(UroToday.com) The American Urological Association's 2026 Annual Meeting, in Washington D.C., was host to the AUA-IBCG Bladder Cancer Forum. Drs. Shilpa Gupta, Felix Guerrero-Ramos and Andrea Necchi Debated Systemic Therapy in MIBC: Should we Follow the Protocol or Use Risk Adapted Therapy?
Dr. Gupta began by presenting the clinical case of a 64-year-old man with gross hematuria, ECOG 0 performance status, well-controlled hypertension, and a prior smoking history. MRI demonstrated a bladder mass staged as cT3bN0, while chest CT was negative for metastatic disease. TURBT confirmed high-grade urothelial carcinoma, with a creatinine clearance of 50 mL/min and positive ctDNA testing.
The patient subsequently received three cycles of EVP. After treatment, the patient developed mild neuropathy and subsequently underwent radical cystectomy with pelvic lymph node dissection (PLND). Final pathology demonstrated a pT0 or complete pathological response (pCR). At the 6-week postoperative visit, the patient was recovering well from surgery but continued to experience residual neuropathy, with repeat ctDNA testing now negative.
Dr. Gupta then posed the central management question to the audience: should treatment continue according to the original protocol-based approach, or should therapy now be adapted based on the patient’s favorable pathologic response and ctDNA status?
Sandwich therapy is the standard of careDr. Necchi began by outlining several key principles guiding the modern management of patients with MIBC. He noted that approximately 25% of MIBC cases present de novo, while an additional ~20% evolve from previously diagnosed NMIBC, raising important considerations regarding prior exposure to immunotherapy or antibody-drug conjugates and the potential impact on subsequent treatment strategies.1
He also discussed the evolving paradigm of cisplatin eligibility, emphasizing that nearly half of patients with MIBC historically never initiated neoadjuvant chemotherapy. According to Dr. Necchi, the increasing availability of IO- and ADC-based approaches is expanding eligibility for neoadjuvant treatment while also contributing to a growing number of patients declining conventional chemotherapy in favor of alternative strategies. Notably, there is an ongoing shift away from a purely neoadjuvant or adjuvant framework toward a more integrated “sandwich” treatment approach, with important future implications for surgical management and multidisciplinary care pathways.
The typical structure of contemporary phase 3 perioperative MIBC trials encompasses that many are built around a “sandwich” treatment approach incorporating both neoadjuvant and adjuvant therapy around radical cystectomy and PLND. For cisplatin-eligible patients, current trial designs commonly randomize patients to receive either IO plus chemotherapy or IO combined with a novel agent in the neoadjuvant setting, followed by continuation of IO-based therapy after surgery, compared with placebo plus chemotherapy followed by observation or placebo.
In cisplatin-ineligible populations, trials increasingly evaluate IO alone or IO combined with novel agents before cystectomy, with continuation of systemic therapy postoperatively versus observation alone as shown below.

Dr. Necchi also highlighted what he described as a missed opportunity within the design of many contemporary perioperative MIBC trials. While these studies helped establish the current standard-of-care perioperative strategies, most did not incorporate biomarker-driven treatment adaptation. He emphasized that biomarkers such as ctDNA could potentially have been used to individualize therapy duration, including identifying patients in whom treatment could be safely de-escalated or discontinued after surgery, rather than continuing protocol-mandated therapy uniformly across all patients.

Dr. Necchi subsequently reviewed long-term survival outcomes across multiple perioperative MIBC trials, including NIAGARA, EV-303/KEYNOTE-905, and SWOG-8710, emphasizing that achievement of pCR consistently correlates with improved overall survival regardless of how it is achieved.2-4 He noted that pCR remains one of the most robust prognostic markers and an established surrogate endpoint in MIBC.
Importantly, he highlighted that survival improvements with perioperative immunotherapy were also observed among patients who did not achieve pCR, raising ongoing questions regarding the relative contribution of adjuvant immunotherapy within modern “sandwich” treatment strategies. However, he emphasized that there are currently no validated predictive biomarkers capable of identifying which patients truly derive benefit from continued perioperative IO exposure. According to Dr. Necchi, current trial designs also limit the ability to extrapolate more refined biomarker-driven treatment decisions beyond what is inherently built into the study protocols.
