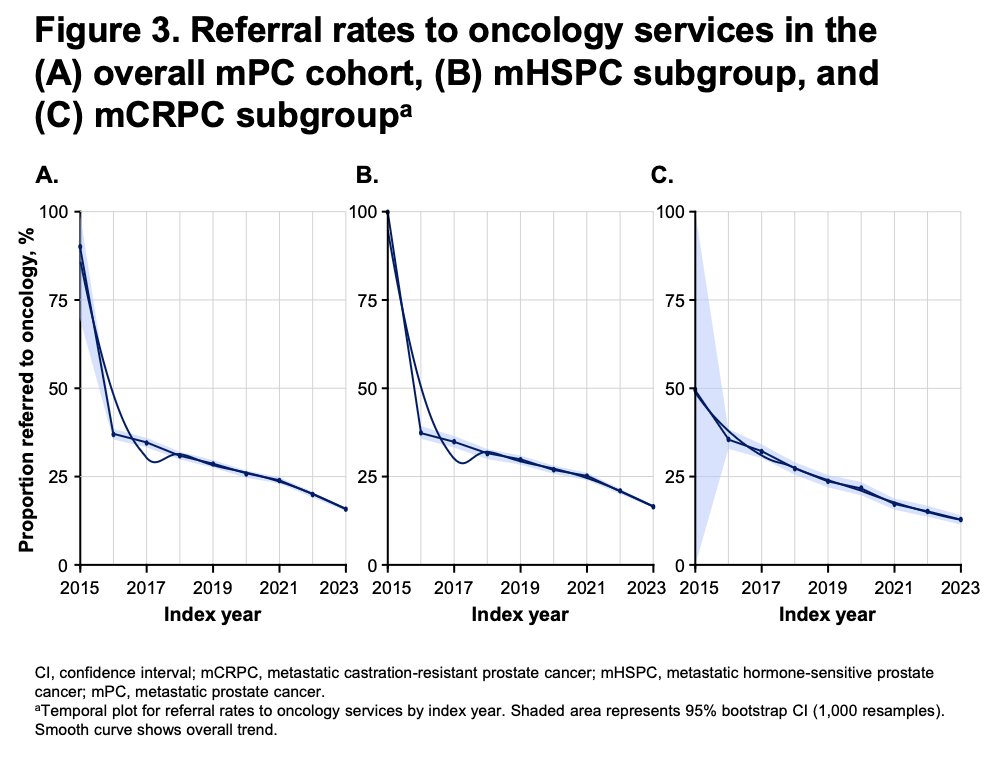
One of the most notable findings from the study was the progressive decline in referrals from urology to oncology services over time across all metastatic prostate cancer cohorts. In the overall metastatic prostate cancer population, referral rates decreased from 37.0% in 2016 to 15.8% in 2023, with an overall referral rate of 24.9% corresponding to 11,732 patients. A similar trend was observed in the metastatic hormone-sensitive prostate cancer subgroup, where referral rates fell from 37.2% in 2016 to 16.2% in 2023, with an overall referral rate of 25.0%. Interestingly, patients with metastatic castration-resistant prostate cancer consistently demonstrated the lowest referral rates throughout the study period. In this cohort, referrals declined from 35.8% in 2016 to 13.0% in 2023, with an overall referral rate of 22.1%.
