(UroToday.com) The American Urological Association's 2026 Annual Meeting, was host to the Interactive Poster IP38: Prostate Cancer: Advanced I Session. Dr. Soichiro Yoshida presented interactive poster IP38-13: Does Triplet Therapy Improve Survival in Metastatic Hormone-Sensitive Prostate Cancer? A Bayesian Individual Patient Data Reanalysis.
Dr. Yoshida began by noting that the incremental benefit of triplet therapy consisting of ADT, docetaxel, and an ARAT over contemporary doublet therapy with ADT plus an ARAT remains controversial in metastatic hormone-sensitive prostate cancer.1-3 Although prior reconstructed individual patient data analyses did not demonstrate a statistically significant overall survival advantage with triplet therapy, these analyses were unable to quantify the probability of clinical benefit.
To address this question, the investigators incorporated data from eight phase III trials evaluating treatment intensification strategies in mHSPC, including ARASENS,2 PEACE-1,3 ARANOTE, TITAN, ENZAMET, ARCHES, STAMPEDE, and LATITUDE.4 Using these datasets, the group performed a Bayesian reanalysis employing both Bayesian Cox proportional hazards modeling and hierarchical Poisson generalized linear mixed models. A noninformative prior distribution of Normal (0,10) was used for the primary analysis, while sensitivity analyses incorporated a weakly skeptical prior of Normal (0,05). Estimation was performed using Markov chain Monte Carlo methods.
The primary endpoint was overall survival, with the investigators specifically estimating the probability that triplet therapy conferred any benefit (Probability [HR<1.0]) as well as the probability of a clinically meaningful benefit (Probability [HR<0.8]). Additional subgroup analyses evaluated outcomes according to metastatic burden and compared AR inhibitor–based triplets with abiraterone-based triplet regimens. Secondary endpoints included radiographic progression-free survival and time to metastatic castration-resistant prostate cancer.
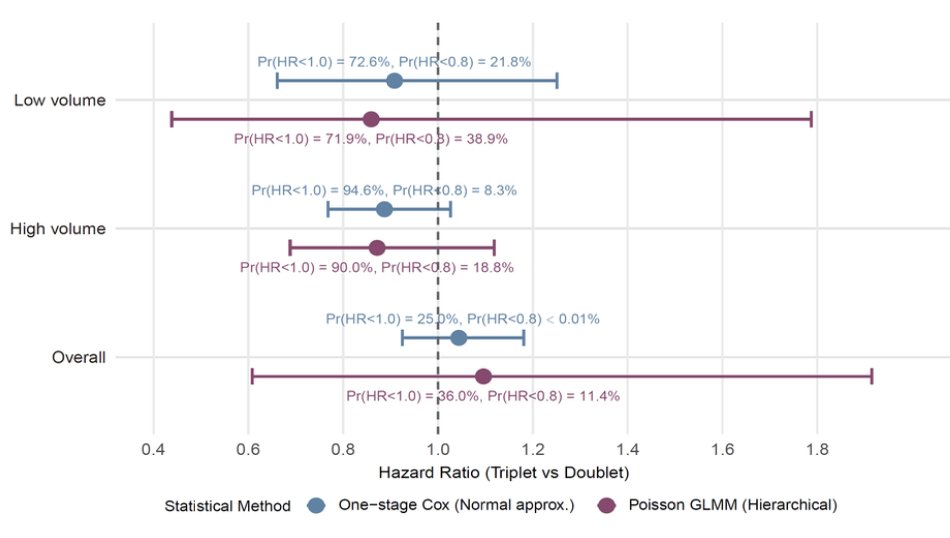
In the overall study population, triplet therapy was not associated with a clear overall survival advantage compared with doublet therapy, with a hazard ratio of 1.04 (95% Credible interval 0.92–1.18). Using the Bayesian framework, the probability that triplet therapy provided any survival benefit was only 36%, while the probability of a clinically meaningful benefit (HR <0.8) was 11%.
When stratified by disease volume, the probability of benefit appeared greater among patients with high-volume disease. In this subgroup, triplet therapy demonstrated a hazard ratio of 0.89 (95% Credible interval 0.77–1.03), corresponding to a 90% probability of any overall survival benefit, although the probability of a clinically meaningful benefit remained modest at 19%.