Dr. Necchi also highlighted emerging perioperative data from China evaluating disitamab vedotin in HER2-expressing MIBC. In the phase 2 RC48-C017 study, neoadjuvant disitamab vedotin was associated with a pCR rate of 63.6% among patients who subsequently underwent radical cystectomy, while 75.8% achieved downstaging to ≤ypT1N0.5 Median time from completion of neoadjuvant therapy to surgery was 5 weeks, and early oncologic outcomes appeared encouraging, with 12-month EFS reaching 92.5%. He additionally noted that responses appeared numerically higher among tumors with HER2 IHC 3+ expression.
Dr. Necchi additionally emphasized the substantial attrition observed across contemporary perioperative phase 3 MIBC trials. Across studies such as NIAGARA, KEYNOTE-905, and KEYNOTE-B15, only approximately 60–70% of randomized patients ultimately initiated adjuvant therapy, with even fewer completing the planned postoperative treatment course.2-4 He noted that these rates are likely even lower in real-world and community practice settings, where postoperative recovery, toxicity, comorbidities, and patient preference further limit treatment continuation.

Dr. Andrea Necchi concluded his presentation with the following key takeaways:
- Sandwich (perioperative) therapy remains the current standard of care for patients with MIBC, supported by level 1 evidence
- Current data do not yet support safe de-escalation of perioperative systemic therapy after initiation of EV-P or durvalumab plus GC
- Given that pCR is achieved in approximately 35–60% of patients receiving neoadjuvant therapy, a selected subset of patients may potentially forgo radical cystectomy and instead undergo stringent surveillance strategies
- Multiple ongoing efforts are evaluating whether the adjuvant or surgical component of therapy can be safely omitted in carefully selected patients using biomarker- and response-adapted approaches
