(UroToday.com) The 2026 American Urological Association (AUA) Annual Meeting featured a poster presentation describing the development and validation of a simple, integer-based prognostic score designed to better quantify recurrence risk among patients with high-risk renal cell carcinoma (RCC) who meet eligibility criteria for adjuvant pembrolizumab based on the phase III KEYNOTE-564 trial.1
Adjuvant pembrolizumab is currently an approved standard of care for patients with resected high-risk clear cell RCC following nephrectomy, having demonstrated significant improvements in disease-free survival in KEYNOTE-564. However, the trial’s eligibility criteria encompassed a broad and clinically heterogeneous population, ranging from patients with pT2 grade 4 tumors to those with pT4, node-positive, or M1 no evidence of disease (M1 NED) status. As a result, clinicians and patients often face uncertainty regarding the absolute risk of recurrence and the magnitude of benefit expected from adjuvant systemic therapy.
To address this challenge, the study investigators performed a retrospective analysis of a large institutional registry and identified patients who fulfilled KEYNOTE-564 eligibility criteria. Using backward stepwise Cox proportional hazards regression with Akaike Information Criterion (AIC)-based model selection, they developed a prognostic model predicting recurrence and/or death at 48 months. Model discrimination was assessed using bootstrap-corrected concordance index (C-index), regression tree analysis was used to identify clinically informative cut-points, Kaplan–Meier analyses evaluated risk group separation, and decision curve analysis (DCA) was used to determine clinical utility.
The baseline study cohort characteristics, compared to those from the placebo arm of KEYNOTE-564, are summarized below: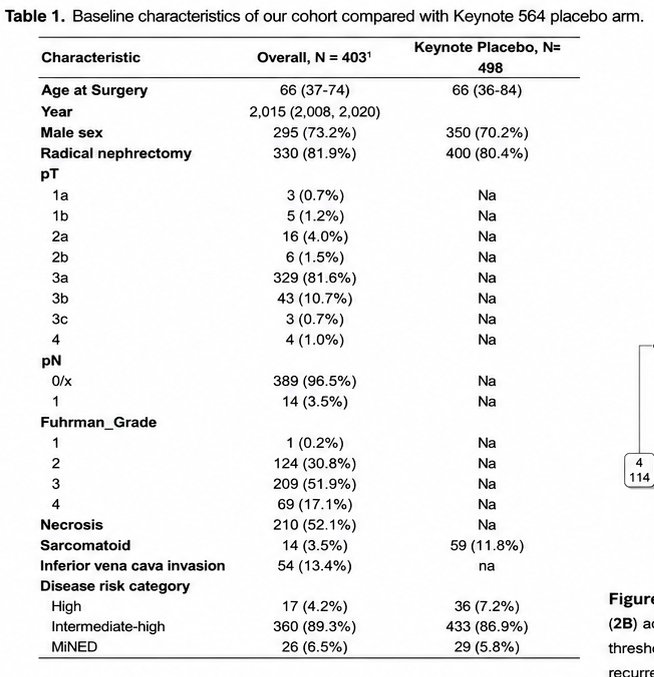
The final model demonstrated moderate discrimination, with a bootstrap-corrected C-index of 67.6%, indicating meaningful ability to distinguish between patients at lower and higher risk of recurrence or death.
From this multivariable model, the investigators derived a practical integer-based score composed of six routinely available pathologic and clinical features:
- Tumor necrosis: 1 point
- M1 no evidence of disease (M1 NED): 2 points
- Inferior vena cava (IVC) tumor thrombus: 2 points
- WHO/ISUP grade 3: 2 points
- WHO/ISUP grade 4 and/or sarcomatoid differentiation: 3 points
- pT4 and/or pN+ disease: 3 points
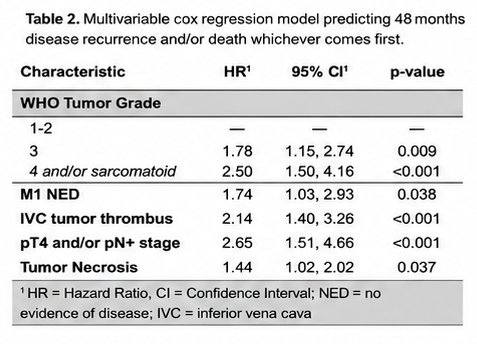
The accompanying model table highlighted the relative contribution of each variable, emphasizing that advanced stage (pT4/pN+), high-grade and sarcomatoid features, and metastatic disease rendered surgically disease-free (M1 NED) were among the strongest predictors of recurrence.
Using regression tree analysis, the investigators identified four prognostic subgroups with significantly different disease-free survival outcomes at 48 months (log-rank p<0.0001). The Kaplan–Meier curves showed clear and sustained separation between these groups, demonstrating the score’s ability to stratify patients into clinically meaningful risk categories.
