(UroToday.com) The American Urological Association's 2026 Annual Meeting, between May 15 – May 18, 2026 in Washington D.C., was host to the AUA-IBCG Bladder Cancer Forum. Drs. Ashish Kamat and Sarah Psutka presented the Update from the International Bladder Cancer Group (IBCG).
Dr. Kamat began by highlighting the role of the International Bladder Cancer Group (IBCG), which convenes yearly scientific retreat meetings that bring together clinicians, scientists, patient advocates, and industry partners from around the world. He emphasized that these collaborative meetings are designed to generate expert consensus recommendations on key topics in bladder cancer management, with the goal of publishing guidance statements that can be implemented globally in clinical practice.
He emphasized that the IBCG has truly global representation, with members spanning North and South America, Europe, Asia, Australia, and other international regions. Dr. Kamat noted that this broad worldwide participation allows the group to incorporate diverse clinical perspectives, practice patterns, and healthcare realities when developing consensus recommendations for bladder cancer management.

Dr. Kamat subsequently reviewed the IBCG consensus development process. Working groups first create recommendation statements in the spring, followed by pre-meeting voting during the summer, where statements receiving ≥75% approval are accepted. Statements not reaching consensus are then formally debated during the annual retreat in August, followed by a final vote. Post-retreat, statements achieving ≥75% agreement are ultimately published as official consensus recommendations.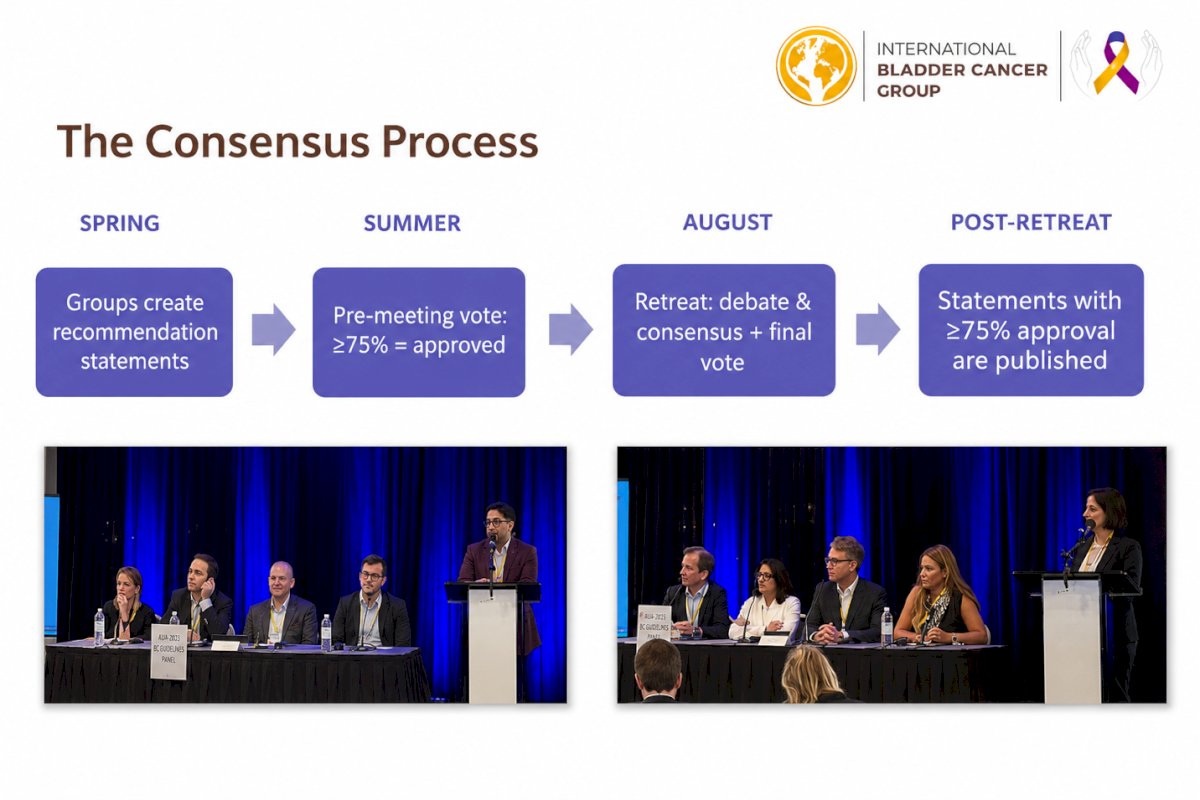
He went on to summarize several of the key topics addressed during prior IBCG retreats and meetings, highlighting the group’s continued efforts to develop evidence-based global recommendations across the spectrum of NMIBC management, including bladder-sparing strategies, BCG-unresponsive disease, surveillance approaches, intravesical therapies, and risk-adapted treatment paradigms.
