(UroToday.com) At the 2026 American Urological Association (AUA) Annual Meeting in Washington, DC, the AUA–International Bladder Cancer Group (IBCG) Bladder Cancer Forum hosted a timely debate in the contemporary management of non–muscle-invasive bladder cancer (NMIBC): whether systemic immuno-oncology (IO) should be added upfront to bacillus Calmette-Guérin (BCG) for patients with BCG-naïve high-risk disease. This discussion occurred in the aftermath of two positive randomized phase III trials—POTOMAC evaluating durvalumab plus BCG1 and CREST evaluating sasanlimab plus BCG2—both of which demonstrated statistically significant improvements in recurrence-related endpoints. At the same time, the phase III ALBAN trial evaluating atezolizumab plus BCG failed to show any efficacy advantage over BCG alone.3 These divergent results have catalyzed an important clinical question: do the gains observed in POTOMAC and CREST justify introducing systemic immunotherapy into a disease state that has historically been managed effectively with intravesical therapy alone?
Following a case presentation by Dr. Mark Tyson, Dr. Neal Shore argued that the addition of IO to BCG represents meaningful clinical progress and the first successful strategy to improve upon a four-decade standard of care. In contrast, Dr. Morgan Rouprêt contended that routine adoption of this strategy in 2026 constitutes clinical overreach, exposing patients with localized disease to substantial toxicity, cost, and logistical burden in exchange for only modest improvements in recurrence endpoints.
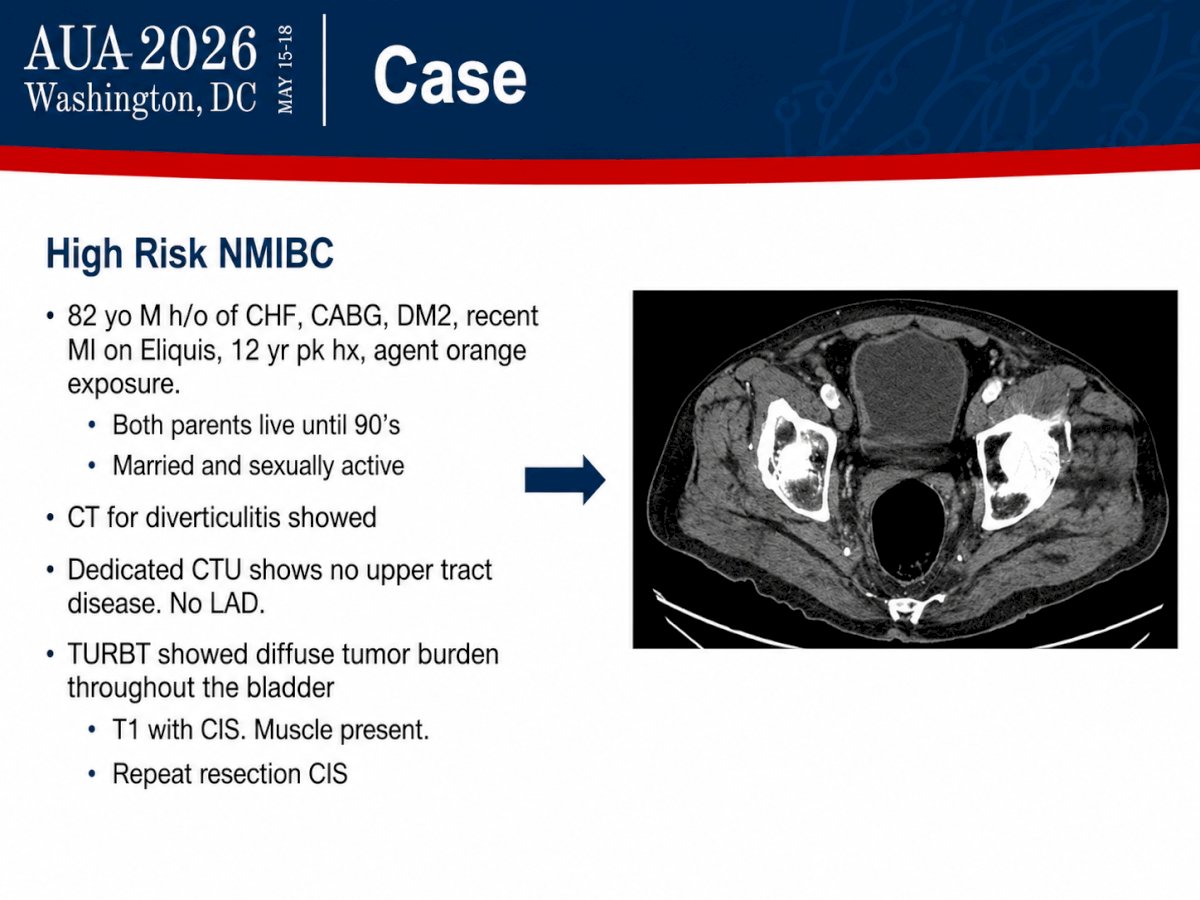
Dr. Mark Tyson opened the session by presenting a representative case of an 82-year-old man with very high-risk BCG-naïve NMIBC. The patient had significant cardiovascular comorbidities, including congestive heart failure, prior coronary artery bypass grafting, diabetes mellitus, and a recent myocardial infarction requiring anticoagulation with apixaban. Despite these medical issues, he remained sexually active and had a strong family history of longevity, suggesting substantial functional reserve and life expectancy. The bladder tumor was detected incidentally during imaging for diverticulitis. CT urography demonstrated no upper tract disease or lymphadenopathy. Transurethral resection of bladder tumor revealed diffuse tumor burden with T1 high-grade urothelial carcinoma and concomitant carcinoma in situ (CIS), with muscularis propria present in the specimen. Repeat resection confirmed persistent CIS. Dr. Tyson used this case to frame the central clinical dilemma: in an older but physiologically robust patient with diffuse T1 high-grade disease and persistent CIS, is optimized induction and maintenance BCG sufficient, or should frontline treatment be intensified with systemic immunotherapy to maximize durable bladder preservation and reduce the risk of recurrence and progression?
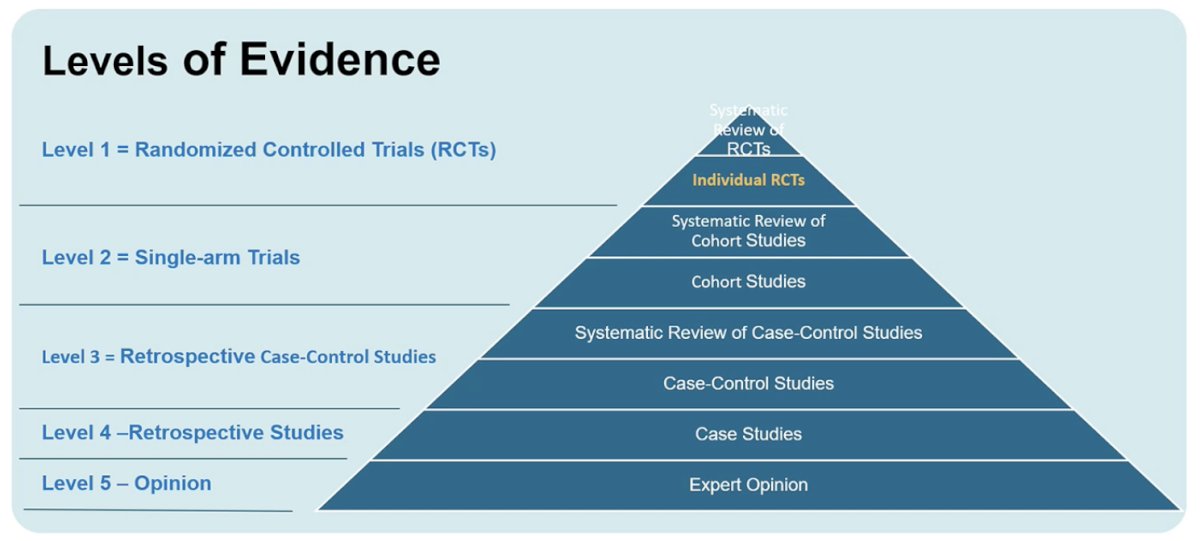
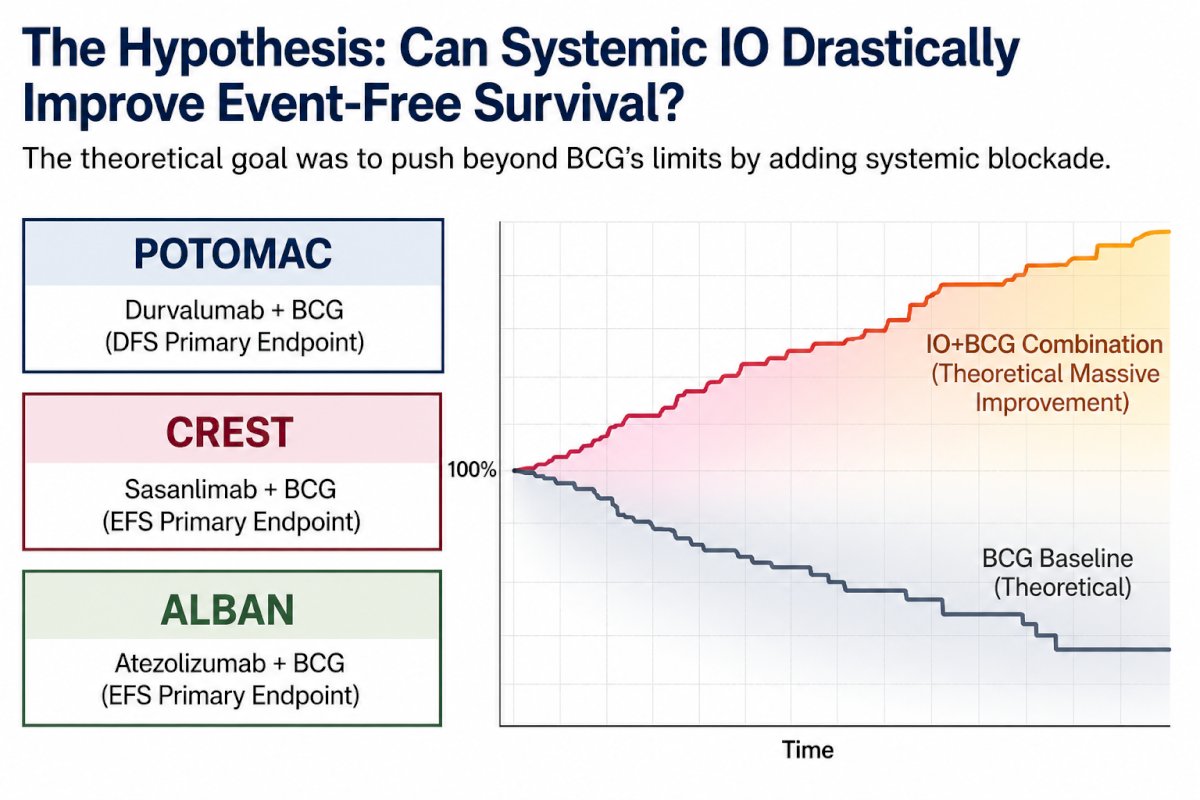
Arguing in favor of BCG + IO, Dr. Neal Shore began by explicitly anchoring his position in levels of evidence. His opening slide contrasted randomized controlled trials as level 1 evidence with progressively weaker forms of data, making clear that his argument rested not on retrospective enthusiasm or single-arm signal seeking, but on three fully accrued phase III randomized studies in the BCG-naïve, high-risk NMIBC space: CREST, POTOMAC, and ALBAN.1-3
He noted that all three studies asked broadly similar questions but did so in somewhat different populations and with different treatment backbones, which is critical when interpreting why two were positive and one was not.