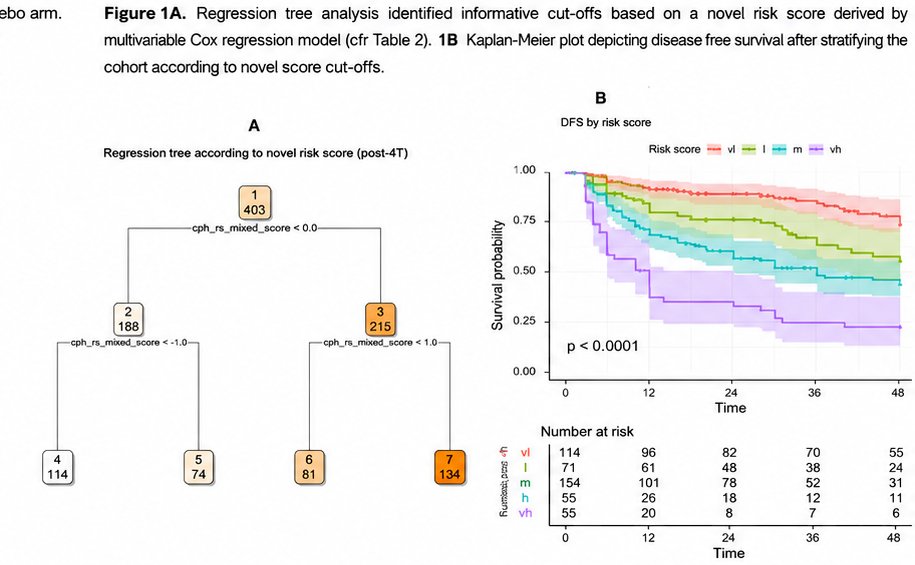
One of the most clinically relevant findings was that patients with a score <2 exhibited a negligible risk of recurrence and/or death over 48 months of follow-up. This suggests that such patients may derive limited absolute benefit from adjuvant pembrolizumab and could potentially be managed with surveillance alone after an informed discussion regarding risks and benefits.
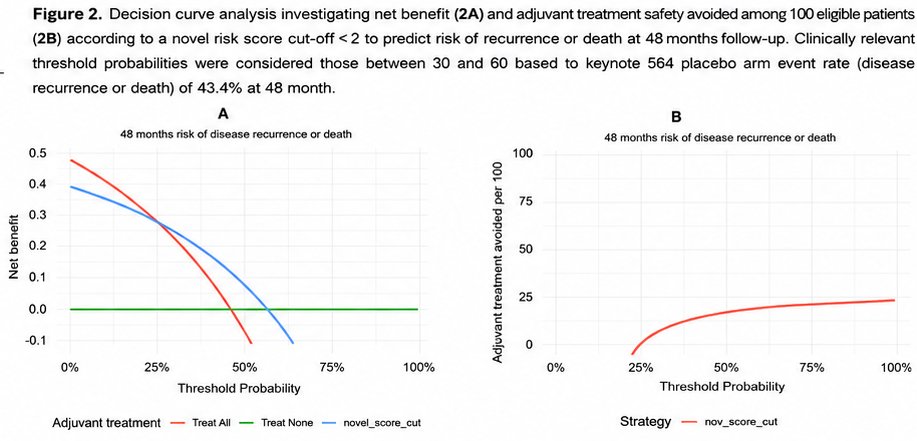
The decision curve analysis further reinforced the clinical value of the model. When a score threshold of ≥2 was used to recommend adjuvant therapy, the prognostic score provided greater net benefit than either a “treat all” or “treat none” strategy across a broad range of threshold probabilities between 25% and 50%. This is particularly important because these thresholds correspond closely to the recurrence risk levels at which clinicians and patients are most likely to consider adjuvant systemic therapy worthwhile.
The investigators concluded that this novel integer-based scoring system is a simple, practical, and validated tool for disease-free survival prognostication among KEYNOTE-564 eligible patients. By quantifying the heterogeneity within this broad “high-risk” population, the score offers a clinically useful framework to support shared decision-making and improve the selection of patients most likely to benefit from adjuvant pembrolizumab.
As adjuvant immunotherapy becomes increasingly integrated into RCC management, tools such as this are likely to play an important role in personalizing postoperative treatment recommendations and avoiding overtreatment in patients with very low residual recurrence risk.
Presented by: Rocco Simone Flammia, MD, Sapienza University of Rome, Rome, Italy
Written by: Rashid K. Sayyid, MD, MSc, Assistant Professor, Urologic Oncologist, Department of Urology at The University of Arizona and Banner University Medical Center, Tucson, AZ – @rksayyid on X during the American Urological Association (AUA) 2026 Annual Meeting, Washington, DC, Fri, May 15 – Mon, May 18, 2026.
References: