(UroToday.com) The American Urological Association's 2026 Annual Meeting, between May 15 – May 18, 2026, in Washington D.C., was host to the Interactive Poster IP38: Prostate Cancer: Advanced I Session. Dr. Hiroshi Yaegashi presented an interactive poster, IP38-05: Development and clinical implementation of a simple radium-223 non-completion risk calculator for bone-metastatic castration-resistant prostate cancer.
Dr. Yaegashi highlighted that radium-223 has been shown to prolong overall survival in patients with bone-metastatic castration-resistant prostate cancer. However, he emphasized that early discontinuation of therapy remains a major clinical issue, as failure to complete the planned treatment course may substantially diminish therapeutic benefit. Given this challenge, the investigators aimed to identify pretreatment predictors associated with failure to complete radium-223 therapy and to develop a simple, clinically accessible risk calculator capable of individualized prediction of treatment completion and overall survival. The goal was to support shared decision-making and optimize patient selection in real-world clinical practice.
To address this question, the investigators analyzed 802 patients with bone-metastatic CRPC treated with radium-223 across 84 centers as part of the FRONTIER study. Treatment completion was defined as receipt of all six planned cycles of radium-223. Baseline clinical characteristics, including ECOG performance status and laboratory parameters, were evaluated to identify predictors associated with treatment non-completion.
