(UroToday.com) The American Urological Association's 2026 Annual Meeting, between May 15 – May 18, 2026 in Washington D.C., was host to the AUA-IBCG Bladder Cancer Forum. Drs. Mario Fernandez; Joan Palou and Akshay Sood debated on the Best Practices for intermediate-risk non-muscle invasive bladder cancer (NMIBC).
Dr. Fernandez began by presenting the case of a 78-year-old male with a 15-pack-year smoking history and medical comorbidities, including coronary artery disease and dyslipidemia. In February 2024, the patient was found to have a 2 cm papillary bladder tumor along with three satellite lesions, while urine cytology was negative. The patient subsequently underwent TURBT followed by immediate intravesical chemotherapy, with pathology demonstrating low-grade Ta disease.
The patient declined additional adjuvant therapy following initial treatment. At 6-month surveillance cystoscopy, several recurrent lesions measuring up to 5 mm were identified in the bladder dome, as shown below:
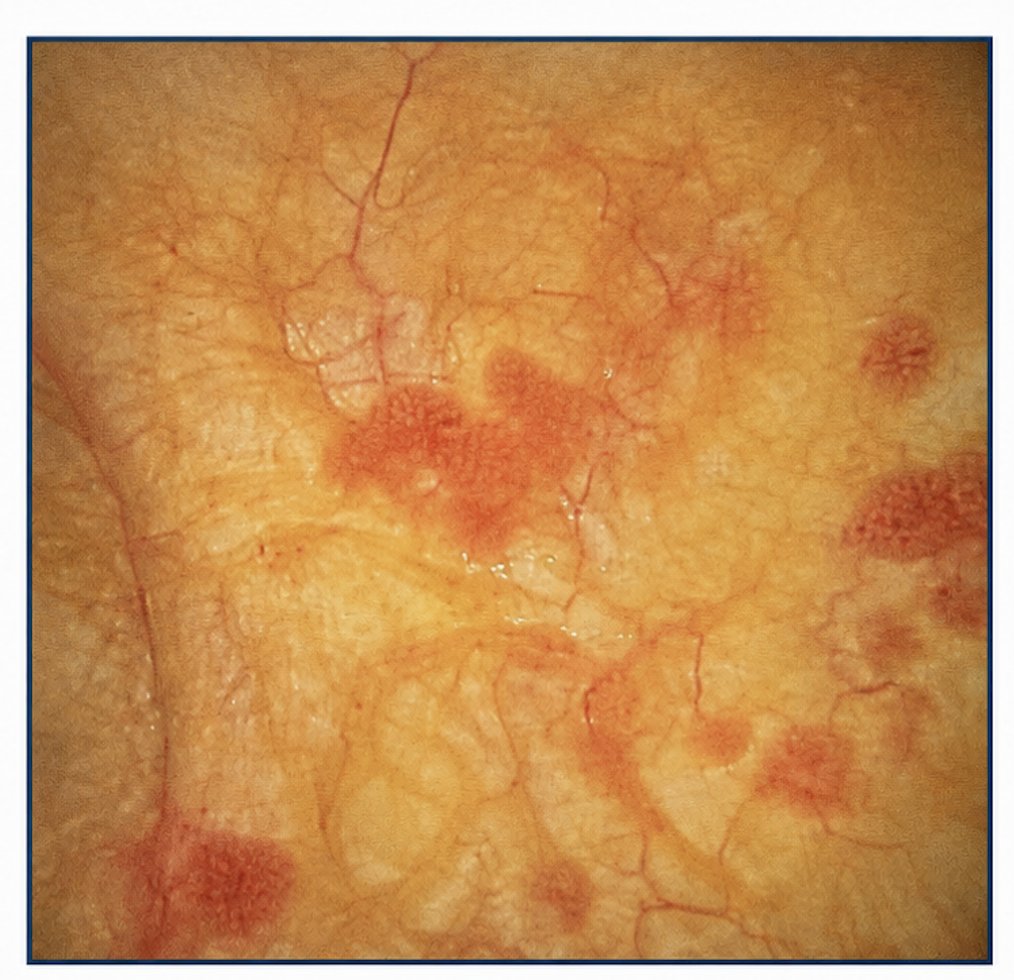
Repeat TURBT confirmed multifocal recurrent low-grade Ta disease occurring within 1 year of initial diagnosis. Based on tumor focality and early recurrence, the patient was classified as having intermediate-risk NMIBC with two established risk factors.