IBCG23 focused on two major topics. The first centered on bladder-sparing therapies for BCG-unresponsive NMIBC, led by Dr. Roger Li and colleagues, with discussions spanning biomarkers, intravesical chemotherapy, gene therapy, immunotherapy, checkpoint inhibitors, targeted therapies, and strategies to optimize treatment selection and sequencing.1
The second focused on bladder preservation strategies in MIBC, led by Dr. Shilpa Gupta and colleagues, including discussions surrounding partial cystectomy, trimodal therapy, clinical complete response following NAC and/or IO, radical TUR approaches, and patient selection for bladder-preserving management strategies.2
IBCG24
He subsequently highlighted that IBCG24 focused on two additional major areas. The first addressed intermediate-risk NMIBC, including discussions surrounding disease definitions, risk stratification models, management strategies, bladder preservation approaches, and clinical trial design in this increasingly heterogeneous disease space.3
The second focused on the optimal sequencing of therapy in MIBC, including recommendations regarding neoadjuvant and adjuvant chemotherapy, immunotherapy, and other systemic therapies in patients undergoing radical surgery and/or radiation-based bladder preservation approaches.4
IBCG25Lastly, Dr. Kamat reviewed the topics discussed during IBCG25. One major focus centered on biomarkers in urothelial cancer, including early detection and screening, NMIBC risk stratification, intravesical therapy, surveillance strategies, bladder preservation, perioperative therapy in MIBC, germline and somatic mutation testing, metastatic urothelial carcinoma immunotherapy, targeted therapies, and mechanisms of treatment resistance and monitoring. He noted that the corresponding manuscript is currently in press.
The second topic focused on the development of the IBCG-Tx tool designed to assess toxicity associated with local therapies, including surgery, radiation therapy, intravesical therapy, and immunotherapy. He highlighted that the manuscript related to this initiative has already been submitted for publication.
IBCG 26Dr. Kamat concluded by previewing the planned topics for IBCG26, which will focus on optimal consolidation and management strategies following systemic response in urothelial cancer, as well as TURBT best practices for multidisciplinary bladder cancer care.
He also emphasized the important role of patient advocates within the IBCG, noting that they actively participate in the annual retreat and contribute to discussions surrounding patient-centered care, treatment decision-making, quality of life, and research priorities across the bladder cancer disease spectrum.
Improving Patient-Reported Outcome Assessment Across the Spectrum of Bladder Cancer CareDr. Psutka then shifted the discussion toward improving the assessment of patient-reported outcomes (PROs) in bladder cancer care. She noted that one of the major objectives of the IBCG initiative was to determine whether PRO assessment could be better integrated not only into routine clinical practice, but also into contemporary clinical trial design.
