(UroToday.com) The American Urological Association's 2026 Annual Meeting, was host to the Interactive Poster IP38: Prostate Cancer: Advanced I Session. Dr. Anthony Zhang presented interactive poster IP38-02: Neoadjuvant apalutamide therapy enhances potency preservation following radical prostatectomy by downstaging the disease in men with high-risk prostate cancer: results of a randomized three-arm phase II trial
Dr. Zhang began by noting that functional recovery following radical prostatectomy remains challenging in patients with high-risk prostate cancer, particularly with respect to postoperative erectile function. He highlighted that neoadjuvant androgen receptor pathway inhibition may provide several potential advantages in this setting, including tumor downstaging, increased feasibility of nerve-sparing surgery, and ultimately improved postoperative potency outcomes.
Against this background, the investigators designed the study to evaluate whether neoadjuvant treatment with apalutamide plus abiraterone acetate/prednisone and a GnRH agonist could improve potency recovery at 12 months following surgery without compromising oncologic outcomes.
This was a randomized multicenter phase II trial (NCT02949284) evaluating neoadjuvant androgen receptor pathway inhibition prior to radical prostatectomy in patients with high-risk localized prostate cancer. Eligible patients had grade group ≥4 disease or a PSA >20 ng/mL. The primary endpoint of the study was potency recovery at 12 months following surgery.
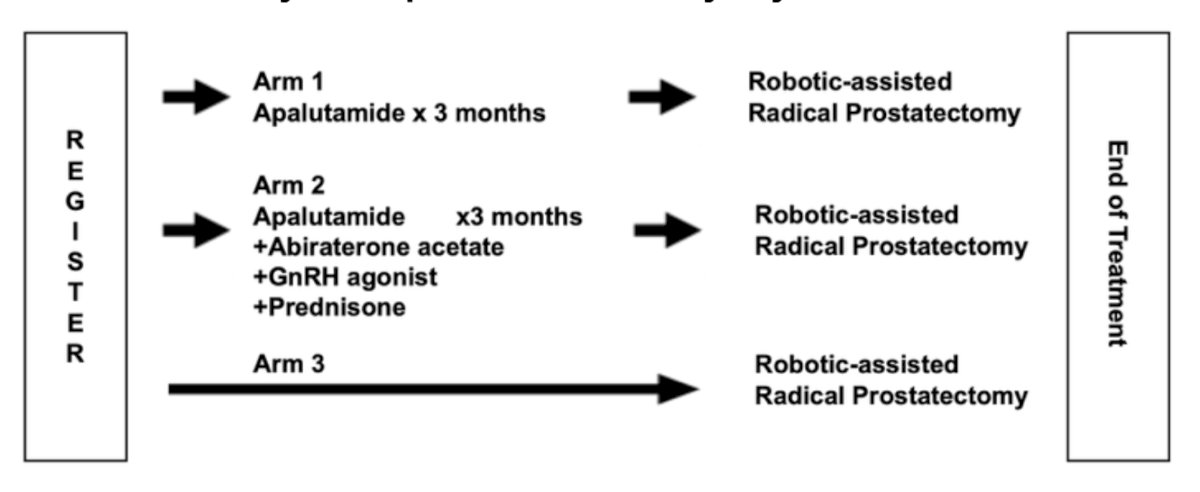
Patients were randomized into three treatment arms. Arm 1 received neoadjuvant apalutamide for 3 months prior to robotic-assisted radical prostatectomy. Arm 2 received intensified neoadjuvant therapy consisting of apalutamide combined with abiraterone acetate, prednisone, and a GnRH agonist for 3 months before surgery. Arm 3 proceeded directly to robotic-assisted radical prostatectomy without neoadjuvant systemic therapy. The study schema is shown below.