Ablation / Active Surveillance for IR NMIBCDr. Sood reviewed the natural history of low-grade intermediate-risk NMIBC, emphasizing the substantial long-term risk of recurrence despite the relatively low risk of progression. He highlighted that patients treated with TURBT alone experience an estimated 7-year recurrence risk approaching 60%, while the risk of progression to high-grade T1 disease remains below 10%, and the risk of developing muscle-invasive bladder cancer is less than 3% over 7 years. (1) He noted that these data likely reflect the true natural history of low-grade Ta disease, as patients in these historical series were managed with TURBT alone without adjuvant intravesical therapy.
He further discussed the impact of overtreatment in recurrent low-grade bladder cancer, emphasizing that repeated TURBTs and escalating interventions may expose patients to substantial cumulative burden despite the relatively low risk of disease progression. Key concerns highlighted included TURBT-related morbidity, complications, and side effects associated with repeated general anesthesia exposure, psychological and quality-of-life consequences related to recurrent hospital visits and operating room procedures, and the broader economic burden associated with long-term NMIBC management. Dr. Sood emphasized that these considerations support efforts toward treatment deintensification strategies in recurrent low-grade disease.2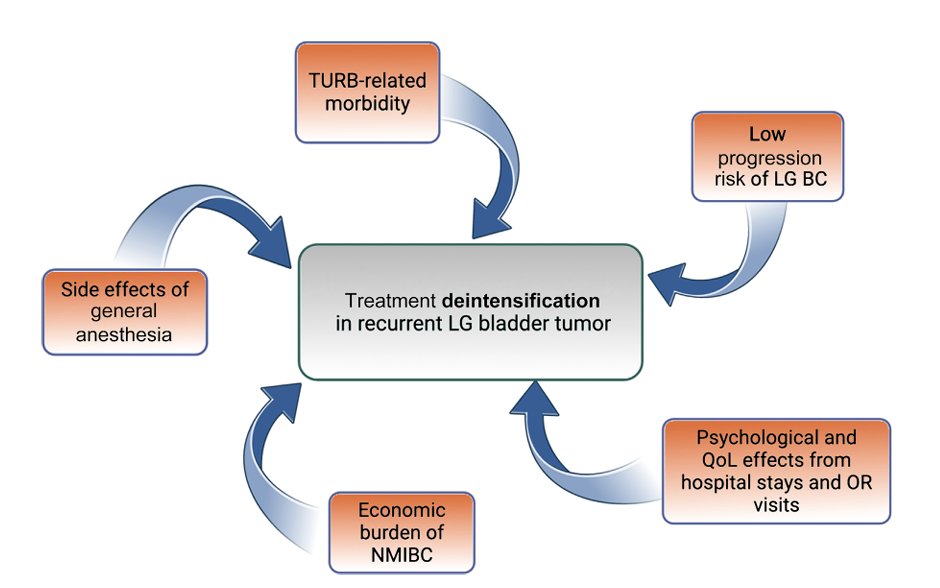
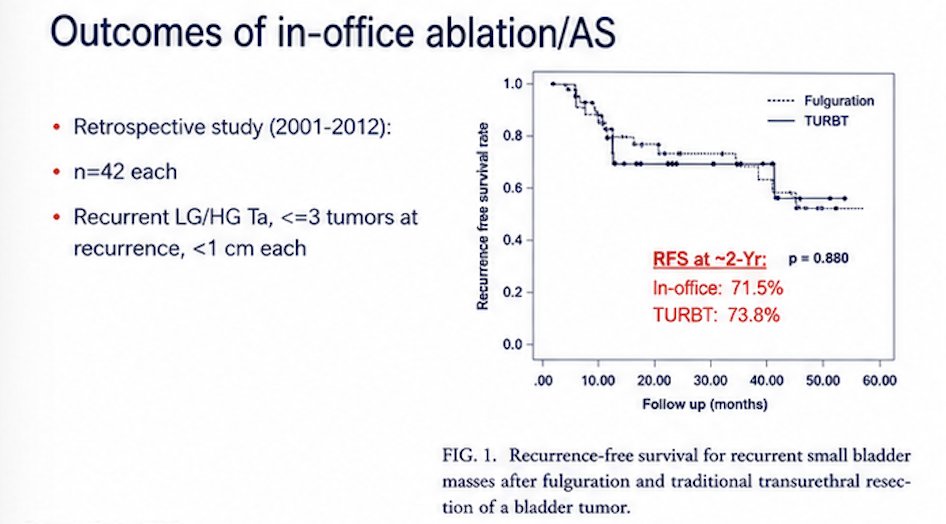
Dr. Sood also reviewed outcomes associated with in-office fulguration and active surveillance strategies for recurrent small bladder tumors. He highlighted a retrospective study conducted between 2001 and 2012 that included 42 patients treated with in-office fulguration and 42 undergoing TURBT. Eligible patients had recurrent low- or high-grade Ta disease with ≤3 tumors at recurrence, each measuring <1 cm. Recurrence-free survival outcomes were comparable between approaches, with approximately 2-year recurrence-free survival rates of 71.5% for in-office treatment versus 73.8% for TURBT (p=0.880), supporting the feasibility of less invasive management strategies in carefully selected patients. He further emphasized that in this study in Korea, the Mean total medical cost was $393.3 vs $1164.6 (p<0.001), favouring in-office fulguration, endorsing the potential cost-effectiveness of in-office fulguration, particularly given the reduced need for operating room utilization, anesthesia, hospital visits, and procedural morbidity compared with repeat TURBT.3
Moreover, Dr. Sood highlighted prospective randomized data evaluating in-office laser ablation and active surveillance strategies for recurrent intermediate-risk NMIBC. The trial, conducted between 2016 and 2022, enrolled 300 patients with recurrent multifocal low-grade Ta disease, with lesions measuring <1.5 cm each. Patients were randomized to in-office management versus TURBT. At 1 year, recurrence-free survival rates were nearly identical between groups at 43.5% for in-office treatment and 43.0% for TURBT. Importantly, progression-free survival at 1 year was 100%, further supporting the oncologic safety of carefully selected bladder-sparing, office-based management approaches in recurrent low-grade IR-NMIBC.4

He further discussed the ATLAS trial, a prospective randomized study evaluating UGN-102 in patients with new or recurrent low-grade intermediate-risk NMIBC. The trial enrolled 282 patients, representing less than 50% of the originally planned accrual, with diagnosis established using office cold-cup biopsy. Patients were randomized to receive six planned instillations of UGN-102 versus TURBT alone. Baseline characteristics demonstrated a substantial proportion of patients with multifocal disease and tumors >3 cm, reflecting a clinically relevant intermediate-risk population as shown in the table below. Dr. Sood highlighted the growing interest in gel-based chemoablative approaches as a potential bladder-sparing alternative capable of reducing repeat operative interventions in carefully selected patients with recurrent low-grade disease.5

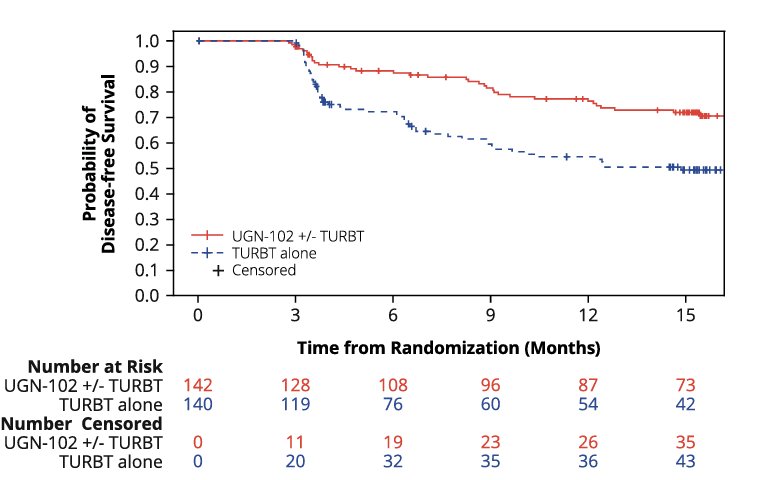
Notably, in the ATLAS trial, treatment with UGN-102 ± TURBT was associated with improved disease-free survival compared with TURBT alone. At 15 months, disease-free survival was 72% in the UGN-102 arm versus 50% in the TURBT-alone arm, corresponding to a hazard ratio of 0.45. Dr. Sood also noted that serious treatment-emergent adverse events occurred in 8.7% of patients treated with UGN-102 compared with 5.3% in the TURBT arm.5
Furthermore, he discussed the ENVISION trial, a prospective single-arm study evaluating UGN-102 in patients with recurrent low-grade intermediate-risk NMIBC.6 Unlike ATLAS, which randomized patients against TURBT, ENVISION focused exclusively on recurrent disease and evaluated the activity of chemoablation with six planned instillations of UGN-102. The study enrolled 240 patients, with approximately 80% harboring multifocal tumors and nearly 80% demonstrating an aggregate tumor burden ≤3 cm.6
Among treated patients, complete response was achieved in 191 patients, corresponding to a complete response rate of 79.6% (95% CI: 73.9–84.5). Residual disease was observed in 15%, while progression to high-grade disease occurred in only 2.9% of patients. Dr. Sood highlighted these findings as further evidence supporting chemoablative strategies as a potential bladder-sparing alternative for carefully selected patients with recurrent low-grade IR-NMIBC.
He also discussed TAR-based chemoablative approaches targeting FGFR-altered disease. Dr. Sood highlighted that FGFR3 mutations are present in approximately 70–80% of low-grade NMIBC, providing a strong biologic rationale for targeted intravesical therapy in this population. TAR-210, an intravesical erdafitinib drug-releasing system, was specifically designed to provide sustained local delivery of FGFR inhibition within the bladder. In patients with intermediate-risk NMIBC harboring FGFR genetic alterations, TAR-210 achieved a complete response rate of 89% at 6 months in a cohort of 62 patients, further supporting the promise of biomarker-driven bladder-sparing strategies in low-grade disease.
Additionally, Dr. Sood highlighted emerging oral molecularly guided ablative therapies, including dabogratinib, which are currently under investigation and have demonstrated success rates approaching 80% in early studies, further expanding the landscape of personalized, bladder-preserving treatment approaches for low-grade IR-NMIBC.
Lastly, he emphasized that management strategies for recurrent low-grade IR-NMIBC should increasingly reflect the real-world practices already being adopted by expert opinion leaders, including his counterpart in the debate, Dr. Palou. He presented a risk-adapted treatment algorithm favoring de-intensification strategies for carefully selected patients with recurrent low-grade disease.7 Following initial TURBT and surveillance cystoscopy, patients with recurrence but a high probability of persistent low-grade disease may be managed with active surveillance, office fulguration/laser ablation, or TURBT depending on tumor burden and clinical features. He highlighted that active surveillance may be particularly appropriate in patients with ≤2 IBCG intermediate-risk factors and low tumor burden, whereas TURBT should remain reserved for lesions with high-grade appearance, positive urine cytology, or tumors >2–3 cm in diameter.


Dr. Palou acknowledged that both the AUA and EAU guidelines support active surveillance and office fulguration as acceptable management options for selected patients with recurrent low-grade IR-NMIBC. However, he challenged whether clinicians should move away from a “good old TURBT,” emphasizing that complete endoscopic resection remains a highly effective and familiar strategy. He further argued that adjuvant intravesical treatment provides meaningful clinical benefit, citing evidence from two studies supporting reductions in recurrence risk with postoperative therapy following TURBT.
Dr. Palou further reviewed data supporting adjuvant mitomycin C (MMC) in intermediate-risk NMIBC, highlighting evidence from a systematic review and meta-analysis evaluating more than 4,500 patients treated with MMC. He noted that higher MMC doses (40 mg versus 20–30 mg) appeared more effective and emphasized that induction plus maintenance therapy yielded superior outcomes compared with induction alone. Importantly, maintenance schedules of 3–6 months appeared to provide recurrence-free survival outcomes comparable to 1 year of maintenance therapy. Overall, adjuvant MMC improved recurrence-free survival compared with TURBT alone, while the risk of progression remained very low in this population.
Using the IBCG stratification model, Dr. Palou suggested that patients with a single risk factor may reasonably receive induction therapy alone, whereas those with two or more risk factors may derive greater benefit from induction followed by maintenance intravesical therapy.
Moreover, he discussed enhanced detection modalities aimed at improving visualization and reducing missed disease in NMIBC. Dr. Palou highlighted prospective multicenter observational data comparing blue-light cystoscopy (BLC) with white-light cystoscopy (WLC) in 283 patients across eight centers. The study demonstrated improved detection sensitivity with BLC, particularly for CIS, where sensitivity approached 99% compared with approximately 70% for WLC. He emphasized that BLC may be especially useful in patients with multifocal Ta lesions and in cases where occult high-grade disease or CIS is suspected, potentially improving staging accuracy and guiding more appropriate treatment selection.10
Lastly, he presented his practical treatment algorithm for patients with recurrent low-grade IR-NMIBC. For patients with fewer than three small tumors, he favored less invasive approaches such as office fulguration or chemoablation. In contrast, patients with more than three tumors were recommended to undergo TURBT, preferably with enhanced detection techniques such as photodynamic diagnosis (PDD), followed by adjuvant intravesical therapy. He also emphasized the importance of individualized decision-making in elderly and frail patients, noting that in select cases, conservative management and avoidance of repeated interventions may be the most appropriate strategy.
Dr. Fernandez then opened the discussion by focusing on which patients with recurrent low-grade IR-NMIBC may safely postpone or avoid repeat TURBT. Dr. Palou emphasized the importance of performing an optimal initial TURBT, arguing that accurate identification of appropriate low-grade candidates at diagnosis is critical to safely offering less invasive management strategies thereafter. He also expressed disagreement with intensive cystoscopic surveillance every 3 months for patients undergoing active surveillance, stating that if clinicians are confident the recurrence represents low-grade disease, surveillance intervals could reasonably be extended to yearly cystoscopy with predefined triggers prompting surgical intervention.
In contrast, Dr. Sood highlighted important differences between practice patterns in the United States and Europe, noting that patients in the U.S. generally prefer closer monitoring. As a result, he continues to follow these patients every 3 months in his practice. Discussing the recently FDA-approved ENVISION data, Dr. Sood emphasized that an excellent upfront TURBT remains essential, while chemoablative strategies may be most appropriate in the recurrent setting rather than as initial therapy.
Dr. Palou additionally stressed the importance of shared decision-making, encouraging clinicians to ask patients about their treatment preferences. He noted that some patients may prefer repeated weekly intravesical instillations, whereas others may favor simpler office-based fulguration approaches, underscoring the need to balance oncologic control, treatment burden, and quality-of-life considerations.
Presented by:
- Mario Fernández, MD, Clínica Alemana Universidad del Desarrollo, Santiago de Chile, Chile
- Joan Palou, MD, Fundacion Puigvert, Universitat Autònoma de Barcelona, Barcelona, Spain
- Akshay Sood, MD, The University of Texas MD Anderson Cancer Center, Houston, TX
References:
- Simon M, Bosset PO, Rouanne M, Benhamou S, Radulescu C, Molinié V, Neuzillet Y, Paoletti X, Lebret T. Multiple recurrences and risk of disease progression in patients with primary low-grade (TaG1) non-muscle-invasive bladder cancer and with low and intermediate EORTC-risk score. PLoS One. 2019 Feb 27;14(2):e0211721. doi: 10.1371/journal.pone.0211721. PMID: 30811419; PMCID: PMC6392242.
- Contieri R, Martini A, Beijert IJ, Mertens LS, Hentschel AE, Bründl J, Compérat EM, Plass K, Rodríguez O, Subiela Henríquez JD, Hernández V, de la Peña E, Alemany I, Turturica D, Pisano F, Soria F, Čapoun O, Bauerová L, Pešl M, Maxim Bruins H, Runneboom W, Herdegen S, Breyer J, Brisuda A, Calatrava A, Rubio-Briones J, Seles M, Mannweiler S, Bosschieter J, Kusuma VRM, Ashabere D, Huebner N, Seisen T, Claps F, Masson-Lecomte A, Liedberg F, Cohen D, Lunelli L, Cussenot O, Sheikh SE, Volanis D, Côté JF, Rouprêt M, Haitel A, Shariat SF, Mostafid AH, Nieuwenhuijzen JA, Zigeuner R, Dominguez-Escrig JL, Hacek J, Zlotta AR, Burger M, Evert M, de Kaa CAH, van der Heijden AG, Kiemeney LALM, Soukup V, Molinaro L, Hurle R, Paciotti M, Moschini M, Pradere B, Perdonà S, Gontero P, Llorente C, Algaba F, Palou J, N'Dow J, Ribal MJ, van der Kwast TH, Babjuk M, Sylvester RJ, van Rhijn BWG. Towards Defining Follow-up Strategies for Patients with Primary Intermediate-risk Non-muscle-invasive Bladder Cancer. Eur Urol Oncol. 2025 Aug;8(4):977-985. doi: 10.1016/j.euo.2025.04.010. Epub 2025 May 21. PMID: 40399193.
- Park DS, Hwang JH, Gong IH, Choi DK, Kang MH, Oh JJ. An analysis of the efficacy, safety, and cost-effectiveness of fulguration under local anesthesia for small-sized recurrent masses: a comparative analysis to transurethral resection of bladder tumors in a matched cohort. J Endourol. 2013 Oct;27(10):1240-4. doi: 10.1089/end.2013.0241. Epub 2013 Aug 21. PMID: 23964922.
- Pedersen GL, Mogensen K, Rosthøj S, Erikson MS, Fode M, Hermann GG. In-Office Laser Coagulation of Ta Bladder Tumor Compared With Transurethral Resection of Bladder Tumor: 12 Months Follow-Up Randomized Clinical Trial. J Urol. 2026 May;215(5):535-543. doi: 10.1097/JU.0000000000004918. Epub 2025 Dec 29. PMID: 41461083.
- Prasad SM, Huang WC, Shore ND, Hu B, Bjurlin M, Brown G, Genov P, Shishkov D, Khuskivadze A, Ganev T, Marchev D, Orlov I, Kopyltsov E, Zubarev V, Nosov A, Komlev D, Burger B, Raju S, Meads A, Schoenberg M. Treatment of Low-grade Intermediate-risk Nonmuscle-invasive Bladder Cancer With UGN-102 ± Transurethral Resection of Bladder Tumor Compared to Transurethral Resection of Bladder Tumor Monotherapy: A Randomized, Controlled, Phase 3 Trial (ATLAS). J Urol. 2023 Oct;210(4):619-629. doi: 10.1097/JU.0000000000003645. Epub 2023 Aug 7. PMID: 37548555; PMCID: PMC12721658.
- Prasad SM, Shishkov D, Mihaylov NV, Khuskivadze A, Genov P, Terzi V, Kates M, Huang WC, Louie MJ, Raju S, Burger B, Meads A, Schoenberg M. Primary Chemoablation of Recurrent Low-Grade Intermediate-Risk Nonmuscle-Invasive Bladder Cancer With UGN-102: A Single-Arm, Open-Label, Phase 3 Trial (ENVISION). J Urol. 2025 Feb;213(2):205-216. doi: 10.1097/JU.0000000000004296. Epub 2024 Oct 24. PMID: 39446087; PMCID: PMC12708048.
- Contieri R, Soloway MS, Gontero P, Herr H, Kassouf W, Mertens LS, Moschini M, O'Donnell M, Palou J, Psutka SP, Rouprêt M, Teoh JYC, Kamat AM. Deintensification of Treatment for Low-grade Bladder Tumors: A Collaborative Review by the International Bladder Cancer Group (IBCG). Eur Urol Oncol. 2025 Feb;8(1):179-189. doi: 10.1016/j.euo.2024.08.001. Epub 2024 Aug 31. PMID: 39218742.
- Li R, Hensley PJ, Babjuk M, Bukavina L, Psutka SP, Lerner SP, O'Donnell MA, Lotan Y, Bree KK, Redorta JP, McConkey DJ, Lee BH, Mariappan P, Mertens LS, Soloway MS, Svatek RS, Tan WS, Williams SB, Gupta S, Buckley R, Kamat AM. Intermediate-risk Non-muscle-invasive Bladder Cancer: Recommendations for Definitions, Risk Stratification, Management Strategies, and Clinical Trial Design from the International Bladder Cancer Group. Eur Urol Oncol. 2025 Dec;8(6):1685-1695. doi: 10.1016/j.euo.2025.08.003. Epub 2025 Oct 10. PMID: 41076366.
- Siva J, et al., Reducing complexity in International Bladder Cancer Group intermediate-risk non-muscle-invasive bladder cancer stratification: a three-factor approach. BJU Int 2026 doi:10.1111/bju.70269
- Maisch P, Koziarz A, Vajgrt J, Narayan V, Kim MH, Dahm P. Blue versus white light for transurethral resection of non-muscle invasive bladder cancer. Cochrane Database Syst Rev. 2021 Dec 1;12(12):CD013776. doi: 10.1002/14651858.CD013776.pub2. PMID: 34850382; PMCID: PMC8632646.