She highlighted several important knowledge gaps and unmet needs in the current PRO landscape for bladder cancer, including:
- A large number of existing PRO instruments with limited standardization across studies and clinical settings
- Frequent requirements for patients to complete multiple questionnaires contribute to survey fatigue
- Limited relevance of many questionnaire items from the patient perspective
- Poor assessment of truly patient-centered domains, including treatment burden
- Failure of existing tools to adequately capture outcomes related to newer contemporary therapies
- Limited incorporation of caregiver-relevant outcomes and experiences into current assessment models
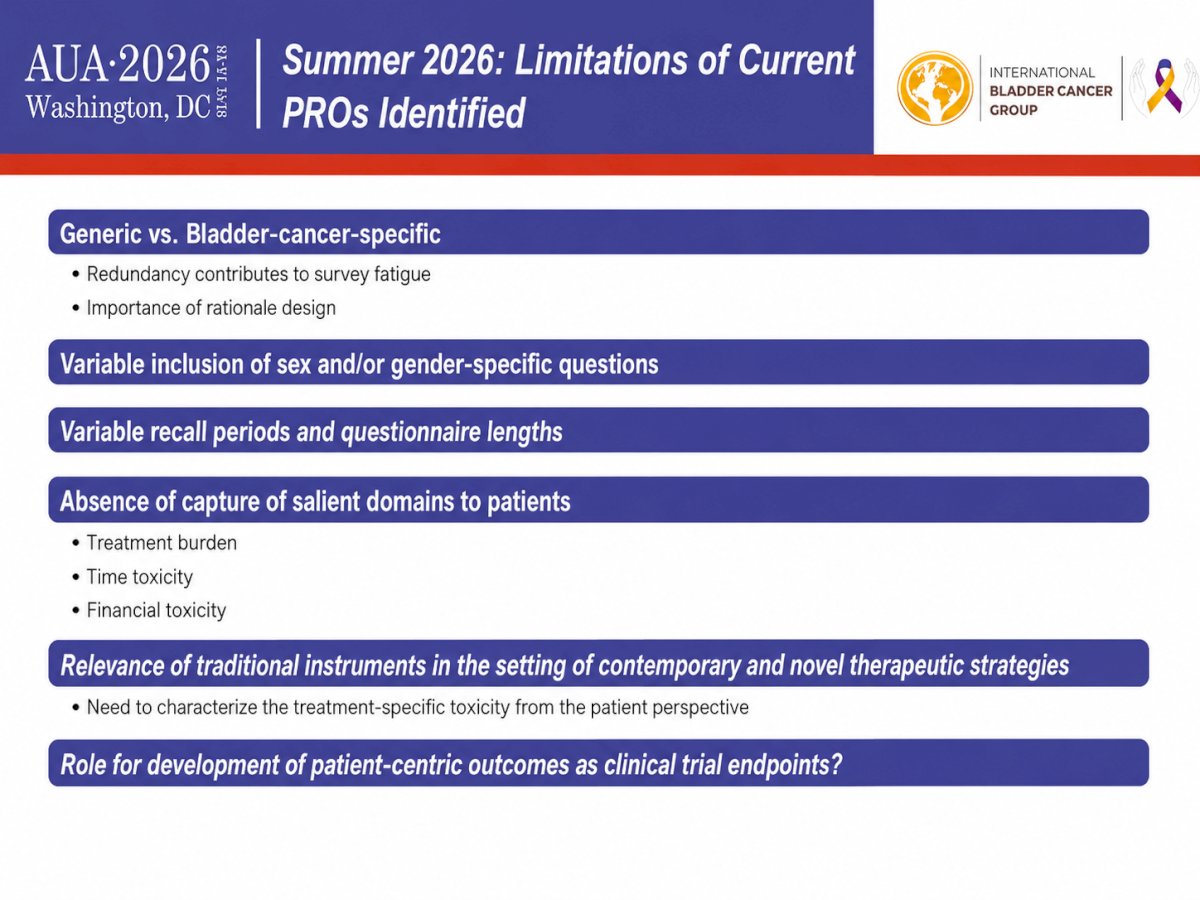
She further reviewed several important limitations of currently available PRO instruments identified during the IBCG discussions. These included:
- Redundancy between generic and bladder cancer–specific questionnaires, contributing to survey fatigue and emphasizing the need for more rational questionnaire design
- Variable inclusion of sex- and gender-specific questions across instruments
- Significant variability in recall periods and questionnaire length
- Failure to adequately capture patient-salient domains, including:
- Treatment burden
- Time toxicity
- Financial toxicity
- Limited relevance of traditional PRO instruments in the setting of contemporary and novel therapeutic strategies
- The need to better characterize treatment-specific toxicities from the patient perspective
- The evolving role of patient-centric outcomes as meaningful clinical trial endpoints
To address these gaps, the group developed a structured PRO taskforce work plan. This included:
- A systematic review of currently available PRO instruments and the domains they assess, along with a scoping review of PROs utilized in geriatrics and oncology
- Identification of the most relevant PRO tools specifically for patients with NMIBC
- Direct patient feedback regarding the relevance of individual questionnaire items to HR-QOL, as well as which domains patients felt should be prioritized in quality-of-life assessments
- Focus groups involving patients, patient advocates, and caregivers to identify additional missing domains and unmet needs
- Integration of these findings into the development of a dedicated IBCG-NMIBC PRO tool, followed by formal testing and validation efforts
Dr. Psutka and her team subsequently conducted a systematic review evaluating the use of PROMs in bladder cancer. The review included adults with NMIBC, MIBC, and metastatic bladder cancer across a broad range of prospective study designs, including randomized clinical trials, prospective non-randomized studies, single-arm trials, cohort studies, and PROM validation studies. Retrospective studies, case reports, case series, reviews, and editorials were excluded from the analysis.
Notably, the systematic review demonstrated substantial heterogeneity in the PROM instruments currently utilized across bladder cancer studies. The most frequently used tools included the EORTC QLQ-C30, FACT-Bl, and EORTC QLQ-BLM30. However, Dr. Psutka emphasized that many of these instruments were often being applied across disease states and treatment settings for which they were not originally designed or validated.
For example, several PROMs developed primarily for MIBC or advanced disease populations were also being utilized in NMIBC studies, despite important differences in treatment burden, symptom profiles, surveillance intensity, and patient priorities across these disease states. This highlighted a major limitation in the current PROM landscape and further supported the need for more disease-specific, treatment-relevant, and patient-centered assessment tools tailored to bladder cancer populations.
As next steps, Dr. Psutka highlighted that the group is currently conducting a scoping review focused on PROM domains that are not adequately captured in prospective bladder cancer research. This work is expanding beyond traditional symptom assessment to include emotional well-being, distress measures, and other patient-centered domains that may be highly relevant yet underrepresented in current instruments.
She emphasized that these efforts build upon prior observations suggesting that many commonly utilized PROMs fail to adequately assess the domains and questions most meaningful from the patient perspective. In this context, the IBCG partnered with Cristiane Bergerot and colleagues, who previously evaluated how patients with kidney cancer perceived the relevance of existing PRO instruments relative to their lived experiences.6,7 That work ultimately led to the development of a novel patient-centered questionnaire, the Kidney Symptom Index-19, serving as a potential model for future bladder cancer–specific PRO development initiatives.6 This work also supported further development of a health-related quality-of-life questionnaire for patients with metastatic or localized RCC, providing a useful framework for the IBCG effort to build a more relevant, bladder cancer–specific PRO tool.7
Dr. Patrick Hensley subsequently presented work performed on behalf of the IBCG team evaluating the incorporation of PROs into NMIBC clinical trials. He highlighted that PROs remain significantly underutilized in contemporary NMIBC research, with only approximately one in five trials incorporating PRO assessments as either primary or secondary endpoints. Importantly, he noted that this gap persists despite increasing emphasis from regulatory agencies and patient advocacy organizations on capturing the patient experience and incorporating patient-centered outcomes into clinical trial design. The findings were presented at ASCO GU, with the accompanying manuscript currently under review at BJUI. Dr Psutka highlighted that these data should serve as a call to action for greater harmonization and broader integration of PRO tools into NMIBC clinical trials moving forward.