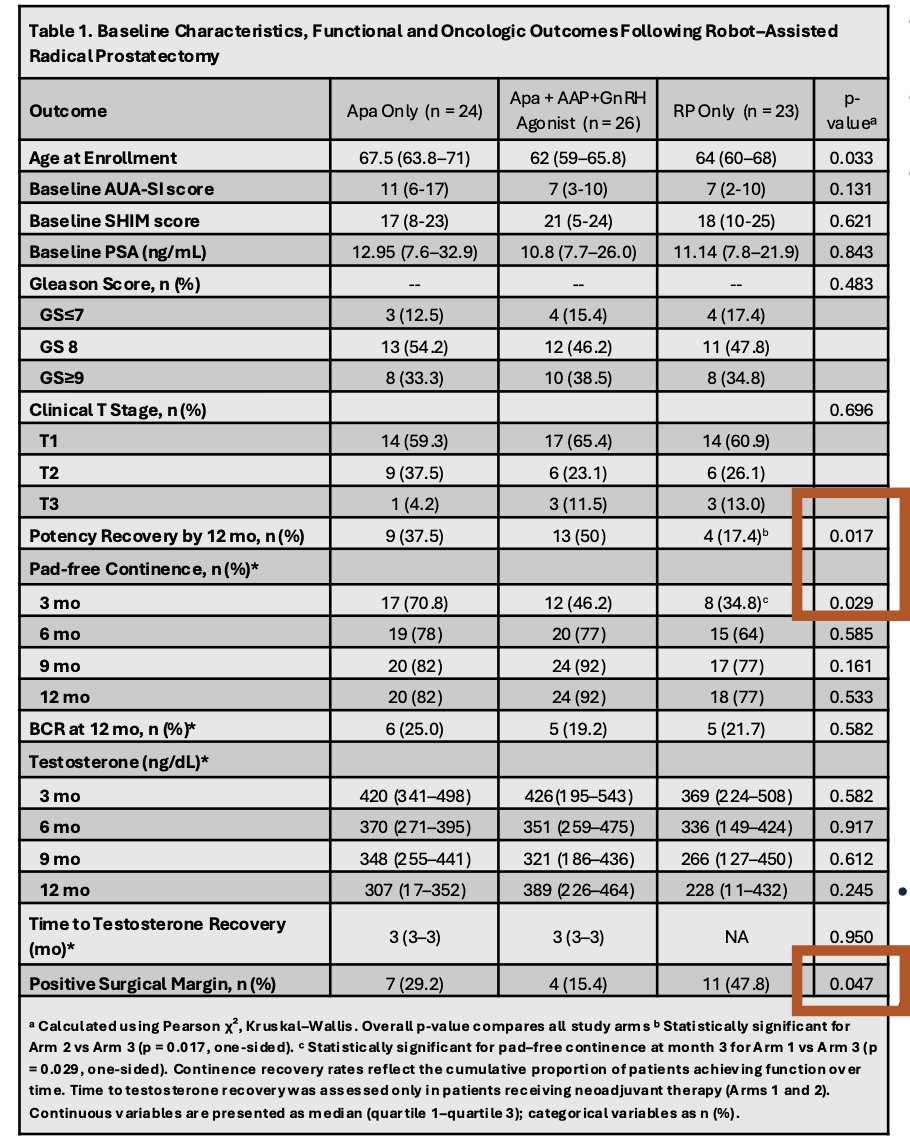
Baseline clinicopathologic characteristics were generally balanced across the three treatment groups, although patients in the intensified neoadjuvant arm tended to be younger at enrollment. Most patients had grade group 4–5 disease, with similar baseline PSA levels and clinical T stage distribution across cohorts. From a functional standpoint, potency recovery at 12 months was highest in the intensified neoadjuvant arm receiving apalutamide plus abiraterone/prednisone and GnRH agonist, reaching 50%, compared with 37.5% in the apalutamide-alone arm and 17.4% in the surgery-only arm (p=0.017). Early continence recovery at 3 months also favored neoadjuvant therapy, although continence rates became similar across groups over time.
Importantly, surgical margin rates were numerically lowest in the intensified neoadjuvant arm (15.4%) compared with apalutamide alone (29.2%) and surgery alone (47.8%), reaching statistical significance (p=0.047). Biochemical recurrence rates at 12 months were similar across groups, while testosterone recovery occurred rapidly following cessation of neoadjuvant therapy as shown in the table below.
The combination of apalutamide plus abiraterone/prednisone and GnRH agonist significantly improved potency recovery at 12 months compared with surgery alone. In addition, intensified neoadjuvant therapy was associated with lower positive surgical margin rates.