Going back to the clinical case, Dr. Guerrero argued that three factors together were sufficient to support a risk-adapted treatment approach following perioperative EV-P: initial cT3 disease treated with neoadjuvant EV-P, achievement of ypT0 at cystectomy, and postoperative ctDNA negativity. He further noted that persistent neuropathy added another important clinical consideration favoring individualized treatment decision-making rather than automatic continuation of protocol-driven therapy.
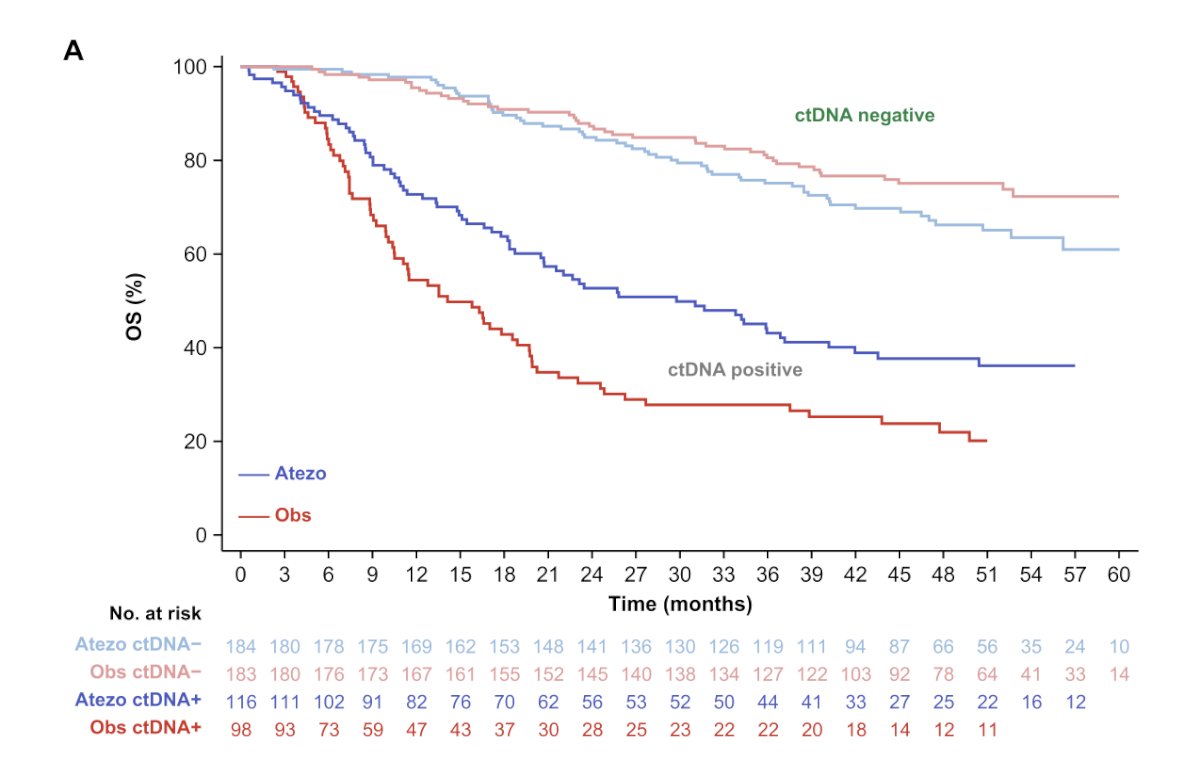
Dr. Guerrero highlighted that the idea to avoid adjuvant therapy began with the ctDNA subgroup analysis from IMvigor010, specifically emphasizing the forest plot demonstrating differential benefit according to ctDNA status. In the study, ctDNA-positive patients appeared to derive significant benefit from adjuvant atezolizumab compared with observation (HR 0.59, 95% CI 0.42–0.83), whereas ctDNA-negative patients did not appear to benefit from adjuvant therapy (HR 1.38, 95% CI 0.93–2.05). He noted that these findings helped establish the foundation for biomarker-driven perioperative strategies in MIBC and raised the possibility that selected ctDNA-negative patients may safely avoid adjuvant treatment.6
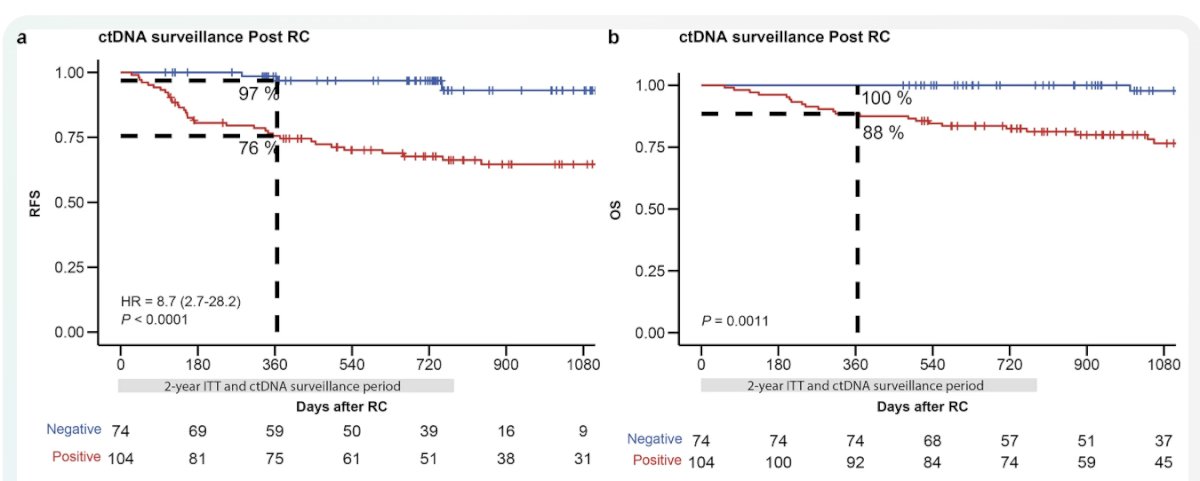
Furthermore, Dr. Guerrero highlighted the TOMBOLA trial, which evaluated a ctDNA-guided perioperative strategy in MIBC. He noted that the study moved beyond traditional clinicopathologic risk stratification by incorporating serial ctDNA testing following radical cystectomy to dynamically guide adjuvant immunotherapy decisions. Importantly, ctDNA-negative patients demonstrated excellent outcomes with surveillance alone, achieving a 97% 1-year recurrence-free survival rate, supporting the concept that selected biomarker-negative patients may safely avoid adjuvant therapy.
