(UroToday.com) The American Urological Association's 2026 Annual Meeting, in Washington D.C., was host to the Clinical Trials in Progress: Bladder Cancer Session. Dr. Max Kates presented the trial in progress: REL-NDV01-301 (BOOST) - A Phase 3, Randomized Study of Adjuvant Intravesical Sustained-Release Gemcitabine-Docetaxel (NDV-01) Versus Surveillance for the Treatment of Intermediate-Risk Non-Muscle Invasive Bladder Cancer.
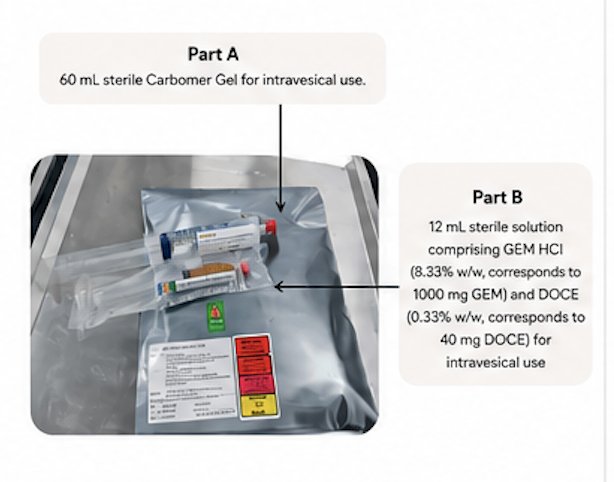
Dr. Kates began by highlighting NDV-01, a novel intravesical formulation combining a carbomer gel matrix with gemcitabine, docetaxel, and DMSO. He explained that the platform is designed to provide prolonged intravesical drug exposure, as the gel dissolves in urine and is washed out within 24 hours while the matrix gradually degrades, allowing continuous exposure to chemotherapy over approximately 10 days.
The formulation includes a 60 mL sterile carbomer gel component and a second solution containing gemcitabine 1000 mg and docetaxel 40 mg for intravesical administration (as illustrated below). Dr. Kates further noted that preparation does not require a specialized chemotherapy hood and that the drug can be instilled over approximately 5 minutes, potentially simplifying administration in clinical practice.
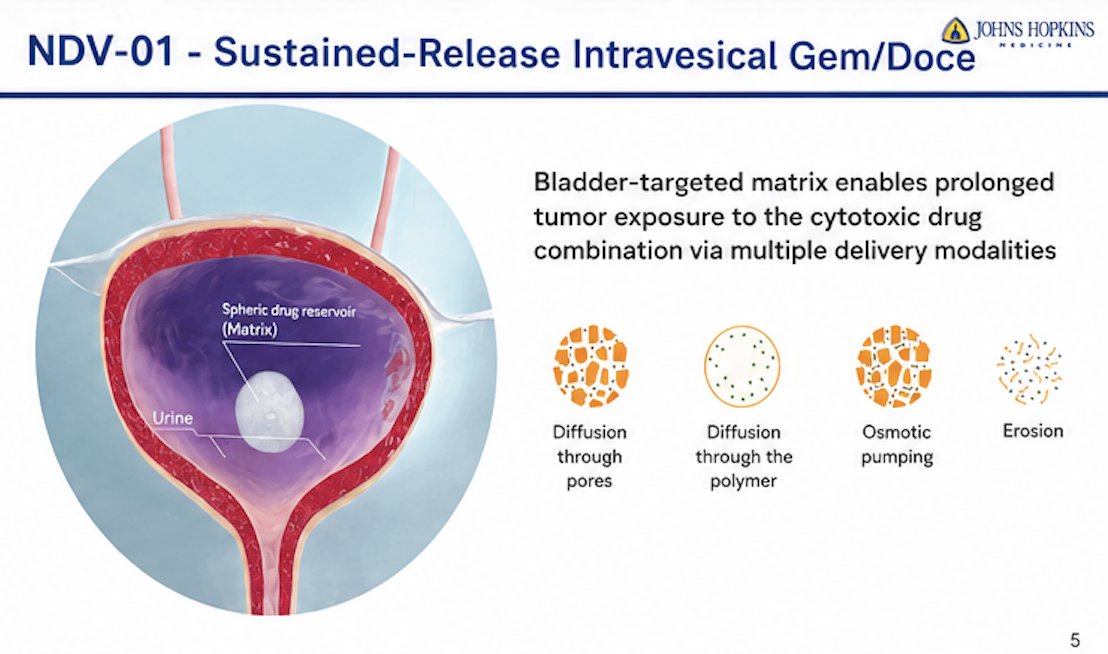
He further explained that NDV-01 is designed as a sustained-release intravesical gemcitabine/docetaxel platform in which a bladder-targeted matrix enables prolonged exposure of tumor tissue to cytotoxic therapy. The spherical drug reservoir gradually releases chemotherapy through multiple delivery mechanisms, including diffusion through pores, diffusion through the polymer matrix, osmotic pumping, and matrix erosion. This sustained-release approach is intended to maximize local drug exposure within the bladder while potentially improving therapeutic durability compared with standard intravesical instillation approaches.
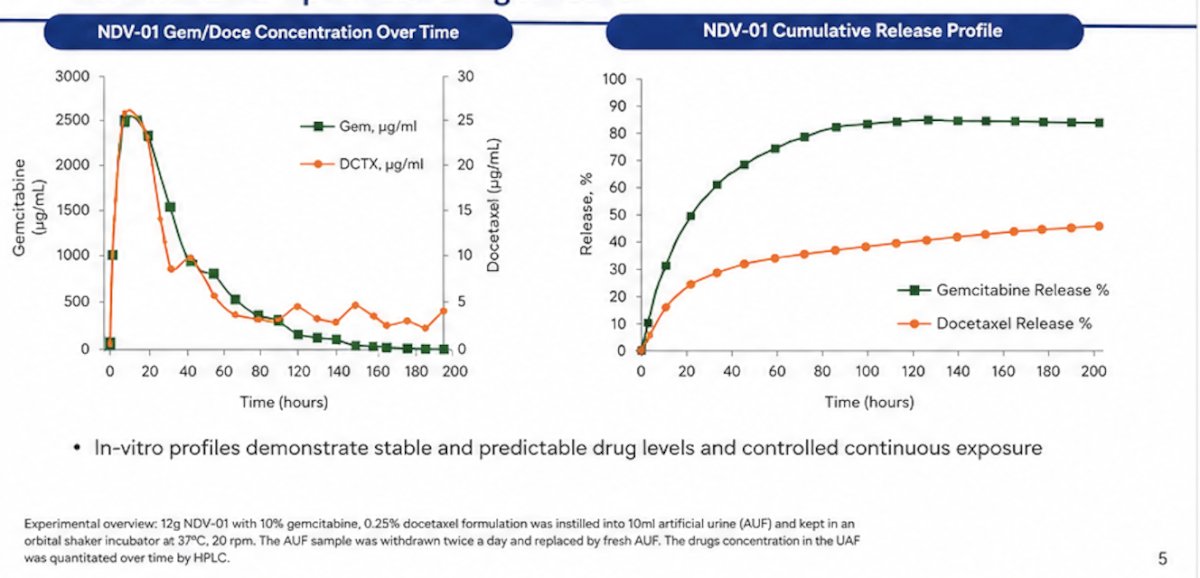
Preclinical in-vitro analyses demonstrated that NDV-01 provides stable and controlled release of both gemcitabine and docetaxel over time. Drug concentration curves showed sustained exposure across approximately 200 hours, while cumulative release profiles demonstrated predictable continuous delivery kinetics for both agents. Gemcitabine release approached approximately 80% over time, whereas docetaxel exhibited a slower and more gradual release profile.
Dr. Kates highlighted that recurrence remains a major clinical challenge in intermediate-risk NMIBC, even after TURBT and standard intravesical therapy. There is a steady decline in recurrence-free survival over time following TURBT, underscoring the persistent burden of recurrence and the ongoing need for more durable bladder-preserving treatment strategies in this patient population.1 The 2025 NCCN Guidelines for NMIBC emphasize that intravesical therapy remains the preferred management strategy for patients with intermediate-risk disease following TURBT. He noted that despite current guideline-directed approaches, recurrence rates remain substantial, highlighting the unmet need for therapies capable of improving the durability of response while preserving the bladder.
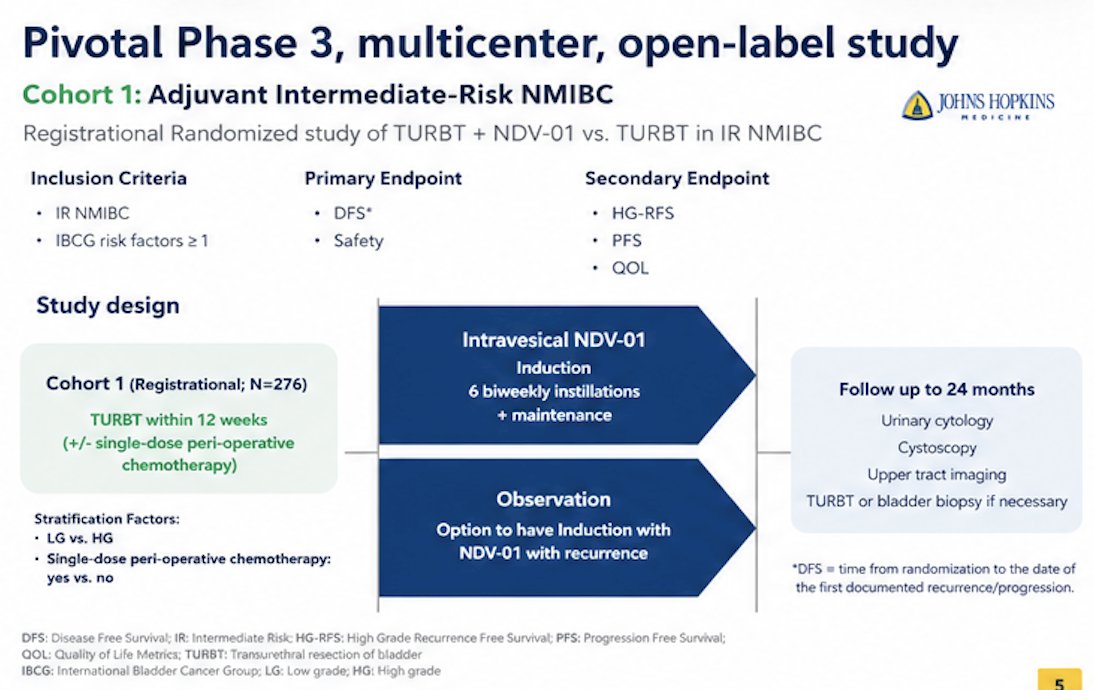
To address this, Dr. Kates presented the design of a pivotal phase 3, multicenter, open-label registrational trial evaluating adjuvant NDV-01 in intermediate-risk NMIBC. Cohort 1 plans to enroll 276 patients with IR NMIBC and at least one IBCG risk factor who have undergone TURBT within 12 weeks, with or without single-dose perioperative chemotherapy. Patients are randomized to intravesical NDV-01 versus observation. The NDV-01 arm includes an induction phase consisting of 6 biweekly instillations followed by maintenance therapy, whereas patients in the observation arm may receive induction NDV-01 at the time of recurrence.
The primary endpoints are disease-free survival and safety, while secondary endpoints include high-grade recurrence-free survival, progression-free survival, and quality-of-life outcomes. Stratification factors include low-grade versus high-grade disease and prior use of single-dose perioperative chemotherapy. Patients will undergo follow-up for up to 24 months with urinary cytology, cystoscopy, upper tract imaging, and TURBT or bladder biopsy as clinically indicated. The study schema is shown below:
Crossover to NDV-01 is permitted for patients in the observation arm at the time of recurrence. Dr. Kates also noted the anticipated study timelines, with estimated last patient in expected in late 2027.

For this study, the power calculation assumed a 25% recurrence rate in the NDV-01 arm compared with a 40% recurrence rate in the control arm at 2 years. The trial was designed with 90% statistical power using a one-sided alpha of 0.025 to detect a significant difference between treatment groups. The study also incorporates an event-driven analysis design, with the primary analysis planned once approximately 128 disease-free survival events have occurred among the 276 randomized participants.
Presented by: Max Kates, MD, Division Director, Bladder Cancer Program, Urologic Oncology, Brady Urological Institute; Associate Professor of Urology, Johns Hopkins Medicine, Baltimore, MD
Written by: Julian Chavarriaga, MD, Clinical Assistant Professor, Urologic Oncologist, Department of Urology at Penn State Health @chavarriagaj on Twitter during the American Urological Association (AUA) 2026 Annual Meeting, Washington, DC, Fri, May 15 – Mon, May 18, 2026.
Reference: