(UroToday.com) The American Urological Association 2026 annual meeting featured a practice-changing, paradigm-shifting clinical trial in urology and a presentation by Dr. Jean Felipe Lestingi discussing long-term oncological outcomes of extended versus limited pelvic lymphadenectomy during radical prostatectomy for intermediate- and high-risk prostate cancer. The role of pelvic lymph node dissection in treating prostate cancer patients remains controversial, due to the lack of randomized trials with more extended and longer follow-up. Dr. Lestingi and colleagues previously reported early oncological outcomes from a randomized trial comparing limited pelvic lymphadenectomy versus extended pelvic lymphadenectomy during radical prostatectomy,1 and at AUA 2026 they reported updated data. The primary endpoint was biochemical recurrence free survival, and the secondary endpoints were metastasis free survival and cancer specific survival.
Between May 2012 and December 2016, in a single institution, 300 patients with D'Amico intermediate or high risk prostate cancer (≥ cT2b and/or ≥ PSA 10 ng/mL and/or Gleason score ≥ 7), absence of bone metastasis, and no previous treatment were randomized to undergo extended pelvic lymphadenectomy (bilaterally chains: obturator, external iliac, internal iliac, common iliac, and pre-sacral) or limited pelvic lymphadenectomy (obturator chains) in proportion 1:1 (extended pelvic lymphadenectomy n = 150; limited pelvic lymphadenectomy n = 150) during radical prostatectomy:
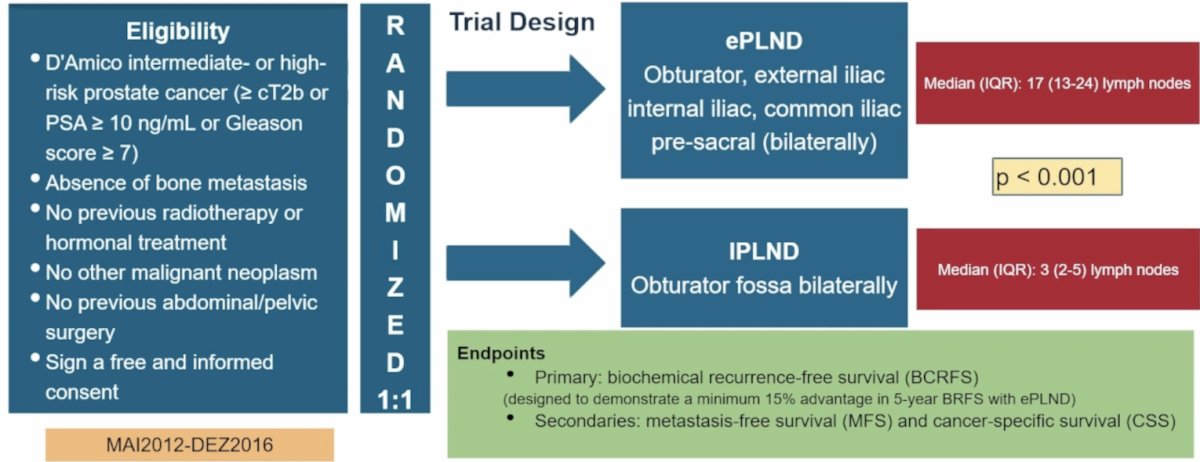
The trial was designed to demonstrate a minimum 15% advantage in 5-year biochemical recurrence free survival with extended pelvic lymphadenectomy.