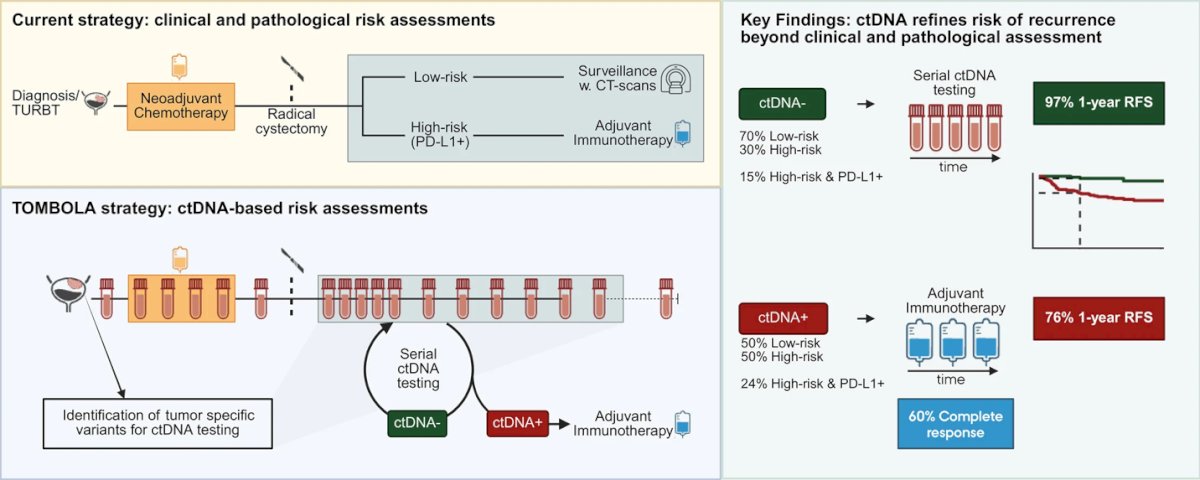
In contrast, ctDNA-positive patients were treated with adjuvant immunotherapy, achieving a 76% 1-year recurrence-free survival rate and complete responses in approximately 60% of cases
Dr. Guerrero subsequently highlighted IMvigor011, describing it as the first biomarker-guided surveillance strategy following radical cystectomy in MIBC. He noted that Atezolizumab recently received FDA approval for ctDNA positive patients, and Signatera was approved as a companion diagnostic test just three days prior to the presentation and represented a major step toward personalized MRD-guided management. Importantly, serial ctDNA testing demonstrated strong prognostic value beyond standard clinicopathologic risk factors. Patients who remained ctDNA-negative after surgery achieved excellent outcomes with surveillance alone, whereas early ctDNA positivity was associated with significantly inferior DFS and OS.
Among ctDNA-positive patients, adjuvant atezolizumab significantly improved outcomes compared with placebo, including improvements in DFS (HR 0.64, 95% CI 0.47–0.87) and OS (HR 0.59, 95% CI 0.39–0.90). According to Dr. Guerrero, these findings reinforce a biomarker-driven perioperative approach in which ctDNA-negative patients may safely proceed with surveillance, potentially avoiding unnecessary adjuvant therapy.