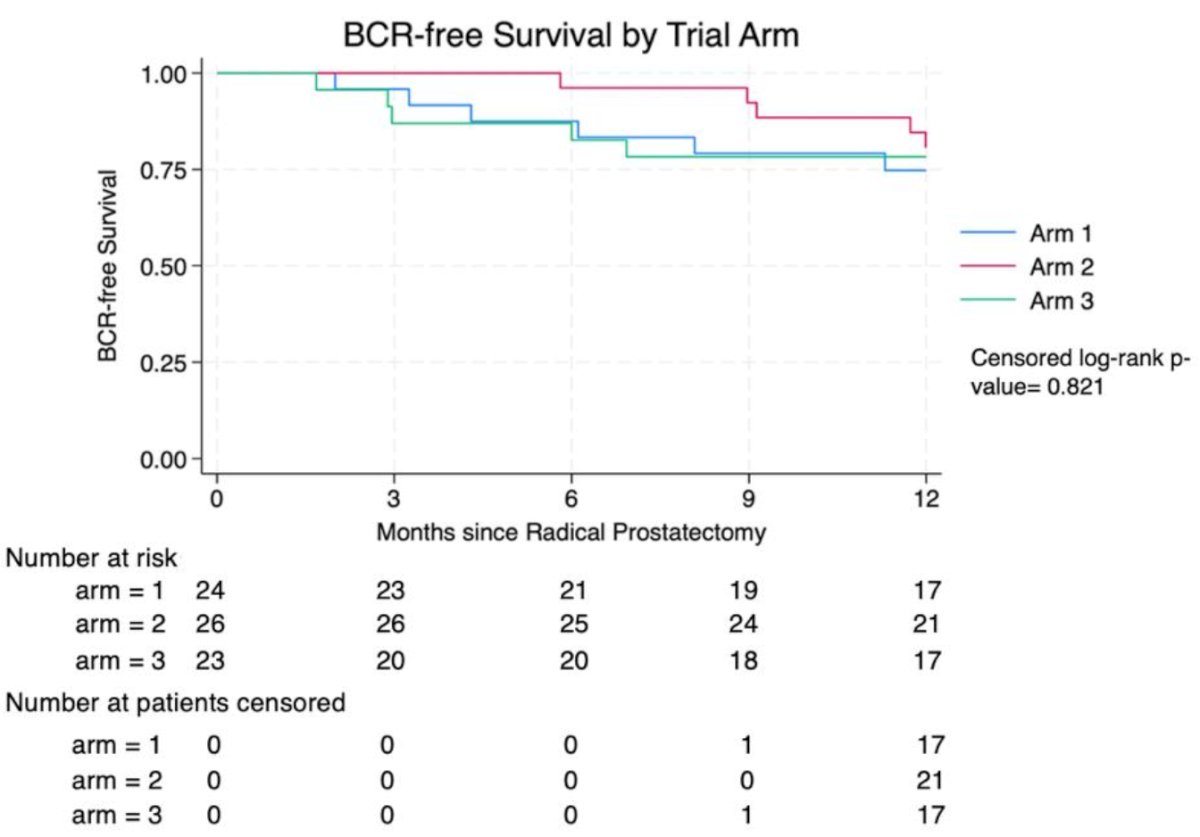
Interestingly, apalutamide monotherapy was associated with improved early continence recovery at 3 months following surgery. Despite differences in functional and pathologic outcomes, biochemical recurrence-free survival at 12 months was similar across treatment arms, although follow-up remains relatively short for definitive oncologic comparisons.
Dr. Zhang concluded with the following key points:
- Neoadjuvant apalutamide-based therapy prior to radical prostatectomy appeared safe and was associated with improved postoperative functional outcomes
- Early oncologic outcomes were similar across treatment groups
- The greatest benefit was observed with intensified combination therapy using apalutamide plus abiraterone/prednisone and GnRH agonist which provided improved potency recovery at 12 months and was associated with lower positive surgical margin rates compared with surgery alone
- These findings support further investigation of neoadjuvant ARPI-based strategies aimed at optimizing both oncologic and functional outcomes in high-risk localized prostate cancer
Presented by: Anthony Zhang, MD, Clinical Research Fellow, Yale School of Medicine, New Haven, CT
Written by: Julian Chavarriaga, MD, Clinical Assistant Professor, Urologic Oncologist, Department of Urology at Penn State Health @chavarriagaj on Twitter during the American Urological Association (AUA) 2026 Annual Meeting, Washington, DC, Fri, May 15 – Mon, May 18, 2026.
Related content: Neoadjuvant Apalutamide for Potency Preservation in High-Risk Prostate Cancer: A Randomized Trial - Isaac Kim