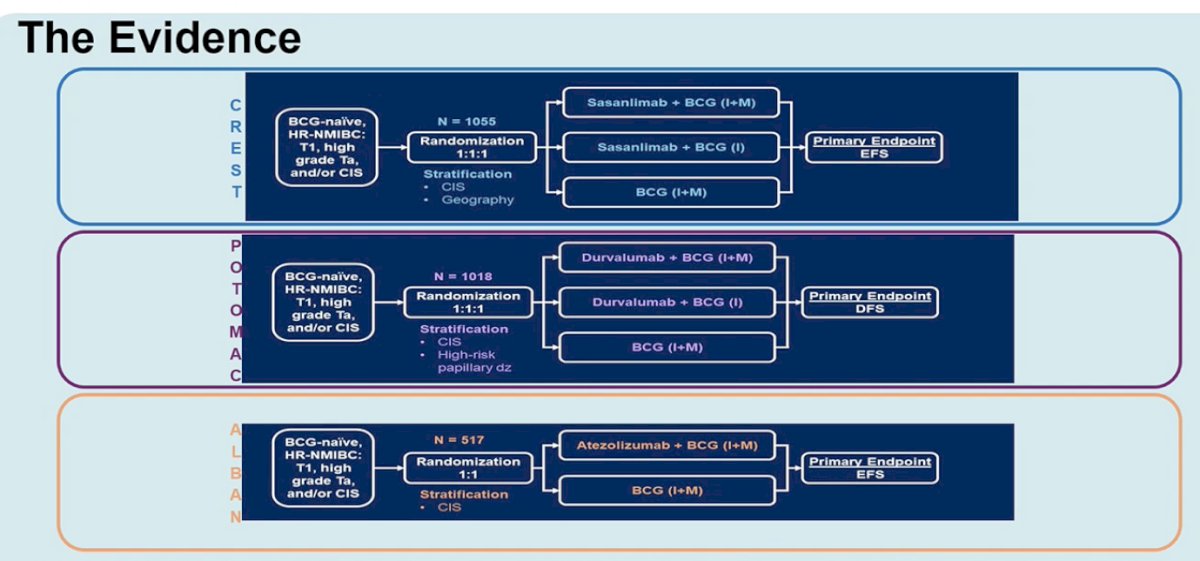
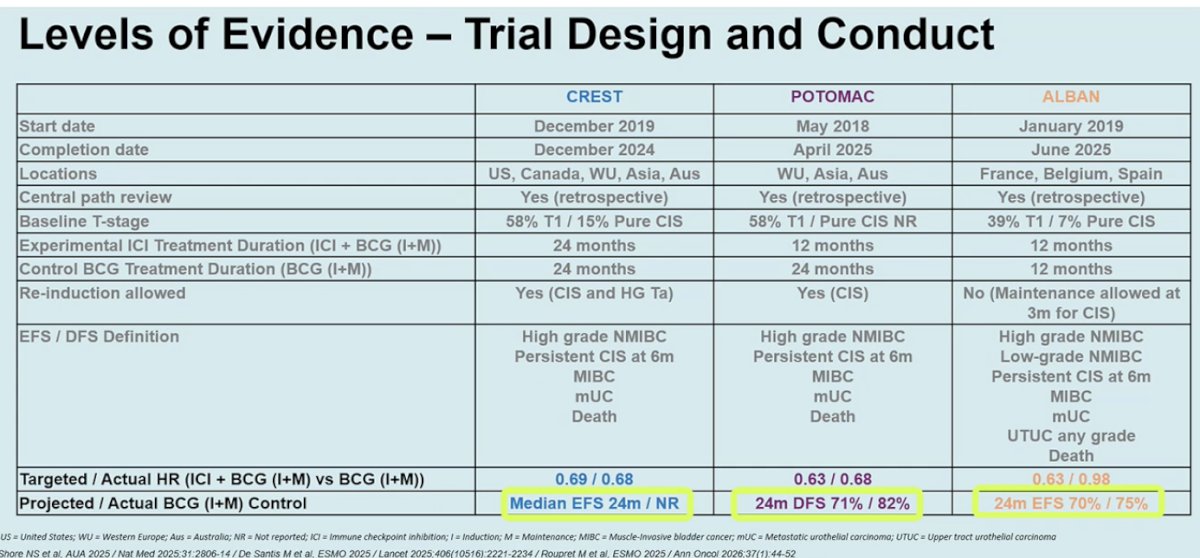
Dr. Shore reviewed the three pivotal phase III trials evaluating this strategy. CREST randomized 1,055 patients to sasanlimab plus BCG induction and maintenance, sasanlimab plus BCG induction only, or BCG induction and maintenance alone, with event-free survival as the primary endpoint. POTOMAC randomized 1,018 patients to durvalumab plus BCG induction and maintenance, durvalumab plus BCG induction only, or BCG induction and maintenance alone, with disease-free survival as the primary endpoint. ALBAN randomized 517 patients to atezolizumab plus BCG versus BCG alone. Dr. Shore emphasized that CREST and POTOMAC enrolled a particularly high-risk population, with approximately 58% of patients harboring T1 disease, and both used a robust 24-month BCG maintenance backbone.
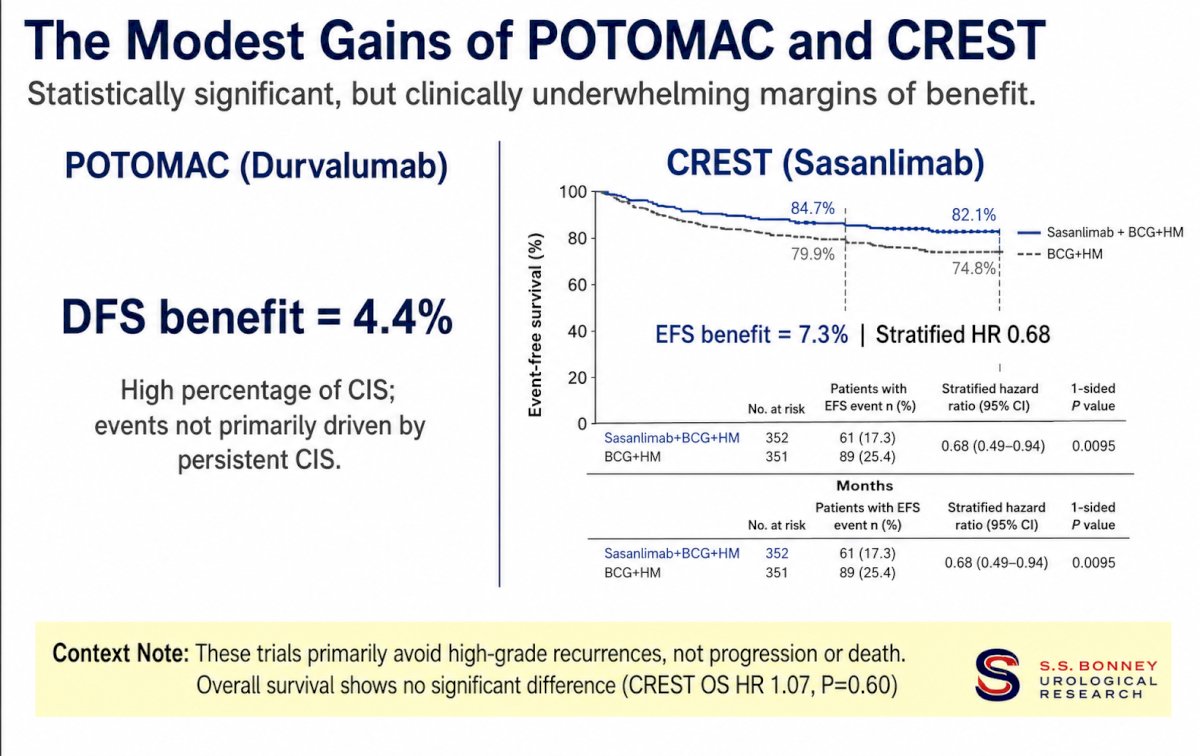
In CREST, sasanlimab plus BCG significantly improved event-free survival, with a hazard ratio of 0.68 (95% CI 0.49–0.94; one-sided p=0.0095). Median event-free survival was 24 months with BCG alone and was not reached with combination therapy. At 36 months, event-free survival was 82.1% with sasanlimab plus BCG compared with 74.8% with BCG alone, representing an absolute benefit of 7.3%. In POTOMAC, durvalumab plus BCG yielded a nearly identical hazard ratio of 0.68, with 24-month disease-free survival improving from 71% with BCG alone to 82% with combination therapy, corresponding to an absolute benefit of approximately 4.4%. In contrast, ALBAN was negative, with an event-free survival hazard ratio of 0.98 and no meaningful benefit. Dr. Shore argued that the concordant positive findings in CREST and POTOMAC provide level 1 evidence that immune checkpoint inhibition can augment the anti-tumor activity of BCG.
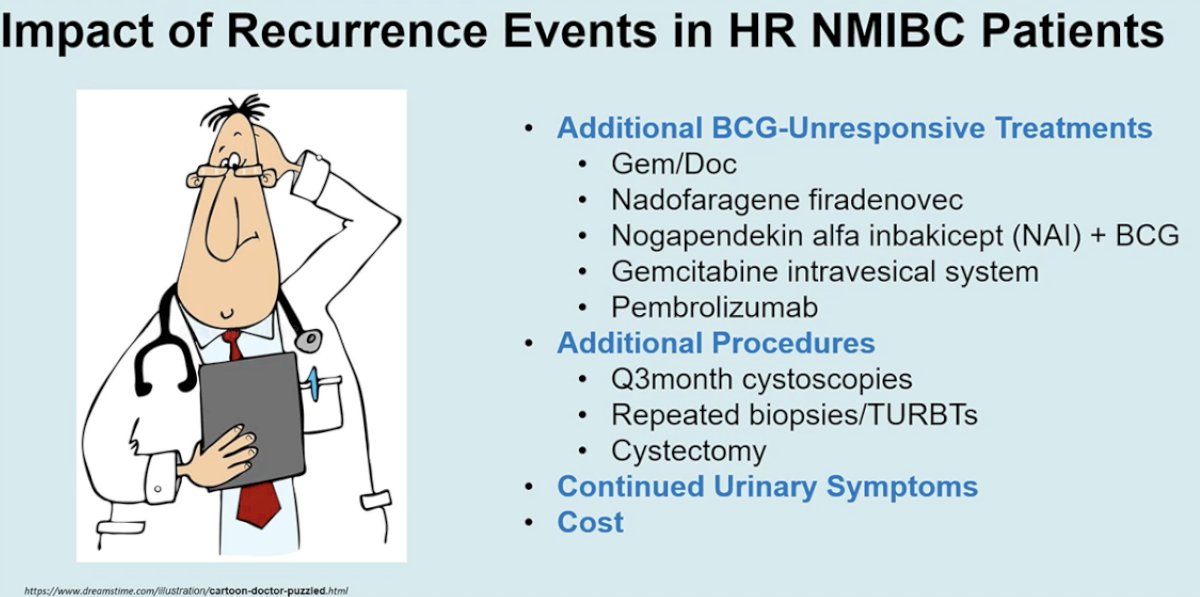
From there, Dr. Shore shifted the discussion from hazard ratios to clinical consequences. One of his more practical slides focused on what recurrence actually means for a patient with high-risk NMIBC. He reminded the audience that recurrence is not a trivial bookkeeping event; rather, it often initiates an entirely new and more burdensome therapeutic pathway. The slide below summarizes the familiar downstream consequences of recurrent or newly BCG-unresponsive disease: additional salvage therapies such as gemcitabine/docetaxel, nadofaragene firadenovec; more frequent cystoscopies; repeated biopsies and TURBTs; ongoing urinary symptoms; greater cost; and, not infrequently, eventual cystectomy. In other words, his argument was that preventing the first high-risk recurrence has value beyond the primary endpoint because it may prevent the entire cascade of subsequent procedures, treatments, symptoms, and anxiety that follows.
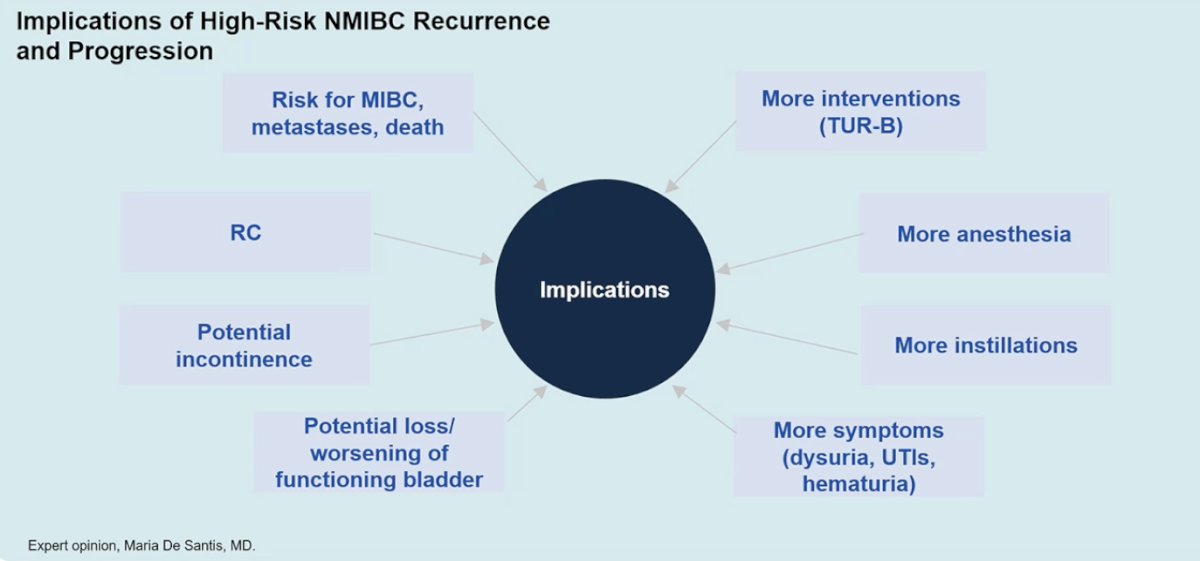
This point was reinforced by a subsequent slide mapping the broad implications of high-risk recurrence and progression, including risk of muscle-invasive disease, metastases, death, additional anesthesia exposure, repeated resections, more intravesical treatments, worsening urinary symptoms, potential incontinence, and possible deterioration of bladder function.
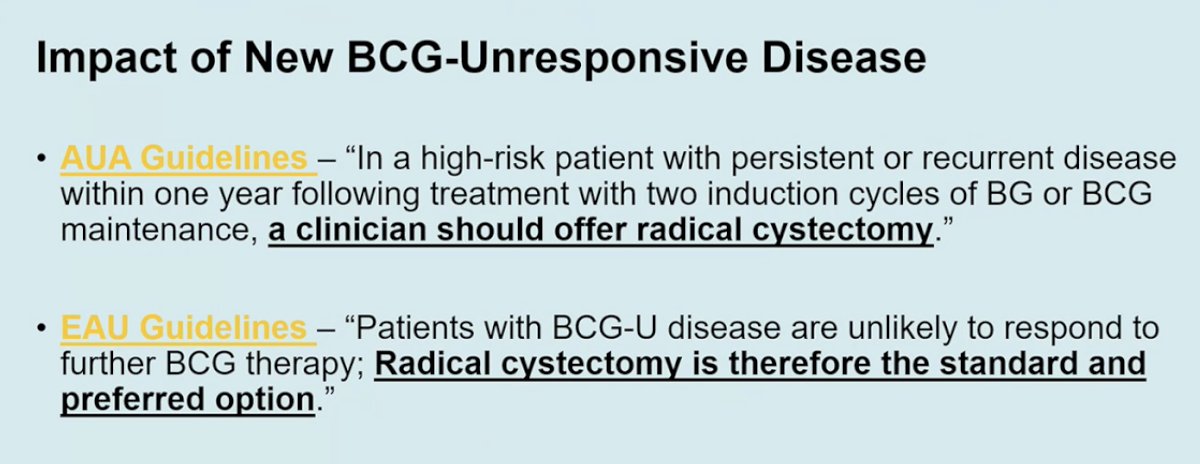
Dr. Shore then connected these recurrence consequences to contemporary guideline language for BCG-unresponsive disease. He showed that once a patient enters that state, the threshold for recommending radical cystectomy becomes much lower. His slide quoted both AUA and EAU guidance to emphasize that persistent or recurrent high-risk disease after adequate BCG frequently leads to a recommendation for cystectomy, with the EAU explicitly describing radical cystectomy as the standard and preferred option in BCG-unresponsive disease. His underlying point was that if BCG plus IO can reduce the risk of those high-risk recurrence events upfront, it may spare some patients from ever entering a disease state in which radical surgery becomes the default recommendation.
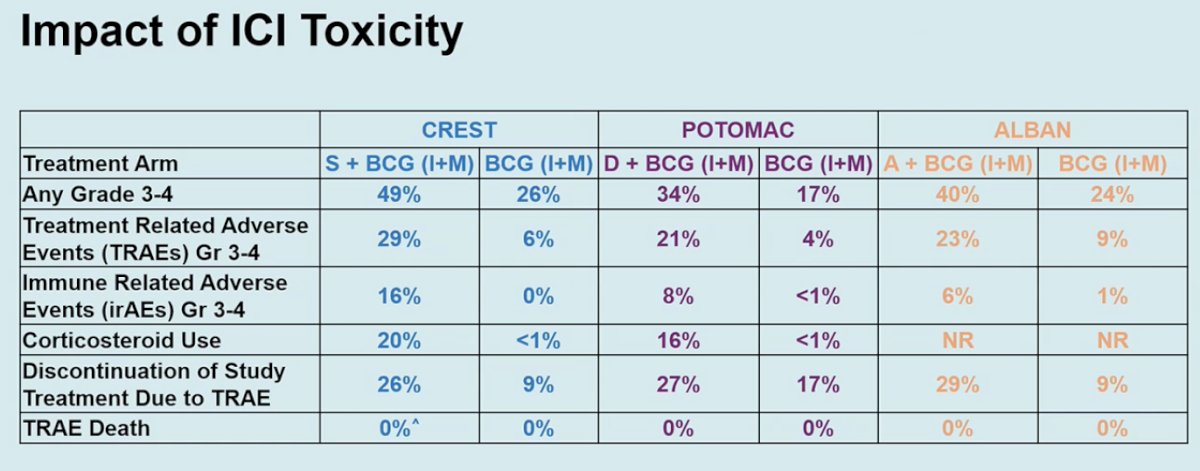
Dr. Shore acknowledged that IO intensification in this setting is associated with increased toxicity. In CREST, the addition of sasanlimab to BCG increased grade 3–4 adverse events from 26% to 49%, grade 3–4 treatment-related adverse events from 6% to 29%, grade 3–4 immune-related adverse events from 0% to 16%, corticosteroid use from less than 1% to 20%, and treatment discontinuation due to TRAEs from 9% to 26%.
In POTOMAC, durvalumab plus BCG increased grade 3–4 treatment-related adverse events from 4% to 21%, and in ALBAN, the atezolizumab combination also produced higher rates of TRAEs and grade 3 or higher TRAEs than BCG alone. Nonetheless, Dr. Shore noted that these added risks were ‘acceptable’ in a carefully selected population at the highest risk of progression and metastasis, particularly when weighed against the clinical impact of recurrence, BCG-unresponsive disease, and eventual cystectomy, and that many of these toxicities can be safely managed in the outpatient setting by either experienced urologists or medical oncologists.
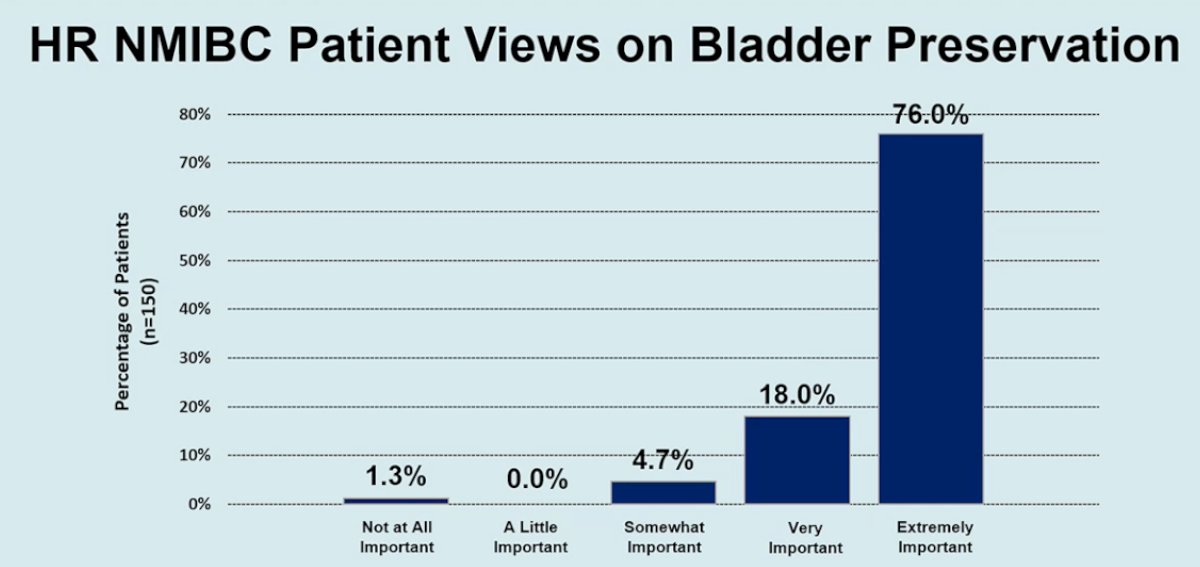
But what really matters to patients, such as the one in the initial case study? Dr. Shore showed a patient-preference slide indicating that bladder preservation is highly valued by this population, with 76% of patients rating bladder preservation as “extremely important” and another 18% rating it “very important.”4 He used this not to argue against evidence-based care, but to frame why shared decision-making matters so much in this disease state. If a patient places enormous value on bladder preservation, and if level 1 evidence now suggests that adding checkpoint inhibition to BCG can improve event-free or disease-free outcomes in a subset of high-risk BCG-naïve patients, then that combination deserves to be part of the conversation rather than reserved as a fringe option.