Timing of ctDNA positivity carries important prognostic implications. In IMvigor011,7 patients who remained persistently ctDNA-negative demonstrated excellent DFS and OS outcomes, whereas patients with early ctDNA positivity following cystectomy experienced substantially inferior clinical outcomes. Dr. Guerrero noted that patients who became ctDNA-positive at the initial postoperative assessment had the worst prognosis, with markedly shorter DFS and OS compared with patients who developed ctDNA positivity later during surveillance. According to him, these findings suggest that serial ctDNA monitoring may provide dynamic risk stratification beyond a single binary ctDNA assessment.
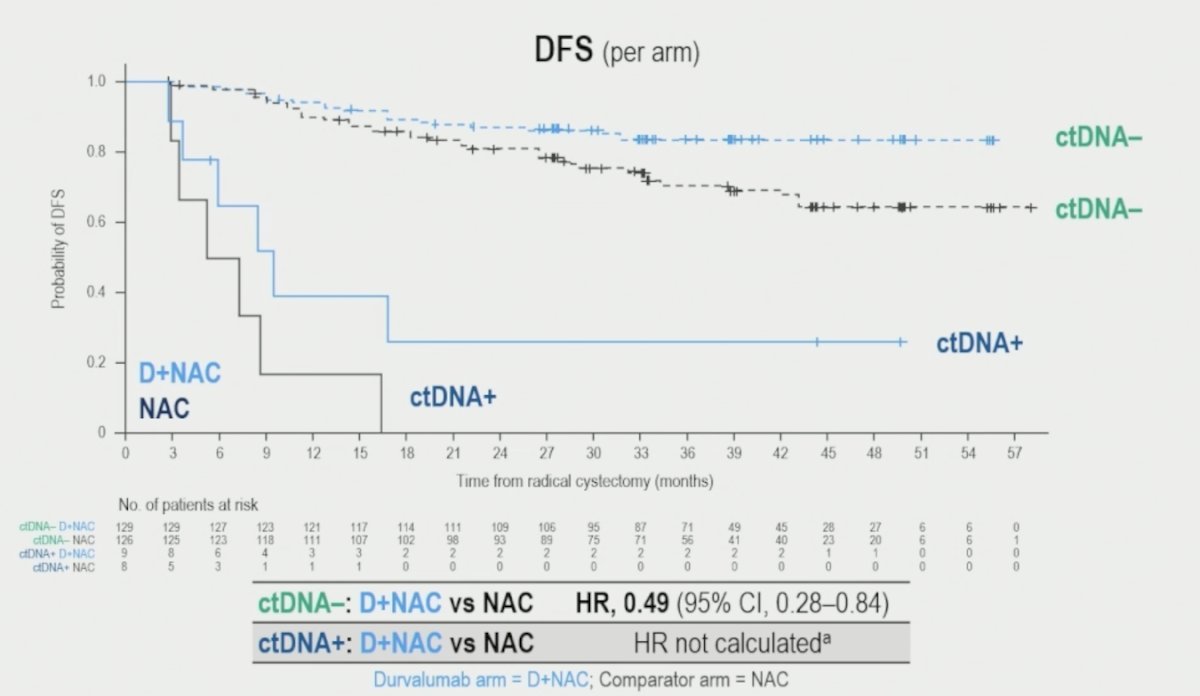
Dr. Guerrero also discussed exploratory ctDNA analyses from the NIAGARA trial, highlighting the ongoing uncertainty regarding the relative contribution of neoadjuvant versus adjuvant immunotherapy. Referring to the ctDNA-stratified DFS curves, he questioned how much of the observed benefit was attributable to neoadjuvant durvalumab compared with the adjuvant component of therapy.
Notably, among ctDNA-negative patients, the addition of durvalumab to neoadjuvant chemotherapy was associated with improved DFS compared with NAC alone (HR 0.49, 95% CI 0.28–0.84). However, outcomes among ctDNA-positive patients remained poor, and hazard ratios could not be reliably calculated because of the limited number of patients.
