(UroToday.com) The American Urological Association's 2026 Annual Meeting, in Washington D.C., was host to the Clinical Trials in Progress: Bladder Cancer Session. Dr. TR Leyshon Griffiths presented the trial in progress: HIVEC®-HEAT (Hyperthermic intravesical mitomycin [Mitomycin medac]) for patients with BCG-unresponsive nonmuscle-invasive bladder cancer trial.
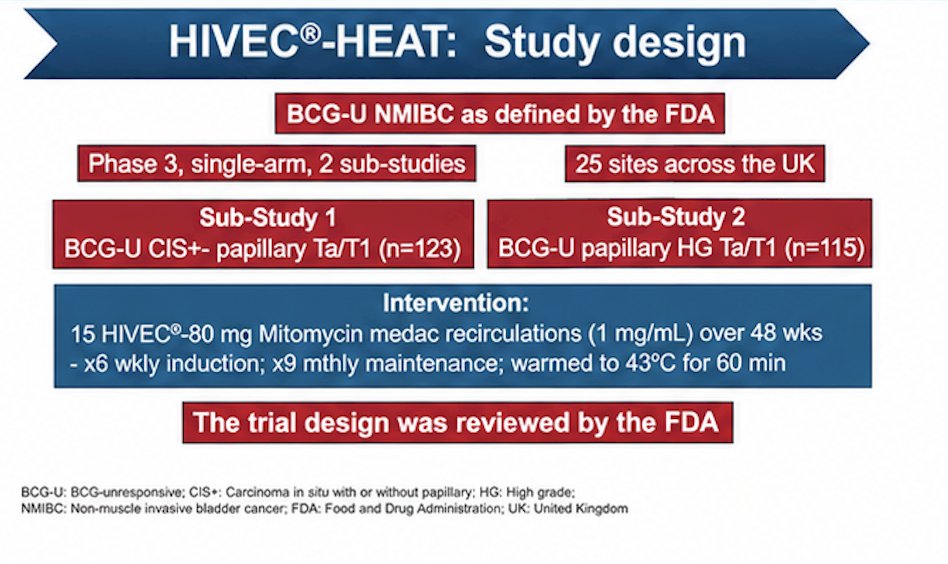
Dr. Griffiths highlighted the design of the HIVEC-HEAT trial in progress, a phase 3, single-arm study being conducted across 25 sites in the United Kingdom, evaluating chemohyperthermia in patients with BCG-unresponsive NMIBC as defined by FDA criteria. The study included two parallel sub-studies: Sub-study 1 enrolled patients with BCG-unresponsive CIS with or without papillary Ta/T1 disease (n=123), while Sub-study 2 enrolled patients with BCG-unresponsive high-grade papillary Ta/T1 disease without CIS (n=115).
Patients received intravesical HIVEC therapy consisting of 80 mg mitomycin C recirculated at a concentration of 1 mg/mL over a 48-week treatment period. Treatment included a 6-week induction phase followed by 9 monthly maintenance instillations. The mitomycin solution was heated to 43°C and administered over 60 minutes. Dr. Griffiths noted that the trial design was reviewed in collaboration with the FDA, and the study design is shown below:
Dr. Griffiths also reviewed the rationale supporting the HIVEC approach with mitomycin C. He noted that the intended standardized concentration for treatment was 1 mg/mL, a dose supported by preclinical and clinical experience evaluating intravesical chemotherapy combined with hyperthermia. Preclinical studies demonstrated that mitomycin penetration with HIVEC appeared to saturate at the 80 mg dose level, supporting the dosing strategy selected for the trial. In addition, prior long-term clinical experience with hyperthermic mitomycin C in NMIBC from Spanish cohorts demonstrated improvements in recurrence-free survival, including a reported 22% improvement in RFS at 24 months (p=0.0007).1