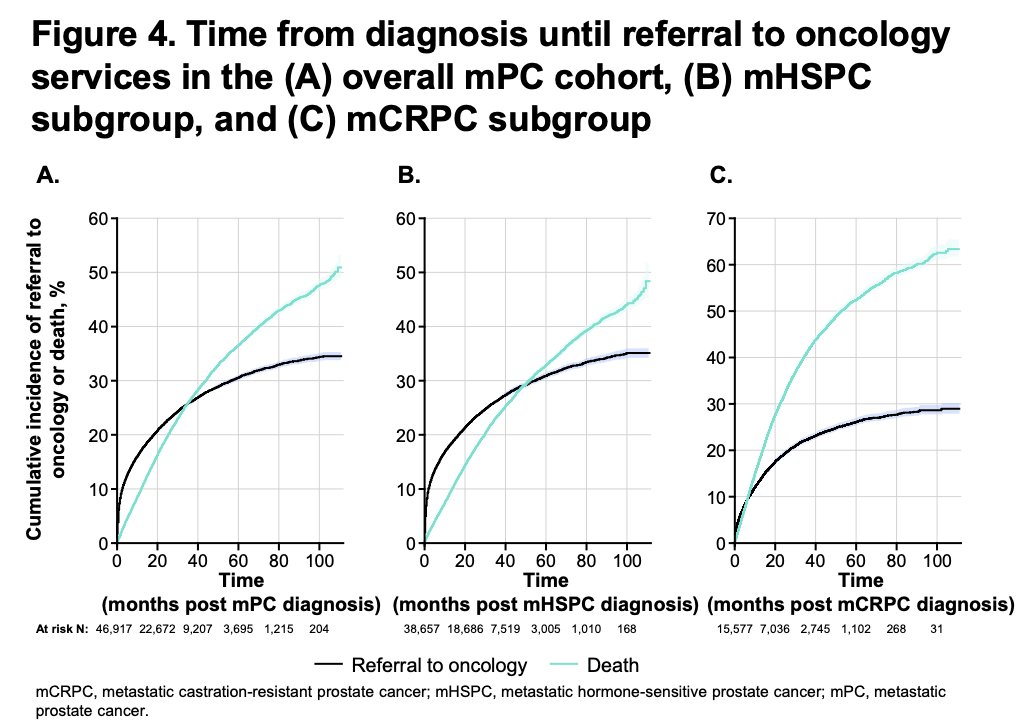
Time-to-referral analyses further demonstrated the relatively low utilization of oncology referrals across all metastatic prostate cancer groups. Median time from diagnosis to referral was not reached, reflecting the low cumulative incidence of referral over longitudinal follow-up.
In the overall metastatic prostate cancer cohort, only 17.2% of patients had been referred to oncology services by 12 months following diagnosis, increasing gradually to 30.5% by 60 months. Notably, the cumulative incidence curves demonstrated that after approximately three years from diagnosis, patients became more likely to die than to be referred to oncology care.
A similar pattern was observed among patients with metastatic hormone-sensitive prostate cancer, where 17.9% were referred by 12 months and 31.0% by 60 months. Referral rates were even lower in the metastatic castration-resistant prostate cancer subgroup, with only 13.1% referred by 12 months and 25.9% by 60 months. In this cohort, patients became more likely to die than undergo oncology referral within the first year following diagnosis.
Interestingly, among patients who were referred to oncology services, return rates to urology practices remained high and remarkably consistent across disease states. The annual return rate to urology centers was 53.2% in the overall metastatic prostate cancer cohort, 52.8% among patients with metastatic hormone-sensitive disease, and 53.5% in the metastatic castration-resistant subgroup, suggesting a substantial degree of shared-care management between oncology and urology providers. Importantly, patients generally transitioned back to urologic care rapidly, with a median time to return of less than one month following oncology referral. By 60 months, more than 80% of referred patients had returned to urology practices, highlighting the ongoing and central role of urologists in the longitudinal management of metastatic prostate cancer in real-world community settings.
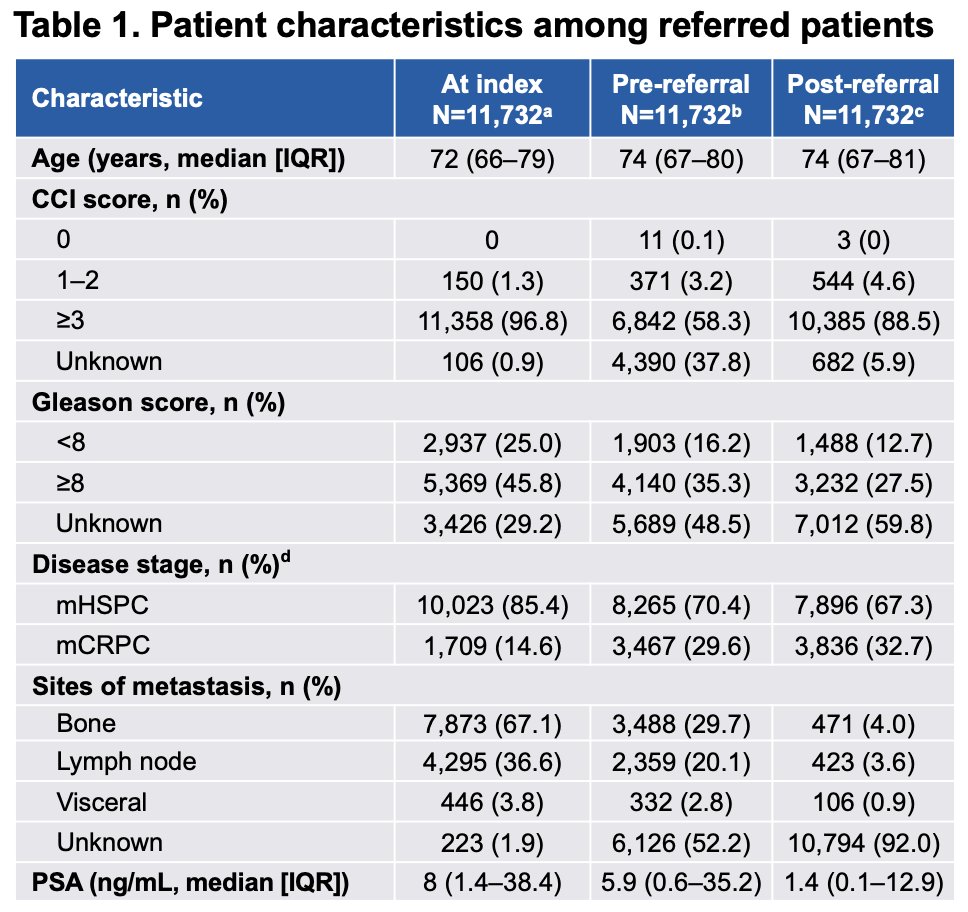
Dr. Shore also reviewed the characteristics of referred patients at the time of metastatic prostate cancer diagnosis, as well as before and after referral to oncology services. The referred population was generally older, with a median age in the mid-70s, and most patients had substantial comorbidity burden, with the majority demonstrating a Charlson Comorbidity Index ≥3. Most referred patients initially had metastatic hormone-sensitive prostate cancer, although the proportion of patients with mCRPC increased over time following referral. Bone metastases represented the most common metastatic site at baseline.
Importantly, Dr. Shore highlighted that median PSA levels were notably lower following oncology referral compared with pre-referral measurements. Median PSA declined from 5.9 ng/mL prior to referral to 1.4 ng/mL post-referral, suggesting that initiation or escalation of systemic therapies within oncology settings was associated with meaningful biochemical responses.
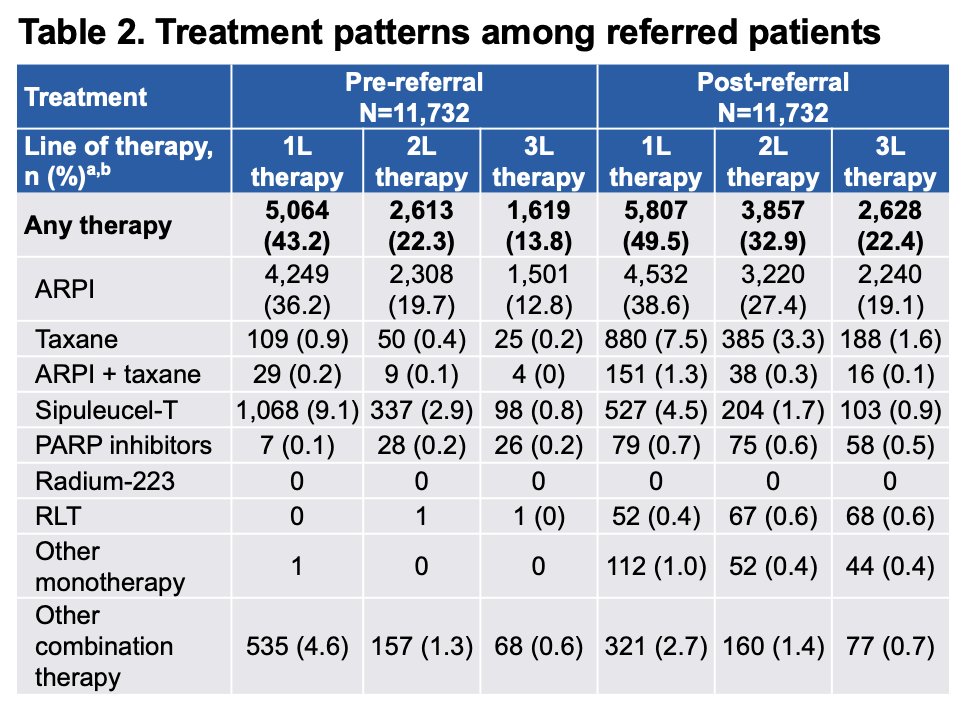
Dr. Shore next discussed treatment patterns before and after referral to oncology services. Among referred patients, overall treatment utilization increased following oncology referral, suggesting broader adoption of systemic therapies after transition to multidisciplinary care. Use of androgen receptor pathway inhibitors remained common both before and after referral. However, referral to oncology was associated with greater utilization of therapies less commonly administered within urology practices, including taxane chemotherapy, PARP inhibitors, and radioligand therapy. Across all treatment lines, taxane use increased substantially from 1.7% prior to referral to 10.8% following referral, while radioligand therapy utilization increased from 0.1% to 1.8%.
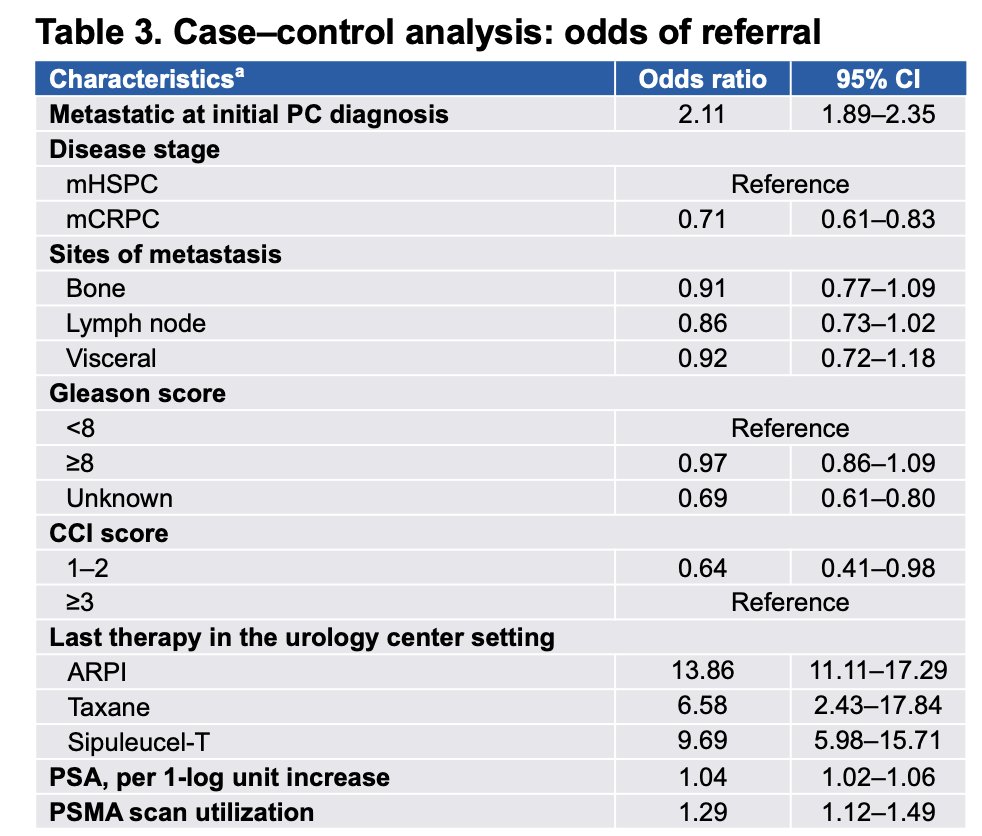
Lastly, the investigators presented matched analyses comparing referred and non-referred patients in order to better understand factors associated with oncology referral and subsequent treatment utilization. In the nested case-control analysis, 6,101 referred patients were matched to 6,101 patients without evidence of oncology referral. Factors associated with higher odds of referral included metastatic disease at the time of initial prostate cancer diagnosis, higher PSA levels, greater Charlson Comorbidity Index scores, and prior PSMA PET utilization. Referral was also strongly associated with receipt of systemic therapies within urology practices, including ARPIs, taxane chemotherapy, and sipuleucel-T.
The investigators additionally performed a propensity-score matched analysis comparing 11,463 referred patients with 11,463 non-referred patients. Interestingly, ARPI utilization was similar between groups across treatment lines. However, referred patients demonstrated greater utilization of taxane chemotherapy and radioligand therapy, further supporting the concept that oncology referral may primarily facilitate access to more advanced or specialized systemic treatment modalities.
Dr. Shore concluded with the following take-home messages:
- Referral rates from community urology practices to oncology services declined substantially over time, despite the expanding therapeutic landscape for metastatic prostate cancer
- Oncology referral was associated with greater utilization of taxanes, PARP inhibitors, and radioligand therapy, as well as meaningful reductions in PSA levels following transition of care
- More than half of the referred patients rapidly returned to urology practices, typically within one month, underscoring the continued central role of urologists in the longitudinal management of metastatic prostate cancer
- These findings highlight the importance of coordinated multidisciplinary care and shared management models between urology and oncology providers
- Better understanding of referral patterns may help identify gaps in care delivery, optimize treatment access, and improve outcomes for patients with both mHSPC and mCRPC
- Additional research evaluating the relationship between referral practices and long-term clinical outcomes is warranted
Presented by: Neal D. Shore, MD, FACS, Director, CPI (Certified Principal Investigator by the Association of Clinical Research Professionals), START Carolinas/Carolina Urologic Research Center, Head of GU Oncology and Radiopharm, START Center for Cancer Research Institute, AUC Urology Specialists, Myrtle Beach, SC
Written by: Julian Chavarriaga, MD, Clinical Assistant Professor, Urologic Oncologist, Department of Urology at Penn State Health @chavarriagaj on Twitter during the American Urological Association (AUA) 2026 Annual Meeting, Washington, DC, Fri, May 15 – Mon, May 18, 2026.
References:
- Ng K, Smith S, Shamash J. Metastatic Hormone-Sensitive Prostate Cancer (mHSPC): Advances and Treatment Strategies in the First-Line Setting. Oncol Ther. 2020 Dec;8(2):209-230. doi: 10.1007/s40487-020-00119-z. Epub 2020 Jun 15. PMID: 32700045; PMCID: PMC7683690.
- Shore ND. Chemotherapy for prostate cancer: when should a urologist refer a patient to a medical oncologist? Prostate Cancer Prostatic Dis. 2013 Mar;16(1):1-6. doi: 10.1038/pcan.2012.23. Epub 2012 Jul 3. PMID: 22751145.