Dr. Guerrero also emphasized the importance of carefully considering treatment-related toxicity, particularly with EV-containing perioperative regimens. Reviewing the safety profile of adjuvant EV plus pembrolizumab, he noted that even low-grade toxicities, especially neuropathy, may significantly affect patients’ quality of life and daily functioning. He stressed that while many adverse events are classified as grade 1–2, chronic neuropathy, fatigue, pruritus, and gastrointestinal toxicities can still meaningfully impact long-term survivorship, further supporting efforts to identify patients who may safely undergo treatment de-escalation strategies.

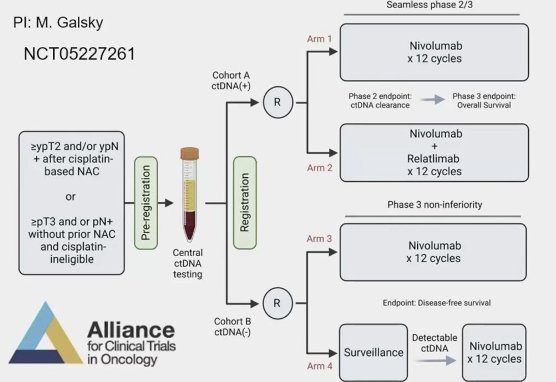
Dr. Guerrero wrapped up his presentation by highlighting ongoing biomarker-driven perioperative trials, including the Alliance AO2103 (MODERN) study, which he described as a major step toward personalized treatment intensification and de-escalation strategies in MIBC. The MODERN trial utilizes a ctDNA-guided design following radical cystectomy. Patients with detectable ctDNA are randomized to receive either nivolumab alone or nivolumab plus relatlimab, with ctDNA clearance serving as the phase 2 endpoint and overall survival as the phase 3 endpoint. In contrast, ctDNA-negative patients are randomized to either adjuvant nivolumab or surveillance, with the option to initiate nivolumab if ctDNA becomes detectable during follow-up.
During the discussion, Dr. Gupta asked whether management would differ if the patient had not developed neuropathy following EV-P. Dr. Guerrero responded that the regimen was designed and approved as a perioperative “sandwich” approach, and therefore treatment should generally be administered as studied, including the adjuvant component. He added that if patients ultimately decline radical cystectomy, clinicians should not “fight” the patient. However, he noted that if the surgical component is removed from the treatment paradigm, Dr. Necchi would favor continuation of systemic therapy to maintain disease control.
Audience polling reflected the ongoing uncertainty surrounding perioperative treatment de-escalation. Approximately 41% of participants favored completing the full sandwich approach, while another 41% supported omission of the adjuvant component in this clinical scenario.
Presented by:
- Shilpa Gupta, MD, Director, Genitourinary Medical Oncology, Taussig Cancer Institute, Co-Leader of the Genitourinary Oncology Program, Department of Hematology and Medical Oncology, Cleveland Clinic, Cleveland, OH
- Félix Guerrero-Ramos, MD, PhD, FEBU, Urologist, Oncologic Urology Unit Coordinator, Hospital Universitario 12 de Octubre, Madrid, Spain
- Andrea Necchi, MD, Chief of Genitourinary Medical Oncology, IRCCS San Raffaele Hospital and Scientific Institute, Professor of Oncology, Vita-Salute San Raffaele University, Milan, Italy
Written by: Julian Chavarriaga, MD, Clinical Assistant Professor, Urologic Oncologist, Department of Urology at Penn State Health @chavarriagaj on Twitter during the American Urological Association (AUA) 2026 Annual Meeting, Washington, DC, Fri, May 15 – Mon, May 18, 2026.
Reference:
- Roviello G, Santoni M, Sonpavde GP, Catalano M. The evolving treatment landscape of metastatic urothelial cancer. Nat Rev Urol. 2024 Oct;21(10):580-592. doi: 10.1038/s41585-024-00872-0. Epub 2024 May 3. PMID: 38702396.
- Powles T, Catto JWF, Galsky MD, Al-Ahmadie H, Meeks JJ, Nishiyama H, Vu TQ, Antonuzzo L, Wiechno P, Atduev V, Kann AG, Kim TH, Suárez C, Chang CH, Roghmann F, Özgüroğlu M, Eigl BJ, Oliveira N, Buchler T, Gadot M, Zakharia Y, Armstrong J, Gupta A, Hois S, van der Heijden MS; NIAGARA Investigators. Perioperative Durvalumab with Neoadjuvant Chemotherapy in Operable Bladder Cancer. N Engl J Med. 2024 Nov 14;391(19):1773-1786. doi: 10.1056/NEJMoa2408154. Epub 2024 Sep 15. PMID: 39282910.
- Vulsteke C, Adra N, Danchaivijitr P, Sabadash M, Rodriguez-Vida A, Zhang Z, Atduev V, Göger YE, Rausch S, Kang SH, Loriot Y, Bedke J, Galsky MD, O'Donnell PH, von Amsberg G, Alimohamed N, Sulimka G, Gupta S, Paramonov V, Nakane K, Mihm M, Meng C, Huang CD, Ramamurthy C, Homet Moreno B, Ullén A; KEYNOTE-905/EV-303 Investigators. Perioperative Enfortumab Vedotin and Pembrolizumab in Bladder Cancer. N Engl J Med. 2026 Apr 2;394(13):1257-1269. doi: 10.1056/NEJMoa2511674. Epub 2026 Feb 18. PMID: 41707170.
- Grossman HB, Natale RB, Tangen CM, Speights VO, Vogelzang NJ, Trump DL, deVere White RW, Sarosdy MF, Wood DP Jr, Raghavan D, Crawford ED. Neoadjuvant chemotherapy plus cystectomy compared with cystectomy alone for locally advanced bladder cancer. N Engl J Med. 2003 Aug 28;349(9):859-66. doi: 10.1056/NEJMoa022148. Erratum in: N Engl J Med. 2003 Nov 6;349(19):1880. PMID: 12944571.
- Guo X, Wang S, Ma Y, Du Y, Chen Y, Wang Q, Yang K, Tang Q, Fan Y, Hao H, He Z, Gong Y, Zhang C. Disitamab vedotin (RC48-ADC) combined with immunotherapy as neoadjuvant therapy for localized muscle-invasive bladder cancer: a multicenter real-world study. NPJ Precis Oncol. 2025 Dec 3;10(1):11. doi: 10.1038/s41698-025-01211-1. PMID: 41331072; PMCID: PMC12780152.
- Powles T, Assaf ZJ, Degaonkar V, Grivas P, Hussain M, Oudard S, Gschwend JE, Albers P, Castellano D, Nishiyama H, Daneshmand S, Sharma S, Sethi H, Aleshin A, Shi Y, Davarpanah N, Carter C, Bellmunt J, Mariathasan S. Updated Overall Survival by Circulating Tumor DNA Status from the Phase 3 IMvigor010 Trial: Adjuvant Atezolizumab Versus Observation in Muscle-invasive Urothelial Carcinoma. Eur Urol. 2024 Feb;85(2):114-122. doi: 10.1016/j.eururo.2023.06.007. Epub 2023 Jul 26. PMID: 37500339.
- Powles T, Kann AG, Castellano D, Gross-Goupil M, Nishiyama H, Bracarda S, Bjerggaard Jensen J, Makaroff L, Jiang S, Ku JH, Park SH, Reig Torras O, Ye D, Maruzzo M, Necchi A, Morales-Barrera R, Giunta EF, Lee JL, Tortora G, Ürün Y, Dolowy L, Erdem D, Pinto A, Grando F, Zou W, Assaf ZJ, Vuky J, Degaonkar V, Steinberg EE, Bellmunt J, Gschwend JE; IMvigor011 Investigators. ctDNA-Guided Adjuvant Atezolizumab in Muscle-Invasive Bladder Cancer. N Engl J Med. 2025 Dec 18;393(24):2395-2408. doi: 10.1056/NEJMoa2511885. Epub 2025 Oct 20. PMID: 41124204.