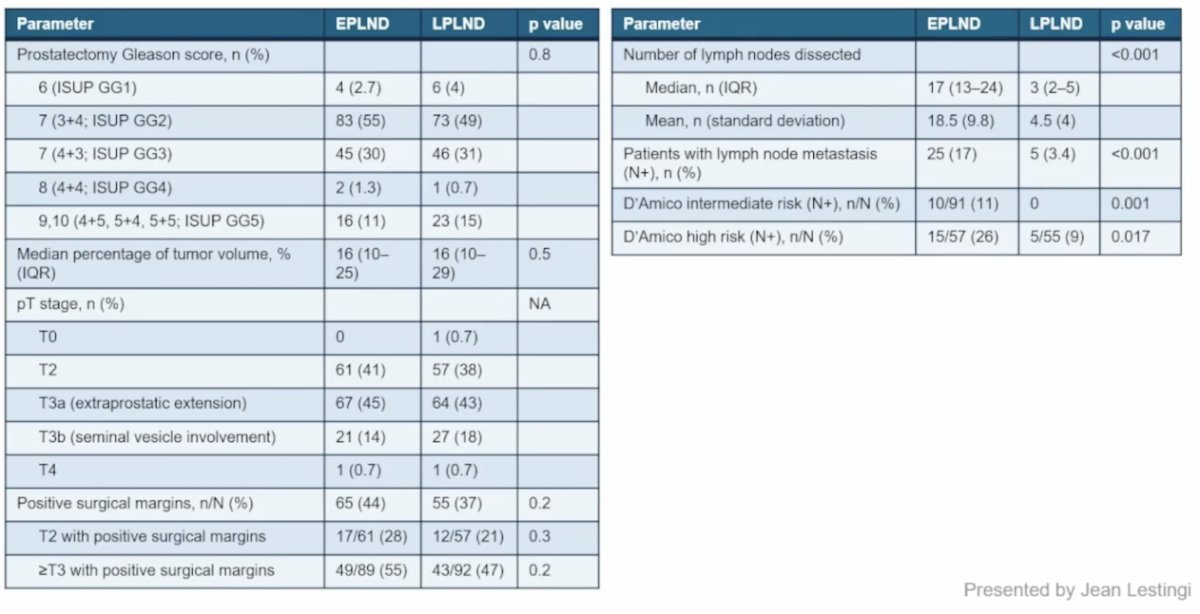
Baseline characteristics were well balanced between the two groups, including 62% of patients with intermediate risk disease undergoing extended pelvic lymphadenectomy versus 63% undergoing limited pelvic lymphadenectomy, and 38% of patients with high risk disease undergoing extended pelvic lymphadenectomy versus 37% undergoing limited pelvic lymphadenectomy. The pathological characteristics are as follows:
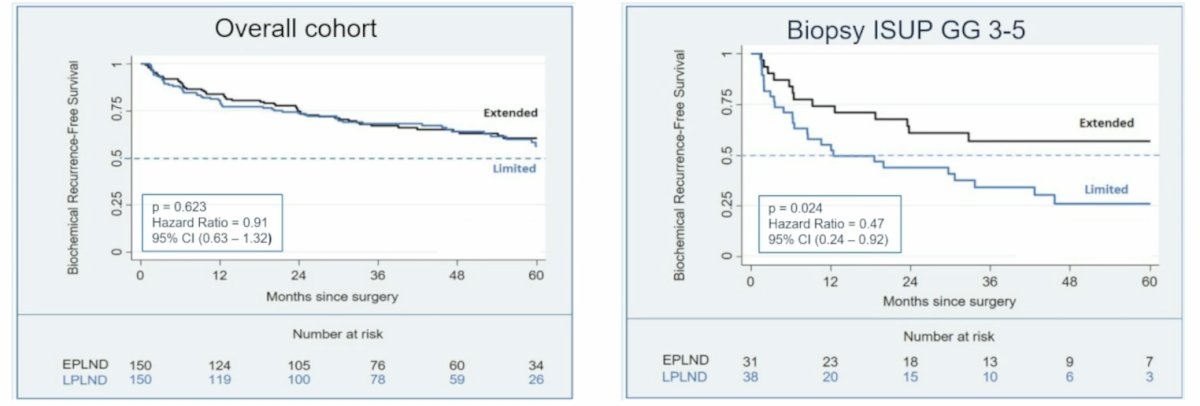
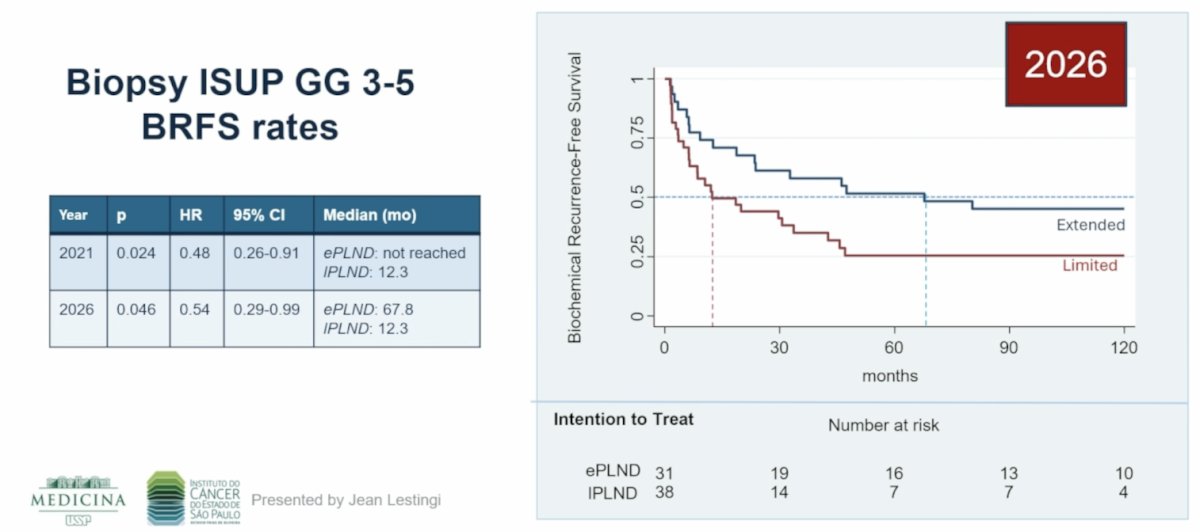
Previously reported,1 the biochemical recurrence free survival rate in the overall cohort showed no benefit for extended pelvic lymphadenectomy (HR 0.91, 95% CI 0.63-1.32), however there was a benefit for those with biopsy ISUP GG 3-5 (HR 0.47, 95% CI 0.24-0.92):
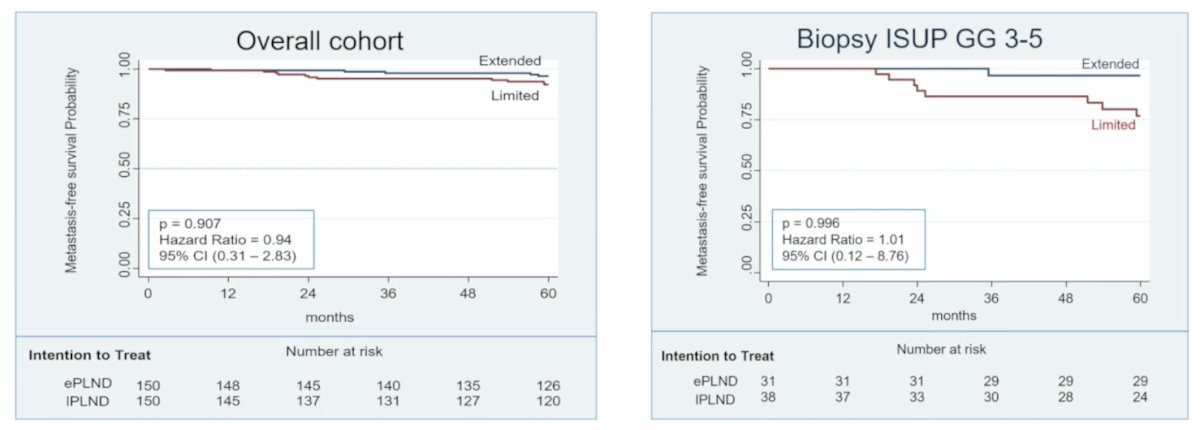
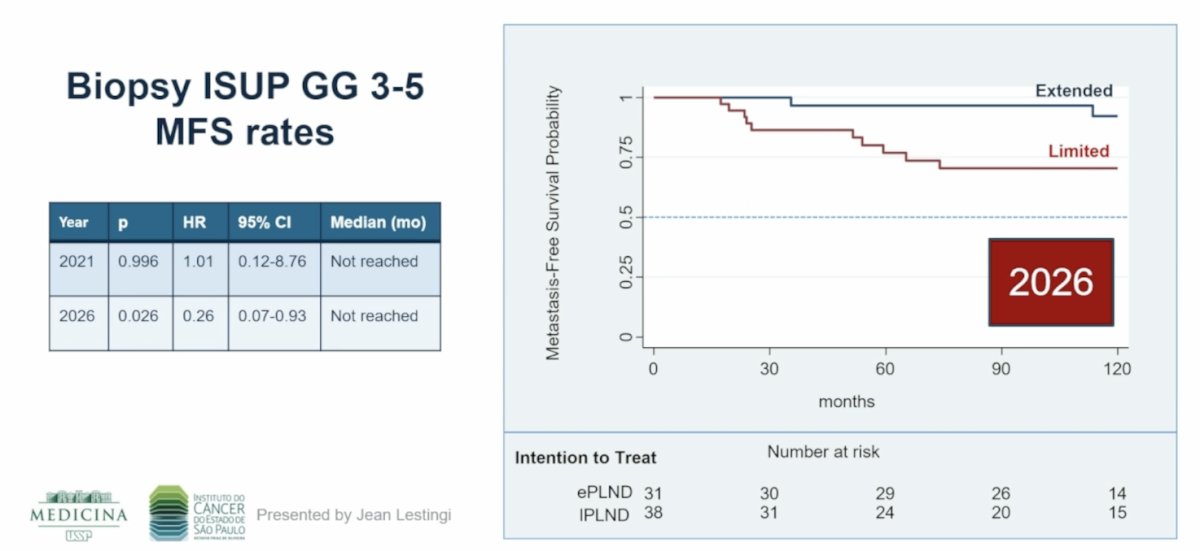
Also previously reported, there was no benefit for extended pelvic lymphadenectomy in the overall cohort for metastasis free survival (HR 0.94, 95% CI 0.31-2.83), and no benefit for those with biopsy ISUP GG 3-5 (HR 1.01, 95% CI 0.12-8.76):
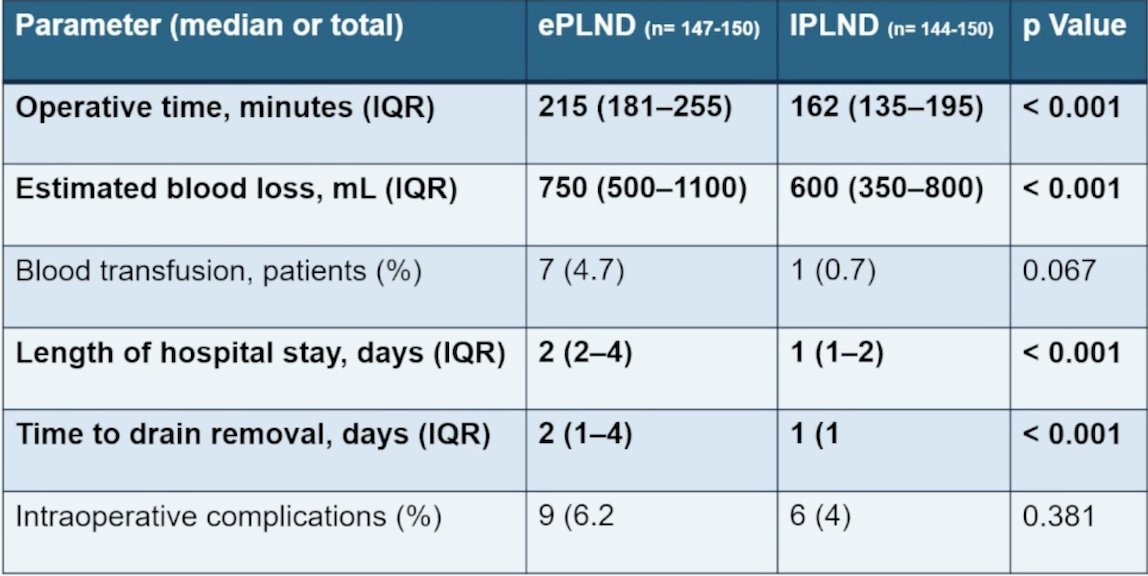
The previously reported surgical complication data showed a longer operative time for extended pelvic lymphadenectomy (p < 0.001), more blood loss (p < 0.001), longer hospital stay (p < 0.001), and longer time to drain removal (p < 0.001):