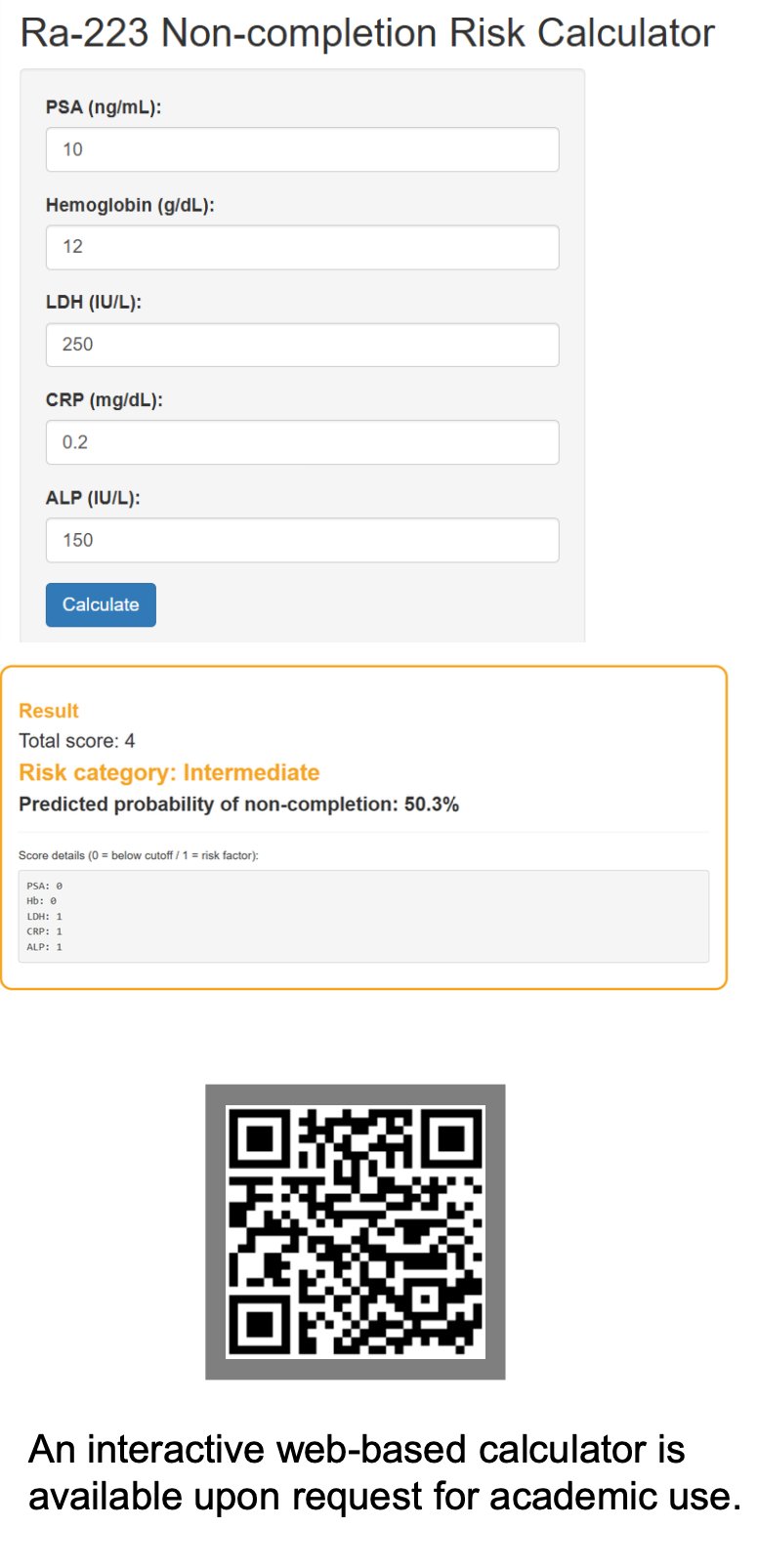
Using univariable and multivariable logistic regression analyses, the investigators identified five independently associated serum biomarkers predictive of treatment discontinuation: PSA, hemoglobin, LDH, alkaline phosphatase, and C-reactive protein. Importantly, variance inflation factor analysis confirmed the absence of significant multicollinearity among variables. Based on weighted β-coefficients, the group developed a simplified 7-point risk scoring system stratifying patients into low (0–2), intermediate (3–4), and high-risk (≥5) categories for non-completion. Kaplan-Meier analyses were subsequently used to evaluate overall survival across risk groups, and the model was internally validated before being incorporated into a web-based clinical risk calculator. An example of the risk calculator is presented below, and the QR code to access it online was presented by Dr. Yaegashi.
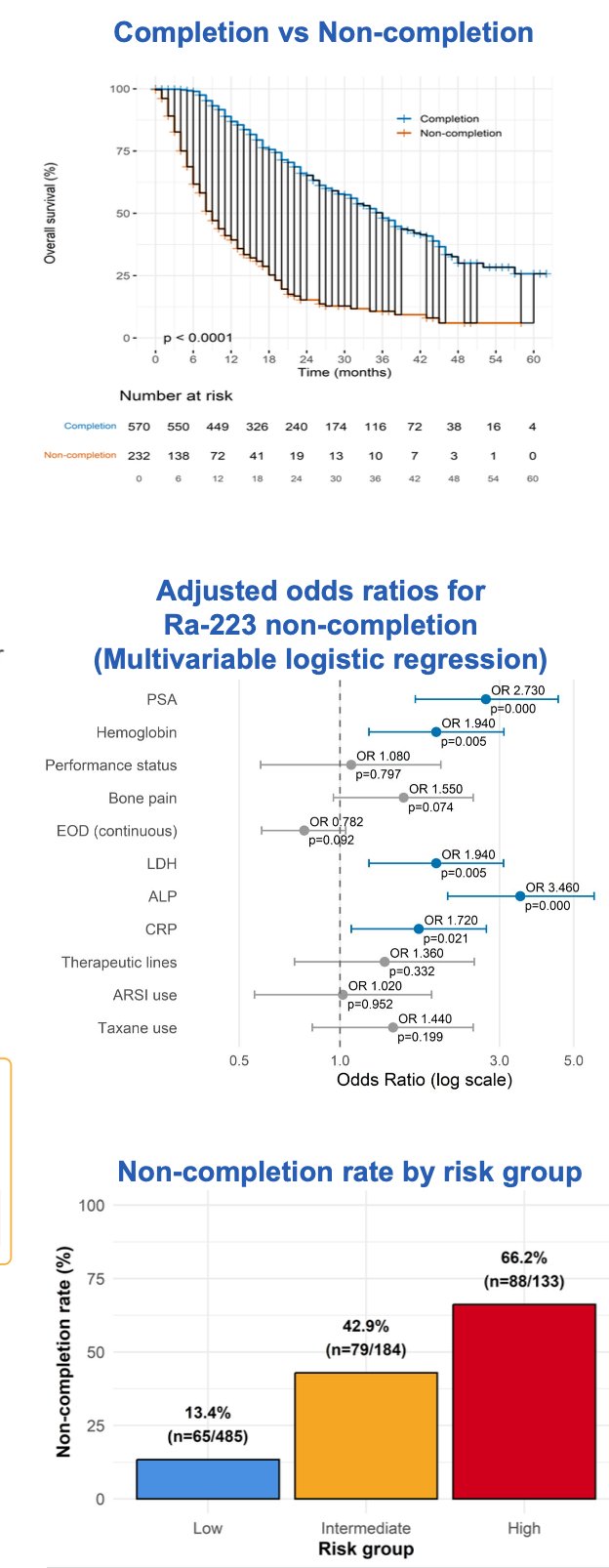
Overall, treatment non-completion occurred in 232 of 802 patients (29%), underscoring the clinical relevance of identifying patients at risk for early discontinuation of radium-223 therapy. On multivariable analysis, five pretreatment serum biomarkers remained independently associated