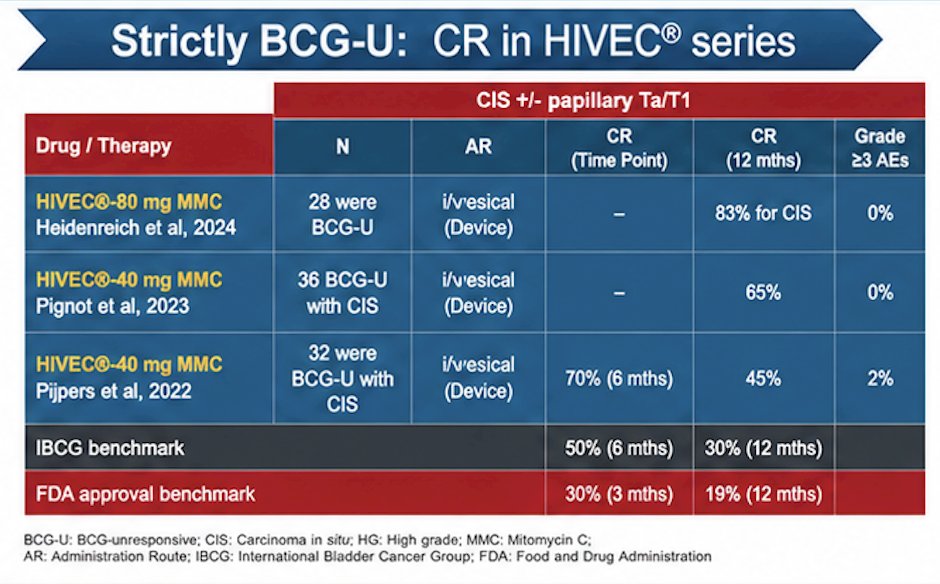
He also reviewed historical outcomes with HIVEC in strictly BCG-unresponsive NMIBC populations. In particular, he highlighted data from the Cologne experience reported by Heidenreich et al. (2024), in which patients treated with HIVEC using 80 mg mitomycin C demonstrated encouraging efficacy, including a 12-month complete response rate of 83% among patients with CIS, with no reported grade ≥3 adverse events.2
Additional series using 40 mg mitomycin C also demonstrated promising activity, with 12-month complete response rates ranging from 45% to 65% and favorable tolerability profiles. These outcomes compared favorably against historical IBCG and FDA approval benchmarks for BCG-unresponsive disease, which generally target complete response rates of approximately 50% at 6 months and 30% at 12 months for the IBCG benchmark, and 30% at 3 months with 19% at 12 months for FDA approval thresholds.
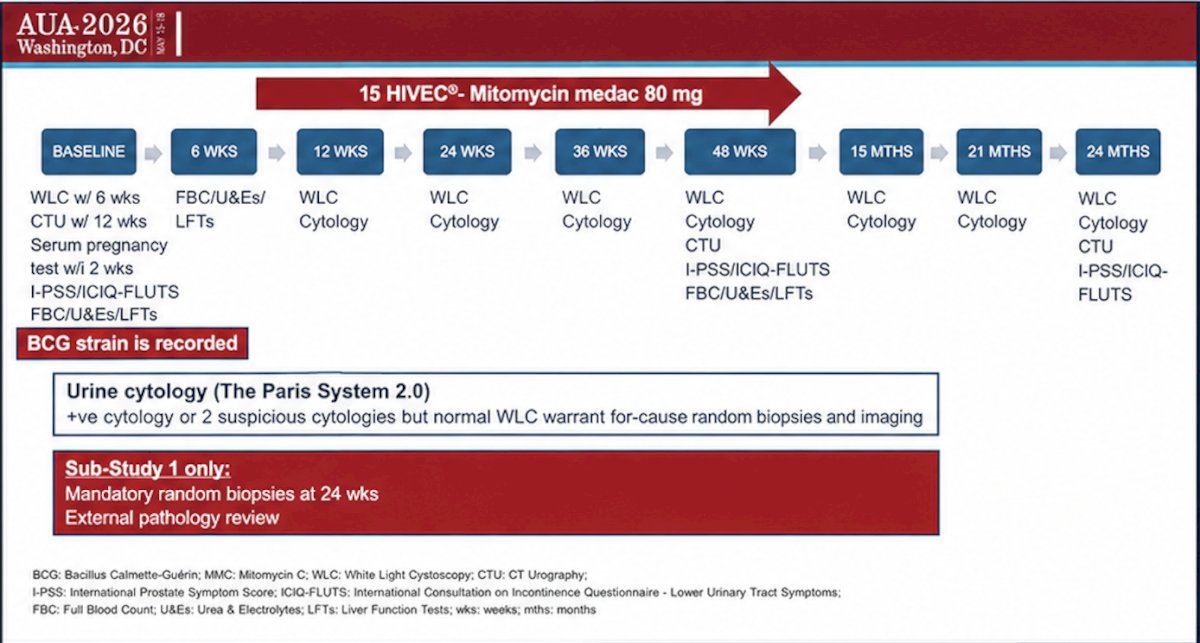
The study schema included a total of 15 HIVEC instillations using 80 mg mitomycin C medac administered over 48 weeks, consisting of a 6-week induction phase followed by monthly maintenance treatments. Patients underwent serial surveillance with white light cystoscopy and urine cytology at predefined intervals throughout follow-up, with additional CT urography, symptom assessments using I-PSS and ICIQ-FLUTS questionnaires, and laboratory evaluations including hematologic and liver function testing. The BCG strain previously received by patients was also recorded. Importantly, positive urine cytology based on Paris System 2.0 criteria, or two suspicious cytologies despite normal cystoscopy, triggered for-cause random biopsies and imaging. In Sub-Study 1, mandatory random biopsies at 24 weeks and external pathology review were incorporated into the protocol.
Inclusion criteria for the study are:
- BCG-unresponsive NMIBC detected on white light cystoscopy
- CIS with or without completely resected high-grade Ta/T1 disease
- Completely resected BCG-unresponsive high-grade Ta/T1 tumors
Key exclusion criteria:
- Disease detected only with enhanced cystoscopy
- Mitomycin C allergy
- Prior salvage therapy for BCG-unresponsive disease
- Upper tract or urethral urothelial carcinoma within 2 years
- Prior pelvic radiotherapy
- Enrollment in another interventional clinical trial
- ECOG performance status 3–4
- Lymphovascular invasion
- Variant histology
The primary endpoints differed between the two sub-studies. In Sub-Study 1, the primary endpoint was complete response at 3 months, defined as a normal cystoscopy without evidence of recurrent CIS in the bladder and a urine cytology result that was not positive. In Sub-Study 2, the primary endpoint was median duration of high-grade recurrence-free survival.
Secondary endpoints for Sub-Study 1 included median duration of complete response, as well as complete response rates at 6, 12, and 24 months. Across both sub-studies, secondary endpoints included adverse events, freedom from recurrent high-grade Ta/T1 or CIS at 6, 12, and 24 months, freedom from non-bladder recurrence of urothelial carcinoma, progression-free survival, cystectomy-free survival, disease-specific survival, and overall survival.
Dr. Griffiths also provided an update on the ongoing trial status. He noted that the first participant was recruited at the end of January, with 5 patients enrolled thus far and an additional 8 under consideration. At the time of presentation, 9 sites were actively open, with a target of 25 participating sites overall, while 27 sites had already expressed interest in participation. He further noted that the first interim analysis for Sub-Study 1 is anticipated in early 2027.
Presented by: TR Leyshon Griffiths, BSc MBBS MD FRCS Ed (Urol) SFHEA Associate Professor/Consultant Urological Surgeon at University of Leicester, United Kingdom
Written by: Julian Chavarriaga, MD, Clinical Assistant Professor, Urologic Oncologist, Department of Urology at Penn State Health @chavarriagaj on Twitter during the American Urological Association (AUA) 2026 Annual Meeting, Washington, DC, Fri, May 15 – Mon, May 18, 2026.
Reference:
- Plata A, Guerrero-Ramos F, Garcia C, González-Díaz A, Gonzalez-Valcárcel I, de la Morena JM, Díaz-Goizueta FJ, Del Álamo JF, Gonzalo V, Montero J, Sousa-Escandón A, León J, Pontones JL, Delgado F, Adriazola M, Pascual Á, Calleja J, Ruano A, Martínez-Piñeiro L, Angulo JC. Long-Term Experience with Hyperthermic Chemotherapy (HIVEC) Using Mitomycin-C in Patients with Non-Muscle Invasive Bladder Cancer in Spain. J Clin Med. 2021 Oct 30;10(21):5105. doi: 10.3390/jcm10215105. PMID: 34768625; PMCID: PMC8584886.
- Kastner L, Rieger C, Pfister D, Schmautz M, Storz E, Heidenreich A. HIVEC as an alternative option in non-muscle-invasive bladder cancer: Experiences from a high-volume center. Urol Oncol. 2024 Aug;42(8):245.e19-245.e26. doi: 10.1016/j.urolonc.2024.01.300. Epub 2024 Apr 22. PMID: 38653592.