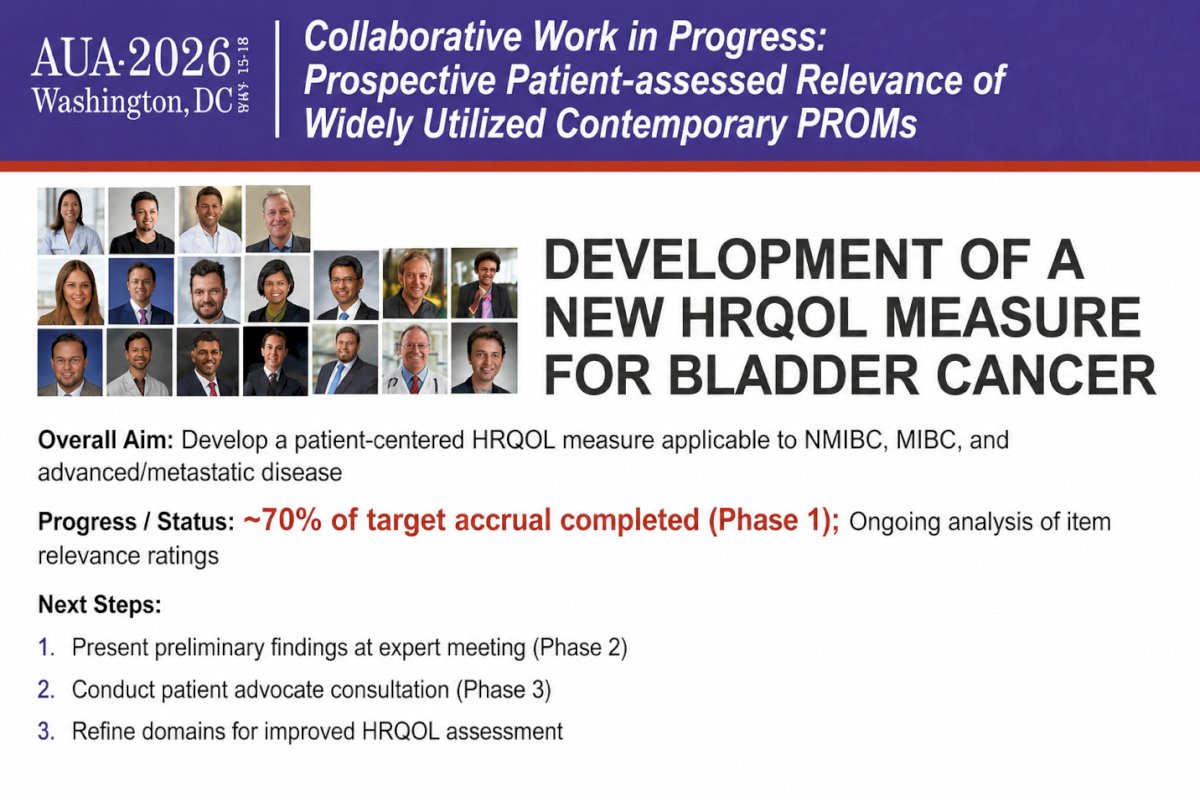
Moreover, the group is actively collaborating with international experts to develop a new patient-centered HRQOL measure for bladder cancer applicable across NMIBC, MIBC, and advanced/metastatic disease settings. Dr. Bergerot highlighted that approximately 70% of the target accrual for phase 1 has already been completed, with ongoing analyses evaluating the relevance of questionnaire items from the patient perspective. Planned next steps include presentation of preliminary findings at expert meetings, patient advocate consultations, and refinement of key HRQOL domains for improved assessment.
Additionally, the IBCG is collaborating with partners in Australia who developed the NMIBC-SI (Non–Muscle Invasive Bladder Cancer Symptom Index), further supporting international efforts to improve symptom assessment and patient-reported outcome measurement specifically for patients with NMIBC.8
Drs. Roger Li and Ashish Kamat's ongoing collaborative efforts are focusing on developing the IBCG bladder cancer toxicity assessment tool and disease-specific PRO modules for NMIBC, MIBC, and metastatic bladder cancer. The initiative is designed to provide a standardized framework to better adjudicate treatment-related toxicities and associate them with commonly used bladder cancer therapies across disease states. These PRO modules are being developed in parallel and aligned with the broader bladder toxicity tool project, with the goal of improving both clinical trial assessment and real-world evaluation of patient symptom burden, urinary function, bladder-related discomfort, infections, hematuria, and overall treatment impact from the patient perspective.
Lastly, Dr. Psutka emphasized that the overarching goal of these initiatives is the generation of a patient-centered PRO tool for use in both clinical trials and real-world practice that more accurately captures the lived experience of patients with bladder cancer. She highlighted several key PRO domains identified as critically important to patients, including financial toxicity, emotional symptoms, treatment-related toxicity from novel agents, gender-specific concerns, functional impairment and time toxicity, impact on family members and caregivers, treatment burden, social support, and overall treatment utility, including whether patients felt therapy was “worth it.”
She further noted that these efforts are being developed in collaboration with major patient advocacy organizations, including the Bladder Cancer Advocacy Network and the World Bladder Cancer Patient Coalition, ensuring that patient voices remain central to the development and refinement of future bladder cancer PRO instruments
Presented by:- Ashish Kamat, MD, MBBS, President, International Bladder Cancer Group (IBCG), Professor of Urology and Wayne B. Duddleston Professor of Cancer Research, MD Anderson Cancer Center, Houston, TX
- Sarah Psutka, MD, MS, FACS, Urologic Oncologist, Associate Professor of Urology, Department of Urology, Fred Hutchinson Cancer Research Center, University of Washington, Seattle, WA
Written by: Julian Chavarriaga, MD, Clinical Assistant Professor, Urologic Oncologist, Department of Urology at Penn State Health @chavarriagaj on Twitter during the American Urological Association (AUA) 2026 Annual Meeting, Washington, DC, Fri, May 15 – Mon, May 18, 2026.
References:
- Li R, Hensley PJ, Gupta S, Al-Ahmadie H, Babjuk M, Black PC, Brausi M, Bree KK, Fernández MI, Guo CC, Horowitz A, Lamm DL, Lerner SP, Lotan Y, Mariappan P, McConkey D, Mertens LS, Mir C, Ross JS, O'Donnell M, Palou J, Pohar K, Steinberg G, Soloway M, Spiess PE, Svatek RS, Tan WS, Taoka R, Buckley R, Kamat AM. Bladder-sparing Therapy for Bacillus Calmette-Guérin-unresponsive Non-muscle-invasive Bladder Cancer: International Bladder Cancer Group Recommendations for Optimal Sequencing and Patient Selection. Eur Urol. 2024 Dec;86(6):516-527. doi: 10.1016/j.eururo.2024.08.001. Epub 2024 Aug 24. PMID: 39183090.
- Gupta S, Hensley PJ, Li R, Choudhury A, Daneshmand S, Faltas BM, Flaig TW, Grass GD, Grivas P, Hansel DE, Hassanzadeh C, Kassouf W, Kukreja J, Mendoza-Valdés A, Moschini M, Mouw KW, Navai N, Necchi A, Rosenberg JE, Ross JS, Siefker-Radtke AO, Taylor J, Williams SB, Zlotta AR, Buckley R, Kamat AM. Bladder Preservation Strategies in Muscle-invasive Bladder Cancer: Recommendations from the International Bladder Cancer Group. Eur Urol. 2026 Jan;89(1):18-28. doi: 10.1016/j.eururo.2025.03.017. Epub 2025 Apr 22. PMID: 40268594.
- Li R, Hensley PJ, Babjuk M, Bukavina L, Psutka SP, Lerner SP, O'Donnell MA, Lotan Y, Bree KK, Redorta JP, McConkey DJ, Lee BH, Mariappan P, Mertens LS, Soloway MS, Svatek RS, Tan WS, Williams SB, Gupta S, Buckley R, Kamat AM. Intermediate-risk Non-muscle-invasive Bladder Cancer: Recommendations for Definitions, Risk Stratification, Management Strategies, and Clinical Trial Design from the International Bladder Cancer Group. Eur Urol Oncol. 2025 Dec;8(6):1685-1695. doi: 10.1016/j.euo.2025.08.003. Epub 2025 Oct 10. PMID: 41076366.
- Shilpa Gupta, Roger Li, Patrick J. Hensley, Siamak Daneshmand, Bishoy M. Faltas, Petros Grivas, Niyati Lobo, Maria Carmen Mir, Joshua J. Meeks, Kent W. Mouw, Marco Moschini, Andrea Necchi, Karima Oualla, Kamal S. Pohar, Jonathan E. Rosenberg, Bogdana Schmidt, Arlene O. Siefker-Radtke, Gary D. Steinberg, Arnulf Stenzl, Roger J. Buckley, Ashish M. Kamat, Optimal Management of Muscle-invasive Bladder Cancer: Recommendations from the International Bladder Cancer Group, European Urology, 2026. https://doi.org/10.1016/j.eururo.2026.01.029.
- Matthow Kirschenbaum, Hale Torgerson, Yurong Shao, Sarah Psutka. Patient-Reported Outcome Measures for Patients with Bladder Cancer: A Systematic Review. PROSPERO 2025 CRD420251159257. Available from https://www.cl.york. Ac.uk/PROSPERO/view/CR0420251159257
- Bergerot CD, Malhotra J, Bergerot P, Philip EJ, Castro DV, Hsu J, Mota ACA, Cardoso de Azeredo A, Neto JNM, Hutson T, Grünwald V, Bex A, Psutka SP, Rini B, Plimack ER, Master V, Albiges L, Choueiri TK, Pal S, Powles T. Patients' Perceptions Regarding the Relevance of Items Contained in the Functional Assessment of Cancer Therapy Kidney Symptom Index-19. Oncologist. 2023 Jun 2;28(6):494-500. doi: 10.1093/oncolo/oyad028. PMID: 36917626; PMCID: PMC10243758.
- Bergerot CD, Cella D, Bergerot PG, Castro DV, Mercier BD, Nally E, Ali AA, Philip EJ, Hutson T, Bex A, Psutka SP, Rini B, Plimack ER, Grünwald V, Master V, Albiges L, Choueiri TK, Pal SK, Powles T. Development of a Health-related Quality of Life Questionnaire for Patients with Metastatic or Localized Renal Cell Carcinoma. Eur Urol Oncol. 2025 Oct;8(5):1295-1302. doi: 10.1016/j.euo.2025.07.012. Epub 2025 Aug 19. PMID: 40829999.
- Rutherford C, Tait MA, Costa DSJ, King MT, Smith DP, Sengupta S, Ischia J, Mitterdorfer A, Hayne D, Watson R, Anderson P, Frydenberg M, Gilling P, Buchan N, Green E, Clarke N, Boorjian SA, Konety B, Holzbeierlein JM, Black PC, Chalasani V, Henseler J, Patel MI; NMIBC-SI Study Group. Development and psychometric evaluation of a patient-reported symptom index for patients with non-muscle invasive bladder cancer: the NMIBC-SI. J Patient Rep Outcomes. 2025 Mar 27;9(1):36. doi: 10.1186/s41687-025-00864-7. PMID: 40146452; PMCID: PMC11950540.