with non-completion: PSA, hemoglobin, LDH, alkaline phosphatase, and C-reactive protein. Among these, elevated ALP demonstrated one of the strongest associations with treatment discontinuation (OR 3.22, 95% CI 2.03–5.10), while elevated PSA, LDH, CRP, and lower hemoglobin levels were also significant predictors.
Importantly, the derived risk score effectively stratified patients according to the likelihood of treatment non-completion. Rates of discontinuation increased substantially across risk groups, occurring in 13.4% of low-risk patients, 42.9% of intermediate-risk patients, and 66.2% of high-risk patients, demonstrating strong discriminatory performance and a significant stepwise trend across categories (Illustrated below).
Notably, the proposed risk model also demonstrated strong prognostic value for overall survival. Median OS differed significantly across risk groups, reaching 37.0 months in the low-risk group, 18.0 months in the intermediate-risk group, and only 9.0 months in the high-risk group (log-rank p<0.0001). As shown in the Kaplan-Meier curves, survival outcomes separated early and remained consistently distinct over time across all three categories.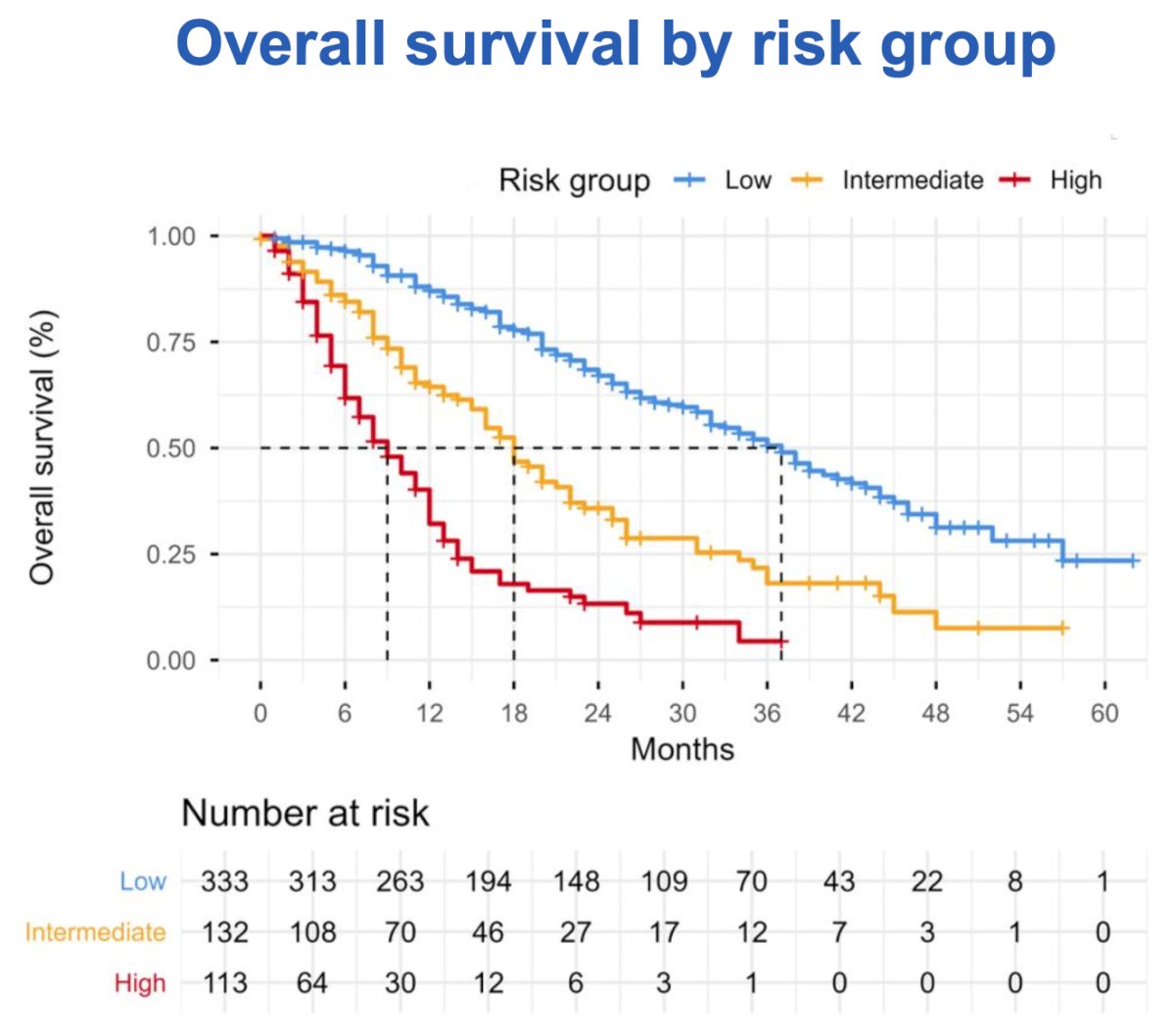
Furthermore, patients who failed to complete the planned six cycles of radium-223 experienced significantly worse overall survival compared with treatment completers (HR 2.5, 95% CI 1.9–3.3; p<0.0001), reinforcing the clinical importance of identifying patients at risk for early discontinuation prior to treatment initiation.
Dr. Yaegashi concluded with the following key messages:
- A simple 5-biomarker risk score using routinely available laboratory parameters was able to predict completion of radium-223 therapy prior to treatment initiation
- The model effectively stratified patients according to both the likelihood of treatment completion and overall survival outcomes
- The score identified patients at particularly high risk for early treatment discontinuation, which may help optimize patient selection in clinical practice
- A freely accessible web-based calculator was developed to facilitate bedside risk estimation and support shared decision-making between clinicians and patients
- The tool may be particularly useful for pretreatment counseling and setting realistic expectations regarding treatment tolerability and anticipated outcomes
Presented by: Hiroshi Yaegashi, MD, Assistant Professor in the Department of Integrative Cancer Therapy and Urology at Kanazawa University Graduate School of Medical Science, Kanazawa, Japan.
Written by: Julian Chavarriaga, MD, Clinical Assistant Professor, Urologic Oncologist, Department of Urology at Penn State Health @chavarriagaj on Twitter during the American Urological Association (AUA) 2026 Annual Meeting, Washington, DC, Fri, May 15 – Mon, May 18, 2026.