Based on these results reported in 2021, the AUA guidelines noted “Clinicians should inform patients that pelvic lymph node dissection staging information may guide future management, but does not consistently document improvement in metastasis free, cancer specific, or overall survival.”
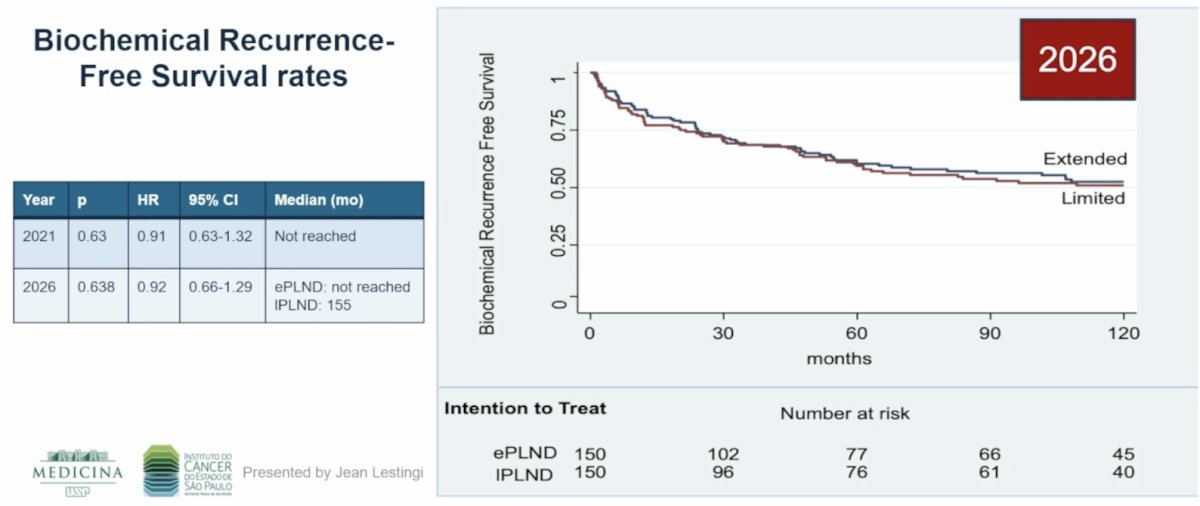
In this updated analysis presented at the AUA 2026 annual meeting, the mean and median follow-up were 119 (+/- 37.2) months and 130.6 (IQR 107.8-146.5) months, respectively. Considering the whole cohort, there were similar biochemical recurrence rates between the arms (HR 0.92, 95% CI 0.66-1.29; p = 0.638):