His final arguments, therefore, moved away from a one-size-fits-all recommendation and toward a personalized treatment framework. He showed a decision-making schema centered on disease characteristics, efficacy profile, safety and tolerability, treatment schedule and duration, access and cost, patient comorbidities, patient preferences and quality of life, and the importance of management by informed specialists. This was an important refinement of his “pro” position: he was not arguing that every patient with high-risk BCG-naïve NMIBC must receive BCG + IO, but rather that the field now has sufficiently strong evidence to justify offering it to appropriate patients, especially those at highest biologic risk.

Dr. Shore concluded his argument in favor of BCG+IO for BCG-naïve, high-risk NMIBC patients as follows:
- Level 1 evidence now supports the addition of immune checkpoint inhibition to intravesical BCG in BCG-naïve high-risk NMIBC
- This combination provides meaningful clinical benefit with an acceptable risk profile in patients at highest risk of recurrence, progression, and metastasis
- Shared decision-making remains the standard of care
Taken together, he argued that BCG+IO should no longer be viewed as speculative intensification, but as a logical next step in the management of select patients with BCG-naïve high-risk NMIBC.
Dr. Morgan Rouprêt presented the opposing viewpoint, arguing that routine addition of systemic immunotherapy to BCG in 2026 represents clinical overreach rather than true progress. His central thesis was that BCG-naïve high-risk NMIBC remains a localized disease for which contemporary induction and maintenance BCG already provides excellent oncologic outcomes with limited toxicity, low cost, and manageable logistics. In this context, any new strategy must deliver substantial and clinically meaningful benefit to justify exposing patients to systemic therapy and immune-related adverse events.
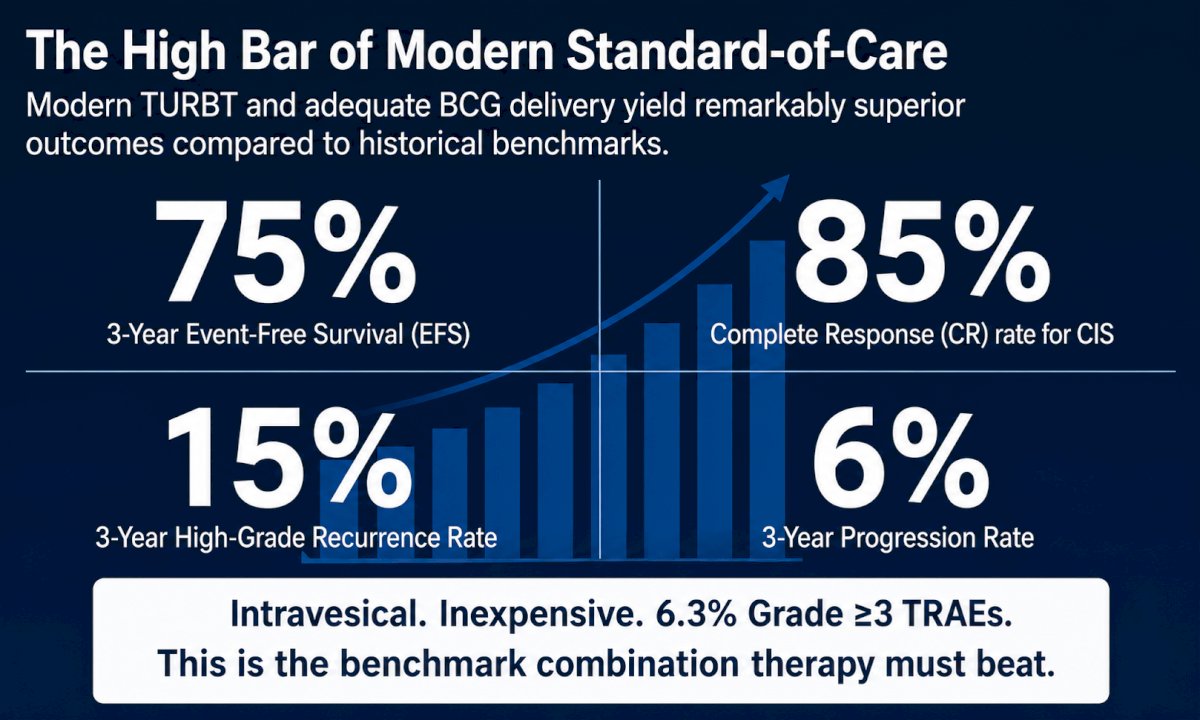
Dr. Rouprêt began by establishing the benchmark against which all new combinations must be judged. Drawing on contemporary data, he noted that optimized TURBT followed by adequate BCG maintenance yields approximately 75% 3-year event-free survival, an 85% complete response rate for carcinoma in situ, a 15% 3-year high-grade recurrence rate, and only a 6% 3-year progression rate. These outcomes are achieved with a grade ≥3 treatment-related adverse event rate of just 6.3%. He emphasized that BCG remains a localized, inexpensive, and logistically sustainable therapy, making it an exceptionally high bar for any new treatment approach to surpass.
He then reviewed the three pivotal randomized phase III trials evaluating BCG plus immune checkpoint inhibition: ALBAN (atezolizumab plus BCG), POTOMAC (durvalumab plus BCG), and CREST (sasanlimab plus BCG). Dr. Rouprêt focused first on ALBAN, which he considered the most direct test of the underlying hypothesis. ALBAN randomized 516 patients with BCG-naïve high-risk NMIBC to atezolizumab plus BCG (n=262) or BCG alone (n=255) and was powered to detect a 10% absolute improvement in 3-year event-free survival. The study was unequivocally negative, with an event-free survival hazard ratio of 0.98 (95% CI 0.71–1.36; p=0.9106) and no absolute 3-year benefit. Importantly, subgroup analyses failed to identify any “hidden” beneficiary population, with no clinically meaningful advantage observed according to stage (T1 versus Ta), presence of carcinoma in situ, age ≥65 years, or sex.
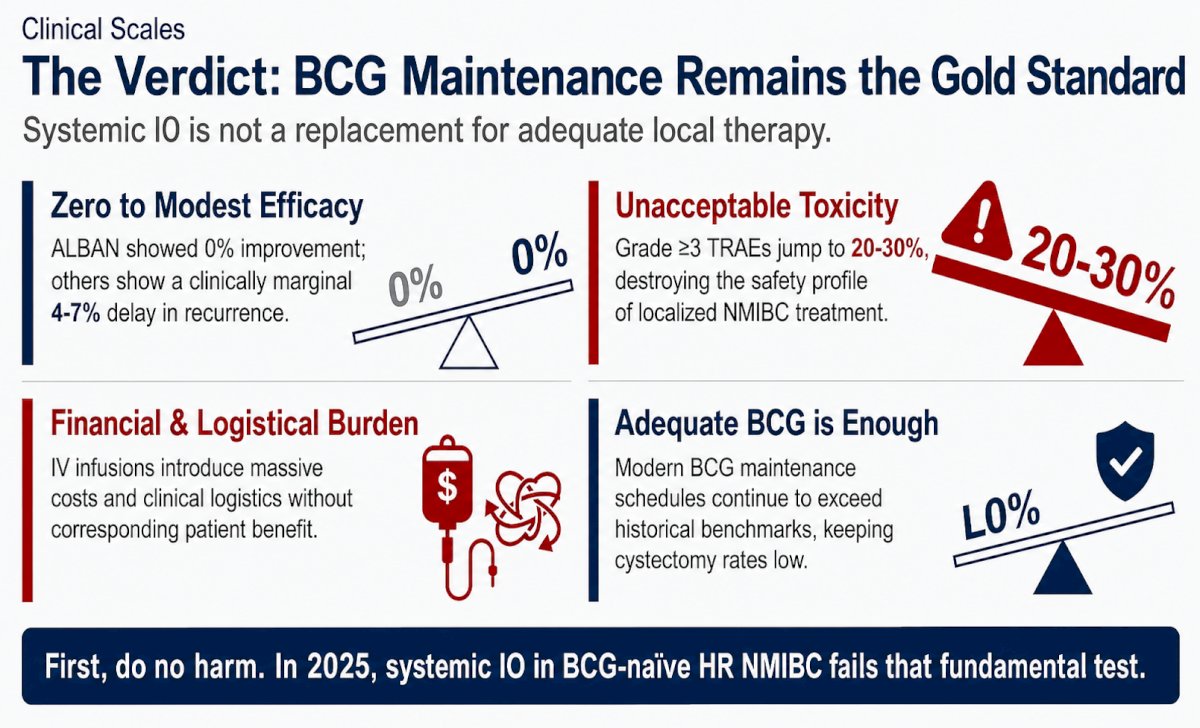
Dr. Rouprêt then turned to POTOMAC and CREST, acknowledging that both studies met their primary endpoints but emphasizing that the magnitude of benefit was modest. In POTOMAC, durvalumab plus BCG improved disease-free survival by an absolute 4.4%. In CREST, sasanlimab plus BCG improved 36-month event-free survival from 74.8% to 82.1%, corresponding to an absolute benefit of 7.3% and a stratified hazard ratio of 0.68 (95% CI 0.49–0.94; p=0.0095). However, he stressed that these gains were driven primarily by reductions in high-grade recurrence rather than demonstrated decreases in progression, metastasis, or death. In CREST, overall survival was not improved (HR 1.07; p=0.60). His conclusion was that these trials were statistically positive but clinically underwhelming.
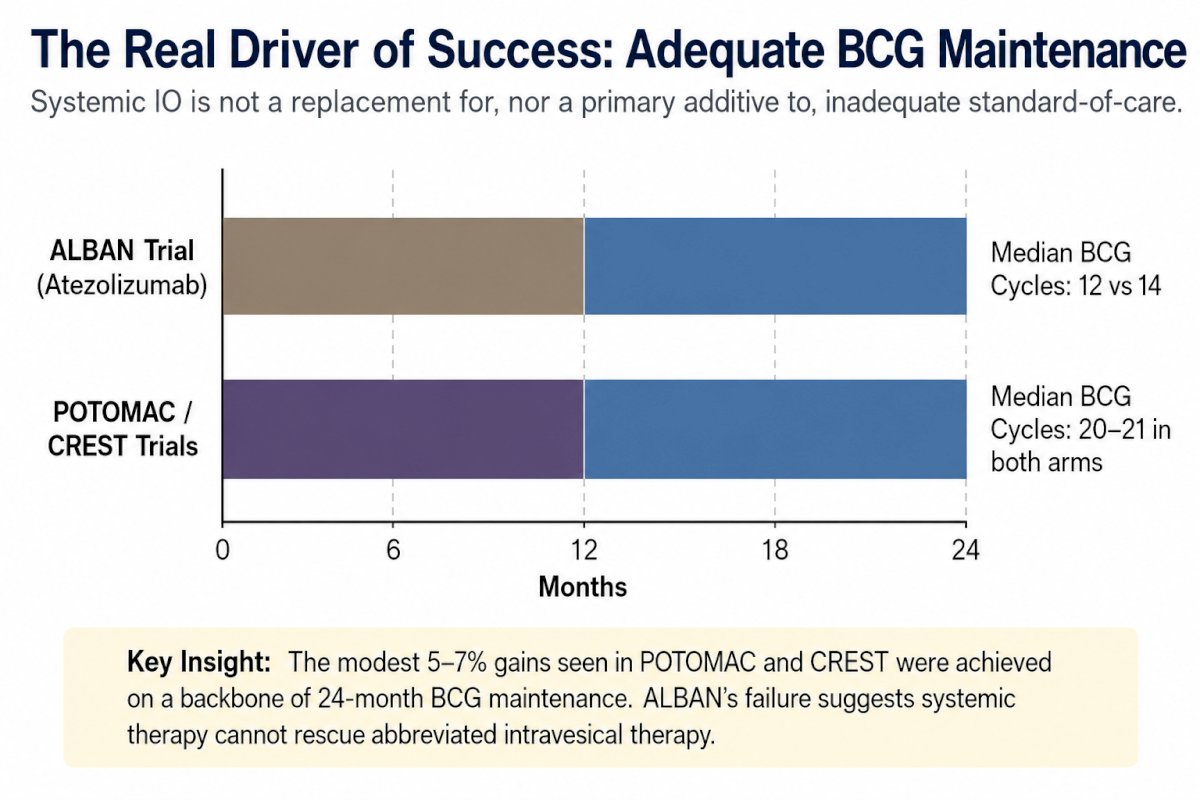
A major focus of Dr. Rouprêt’s presentation was the critical importance of adequate BCG maintenance. He noted that ALBAN incorporated 12 months of maintenance BCG, with median exposure of 12–14 cycles, whereas both POTOMAC and CREST employed 24 months of maintenance, with median BCG exposure of approximately 20–21 cycles in both treatment arms. In his view, the modest 4–7% improvements observed in POTOMAC and CREST were achieved on the foundation of prolonged, optimized BCG administration and may reflect the effectiveness of the intravesical backbone as much as, if not more than, the contribution of systemic immunotherapy. As he summarized, systemic therapy cannot compensate for inadequate intravesical treatment, and optimized maintenance remains the principal determinant of outcome.
Dr. Rouprêt next addressed the toxicity burden associated with immune checkpoint inhibition. Across ALBAN, POTOMAC, and CREST, grade ≥3 treatment-related adverse events increased from approximately 6–9% with BCG alone to roughly 20–30% with combination therapy. In ALBAN, treatment discontinuation due to adverse events occurred in 28.6% of patients receiving atezolizumab plus BCG compared with 8.8% receiving BCG alone, representing a 3.2-fold increase. He argued that clinicians are exposing patients with localized disease to substantial immune-related toxicity primarily to prevent high-grade recurrences rather than to reduce progression or improve survival.
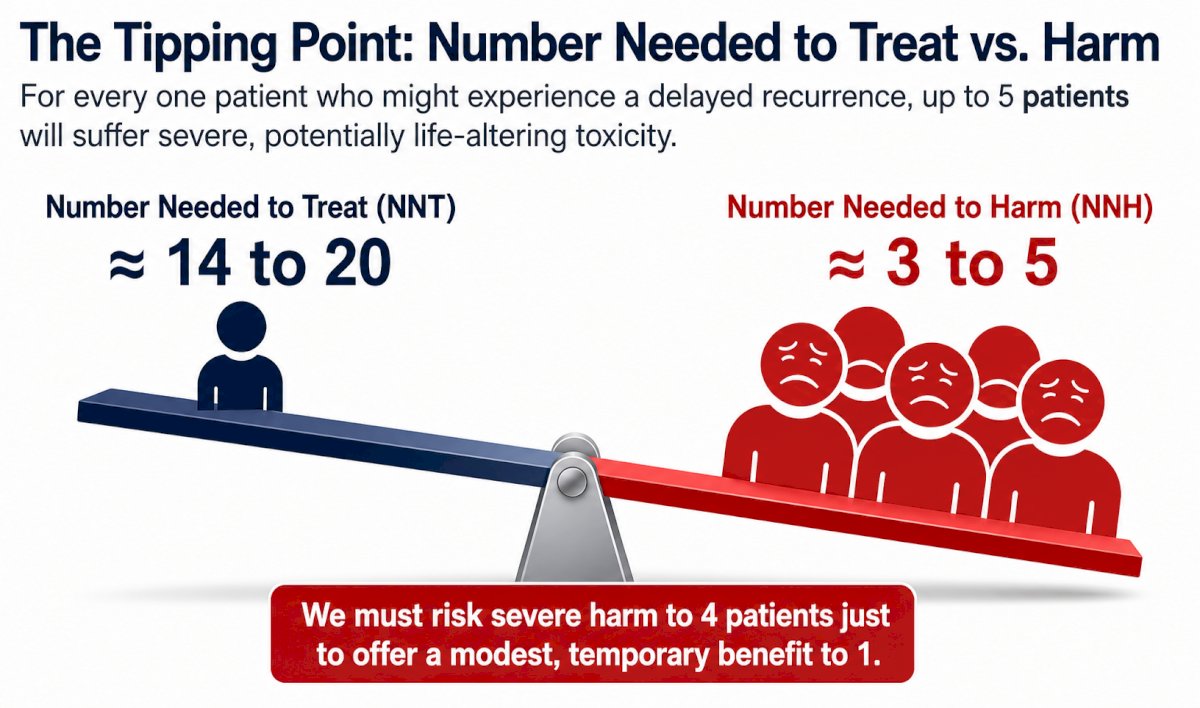
To further illustrate this imbalance, Dr. Rouprêt contrasted the estimated number needed to treat (NNT) with the number needed to harm (NNH). Based on the available trial data, approximately 14–20 patients would need to receive BCG plus immunotherapy to prevent one recurrence event, whereas only 3–5 patients would need to be treated for one to experience severe toxicity. In practical terms, several patients may incur grade ≥3 adverse events for every patient who derives a modest and potentially temporary improvement in recurrence-free outcomes.
He also highlighted the substantial financial and logistical implications of introducing systemic therapy into frontline NMIBC management, including intravenous or subcutaneous administration, infusion-center visits, laboratory monitoring, and management of immune-related adverse events. Given the already excellent outcomes achieved with BCG alone and the expanding availability of effective bladder-sparing options for BCG-unresponsive disease, he questioned whether such added complexity is justified.
Dr. Rouprêt concluded with the memorable MUST framework summarizing why BCG maintenance remains the preferred frontline strategy: Maintenance achieves excellent efficacy; Unexpensive and logistically sustainable therapy; Second-line effective intravesical therapies are now available for BCG failure; and Tolerable safety profile. His final message was unequivocal: until predictive biomarkers identify a clearly defined subgroup with substantial benefit, the routine addition of systemic immunotherapy to BCG in BCG-naïve high-risk NMIBC remains a clinical overreach rather than a new standard of care.
Presented by:
- Mark Tyson, MD, MPH, Associate Professor, Department of Urology, Mayo Clinic, Phoenix, AZ
- Neal Shore, MD, FACS, Urologist, Director, CPI, Carolina Urologic Research Center, Atlantic Urology Clinics, Myrtle Beach, SC
- Morgan Rouprêt, MD, PhD, Professor, Department of Urology, Pitié-Salpétrière Hospital, Paris, France
Written by: Rashid K. Sayyid, MD, MSc, Assistant Professor, Urologic Oncologist, Department of Urology at The University of Arizona and Banner University Medical Center, Tucson, AZ – @rksayyid on X during the American Urological Association (AUA) 2026 Annual Meeting, Washington, DC, Fri, May 15 – Mon, May 18, 2026.
References:
- De Santis M, Palou Redorta J, Nishiyama H, et al. Durvalumab in Combination With BCG for BCG-Naive, High-Risk, Non-Muscle-Invasive Bladder Cancer (POTOMAC): Final Analysis of a Randomised, Open-Label, Phase 3 Trial. Lancet. 2025;406(10516):2221-2234.
- Shore ND, Powles TB, Bedke J, et al. Sasanlimab Plus BCG in BCG-Naive, High-Risk Non-Muscle Invasive Bladder Cancer: The Randomized Phase 3 CREST Trial. Nat Med. 2025;31(8):2806-2814.
- Roupret M, Palou J, De Santis M, et al. ALBAN (GETUG-AFU 37): A Phase III, Randomized, Open-Label International Trial of Intravenous Atezolizumab and Intravesical Bacillus Calmette-Guérin (BCG) Versus BCG Alone in BCG-Naive High-Risk Non-Muscle-Invasive Bladder Cancer (NMIBC). Ann Oncol. 2025;36(1):27-35.