Among patients with low-volume disease, the estimated benefit of triplet therapy was less convincing, with a hazard ratio of 0.91 (95% Credible interval 0.66–1.25), a 73% probability of any benefit, and only a 22% probability of a clinically meaningful benefit. Importantly, the investigators emphasized that the overall probability of a meaningful survival advantage with triplet therapy remained low across the broader mHSPC population, although a modest signal of benefit may exist in selected patients with high-volume disease.
Dr. Yoshida concluded with the following key messages:
- ADT plus ARAT doublet therapy remains the preferred standard approach for most patients with mHSPC
- Triplet therapy may be selectively considered in patients with high-volume disease, where a modest probability of overall survival benefit was observed
- No clear overall survival advantage for triplet therapy was identified in the overall study population
- Although Bayesian analyses suggested a possible signal of benefit in high-volume disease, the probability of a clinically meaningful survival improvement remained relatively low
Presented by: Soichiro Yoshida, MD, Department of Urology, Tokyo Medical and Dental University, Tokyo, Japan.
Written by: Julian Chavarriaga, MD, Clinical Assistant Professor, Urologic Oncologist, Department of Urology at Penn State Health @chavarriagaj on Twitter during the American Urological Association (AUA) 2026 Annual Meeting, Washington, DC, Fri, May 15 – Mon, May 18, 2026.
References:
- Kyriakopoulos CE, Chen YH, Carducci MA, Liu G, Jarrard DF, Hahn NM, Shevrin DH, Dreicer R, Hussain M, Eisenberger M, Kohli M, Plimack ER, Vogelzang NJ, Picus J, Cooney MM, Garcia JA, DiPaola RS, Sweeney CJ. Chemohormonal Therapy in Metastatic Hormone-Sensitive Prostate Cancer: Long-Term Survival Analysis of the Randomized Phase III E3805 CHAARTED Trial. J Clin Oncol. 2018 Apr 10;36(11):1080-1087. doi: 10.1200/JCO.2017.75.3657. Epub 2018 Jan 31. PMID: 29384722; PMCID: PMC5891129.
- Smith MR, Hussain M, Saad F, Fizazi K, Sternberg CN, Crawford ED, Kopyltsov E, Park CH, Alekseev B, Montesa-Pino Á, Ye D, Parnis F, Cruz F, Tammela TLJ, Suzuki H, Utriainen T, Fu C, Uemura M, Méndez-Vidal MJ, Maughan BL, Joensuu H, Thiele S, Li R, Kuss I, Tombal B; ARASENS Trial Investigators. Darolutamide and Survival in Metastatic, Hormone-Sensitive Prostate Cancer. N Engl J Med. 2022 Mar 24;386(12):1132-1142. doi: 10.1056/NEJMoa2119115. Epub 2022 Feb 17. PMID: 35179323; PMCID: PMC9844551.
- Fizazi K, Foulon S, Carles J, Roubaud G, McDermott R, Fléchon A, Tombal B, Supiot S, Berthold D, Ronchin P, Kacso G, Gravis G, Calabro F, Berdah JF, Hasbini A, Silva M, Thiery-Vuillemin A, Latorzeff I, Mourey L, Laguerre B, Abadie-Lacourtoisie S, Martin E, El Kouri C, Escande A, Rosello A, Magne N, Schlurmann F, Priou F, Chand-Fouche ME, Freixa SV, Jamaluddin M, Rieger I, Bossi A; PEACE-1 investigators. Abiraterone plus prednisone added to androgen deprivation therapy and docetaxel in de novo metastatic castration-sensitive prostate cancer (PEACE-1): a multicentre, open-label, randomised, phase 3 study with a 2 × 2 factorial design. Lancet. 2022 Apr 30;399(10336):1695-1707. doi: 10.1016/S0140-6736(22)00367-1. Epub 2022 Apr 8. PMID: 35405085.
- Fizazi K, Tran N, Fein L, Matsubara N, Rodriguez-Antolin A, Alekseev BY, Özgüroğlu M, Ye D, Feyerabend S, Protheroe A, Sulur G, Luna Y, Li S, Mundle S, Chi KN. Abiraterone acetate plus prednisone in patients with newly diagnosed high-risk metastatic castration-sensitive prostate cancer (LATITUDE): final overall survival analysis of a randomised, double-blind, phase 3 trial. Lancet Oncol. 2019 May;20(5):686-700. doi: 10.1016/S1470-2045(19)30082-8. Epub 2019 Apr 12. PMID: 30987939.