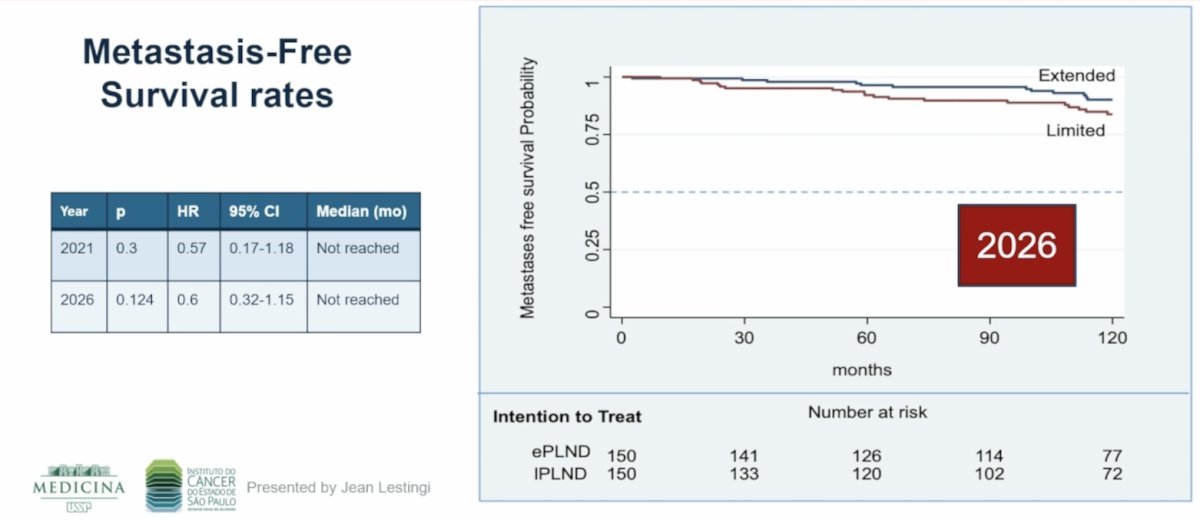
Additionally, there were no differences in metastasis free survival (HR 0.60, 95% CI 0.32-1.15; p = 0.124):
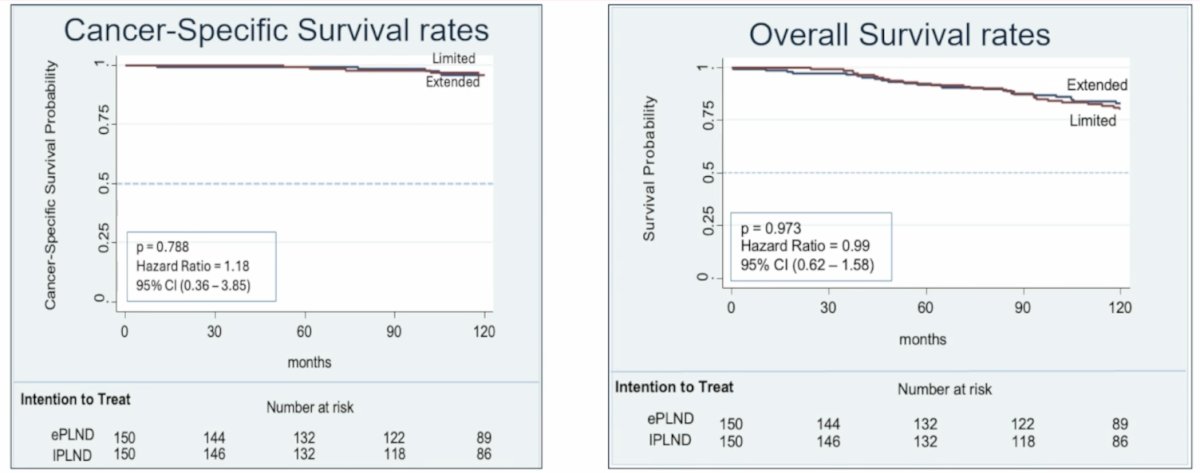
Moreover, there was no difference in cancer specific survival (HR 1.18, 95% CI 0.36-3.85) or overall survival (HR 0.99, 95% CI 0.62-1.58):
Nevertheless, patients with preoperative biopsy ISUP grade groups 3–5 who underwent extended pelvic lymphadenectomy had better biochemical recurrence free survival (HR 0.54, 95% CI 0.29-0.99; p =0.046):
Additionally, in this high-grade subgroup, a significant improvement in metastasis free survival was also observed with extended pelvic lymphadenectomy (HR 0.26, 95% CI 0.07–0.93; p = 0.026) with extended follow-up:
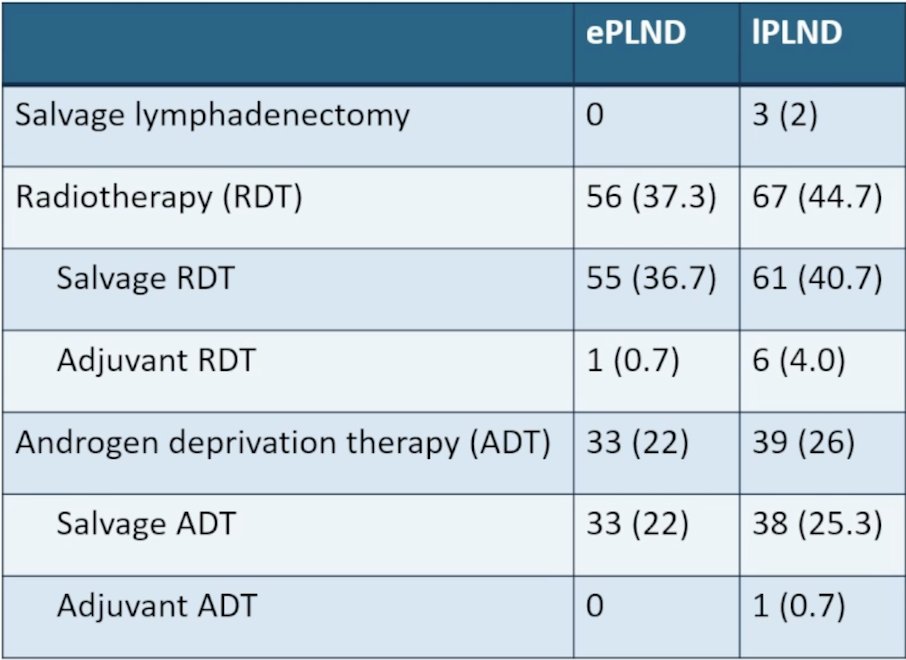
Secondary treatments stratified by extended versus limited pelvic lymphadenectomy are highlighted in the following table:
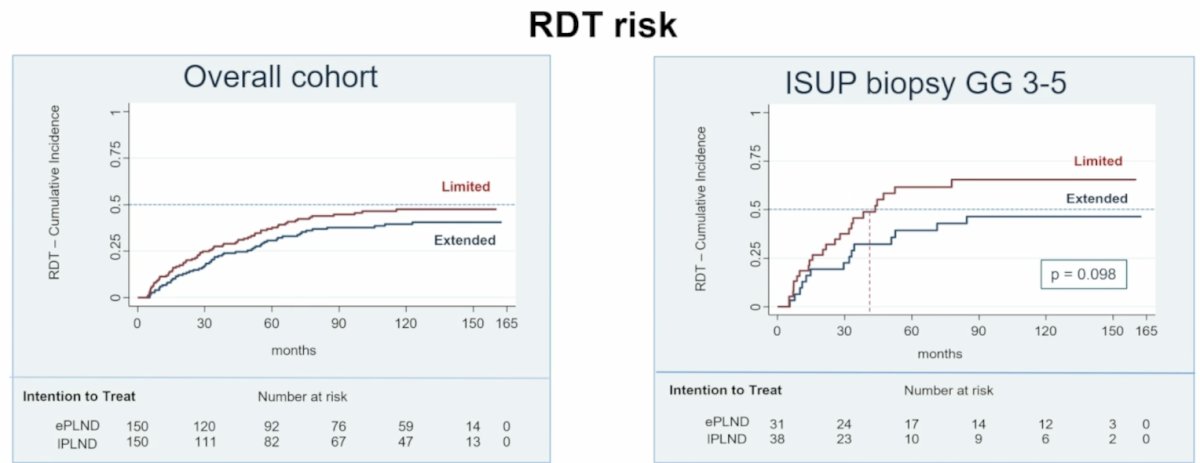
There was no difference in risk of radiotherapy amongst the overall cohort, although there was a trend towards patients undergoing limited pelvic lymphadenectomy having increased risk of radiotherapy (median time to radiotherapy: 43.7 months limited PLDN versus not reached for extended pelvic lymphadenectomy, p = 0.098):
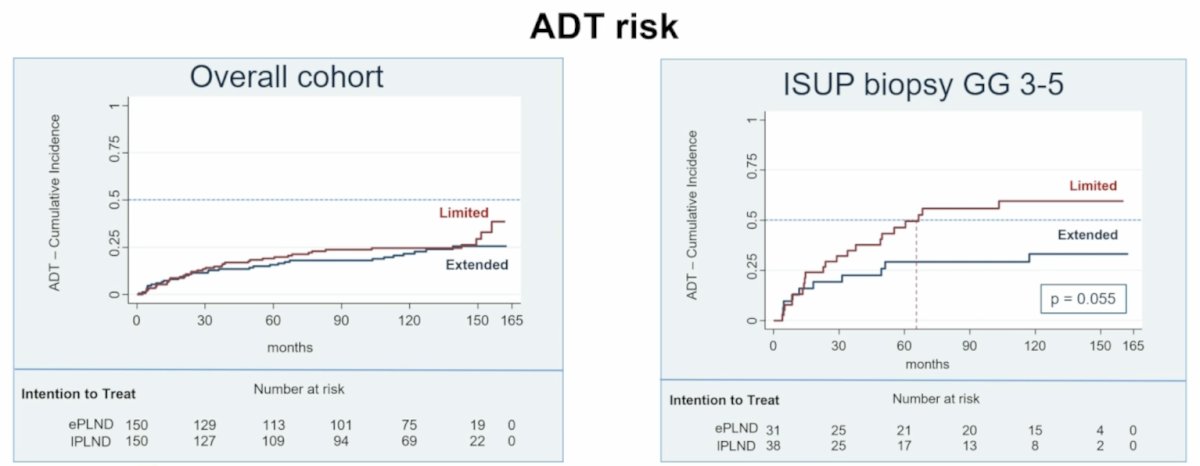
Additionally, there was no difference in risk of ADT amongst the overall cohort, although there was a trend towards patients undergoing limited pelvic lymphadenectomy having increased risk of ADT (median time to ADT: 66.5 months for limited PLDN versus not reached for extended pelvic lymphadenectomy, p = 0.055):
Dr. Lestingi concluded this presentation discussing long-term oncological outcomes of extended versus limited pelvic lymphadenectomy during radical prostatectomy for intermediate- and high-risk prostate cancer with the following take home points:
- As previously published, this randomized phase 3 trial did not demonstrate oncologic superiority of extended pelvic lymphadenectomy over limited pelvic lymphadenectomy among unselected intermediate and high-risk prostate cancer patients
- In patients with biopsy ISUP group grade 3–5 disease, after a long-term follow-up:
- Extended pelvic lymphadenectomy could be considered a standard in these subgroups undergoing radical prostatectomy
- Guidelines recommendations should consider this updated data
Presented by: Jean Felipe Lestingi, MD, Instituto do Cancer do Estado de Sao Paulo ICESP, Hospital das Clinicas HCFMUSP, Sao Paulo, Brazil
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the American Urological Association (AUA) 2026 Annual Meeting, Washington, DC, Fri, May 15 – Mon, May 18, 2026.
References: