(UroToday.com) The American Urological Association's 2026 Annual Meeting, in Washington D.C., was host to the Clinical Trials in Progress: Bladder Cancer Session. Dr. David Cahn presented Safety and Efficacy of Bel-sar (AU-011), a Virus-Like Drug Conjugate, in Participants with Non-Muscle Invasive Bladder Cancer (NMIBC).
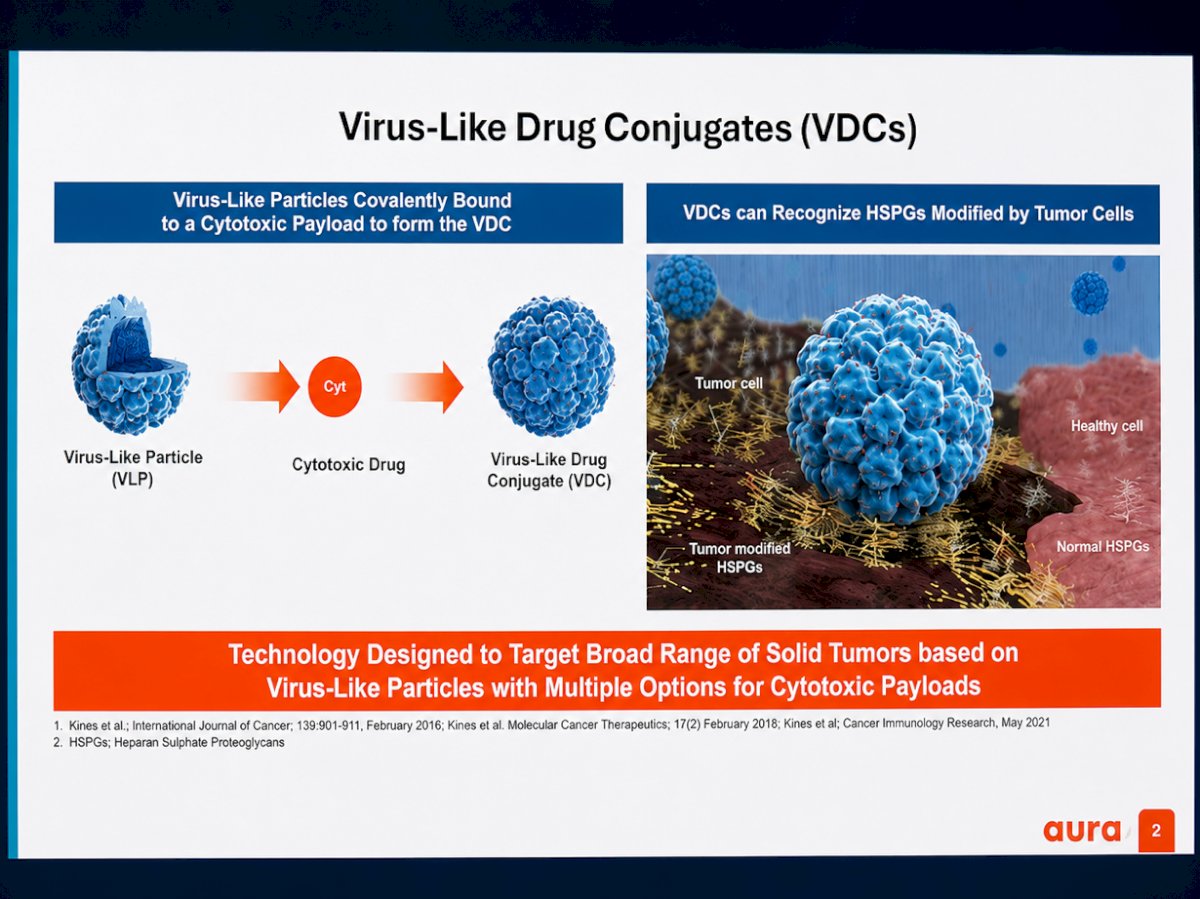
Dr. Cahn began by highlighting the development of virus-like drug conjugates (VDCs), a novel therapeutic platform designed to selectively deliver cytotoxic payloads to tumor cells. He explained that these constructs consist of virus-like particles covalently bound to cytotoxic agents, creating a targeted delivery system capable of recognizing tumor-associated heparan sulfate proteoglycans (HSPGs), which are modified on the surface of malignant cells. He further noted that this technology is intended to target a broad range of solid tumors while potentially minimizing effects on healthy tissues, leveraging the biologic properties of virus-like particles to improve tumor-specific drug delivery.
Dr. Cahn further described the proposed mechanism of action of bel-sar (AU-011), noting that virus-like drug conjugates bind to tumor-associated HSPGs on malignant cells and are subsequently activated by 689 nm light exposure. This activation generates reactive oxygen species that disrupt tumor cell membranes and organelles, resulting in rapid tumor cell necrosis.
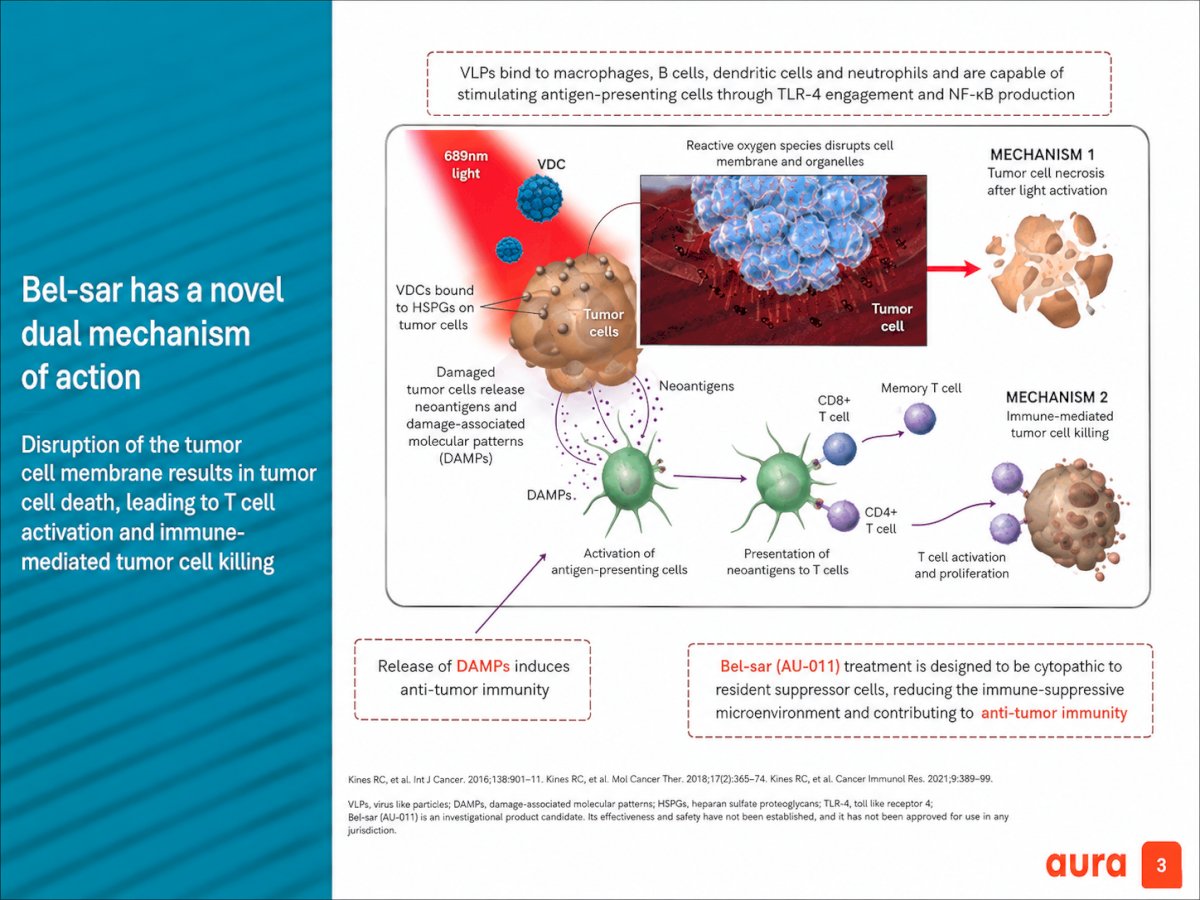
He emphasized that, beyond direct cytotoxicity, treatment may also promote an anti-tumor immune response. Damaged tumor cells release neoantigens and damage-associated molecular patterns (DAMPs), leading to activation of antigen-presenting cells and downstream CD4+ and CD8+ T-cell activation. Bel-sar was designed not only to induce tumor cell killing, but also to reduce the local immune-suppressive tumor microenvironment and enhance anti-tumor immunity.
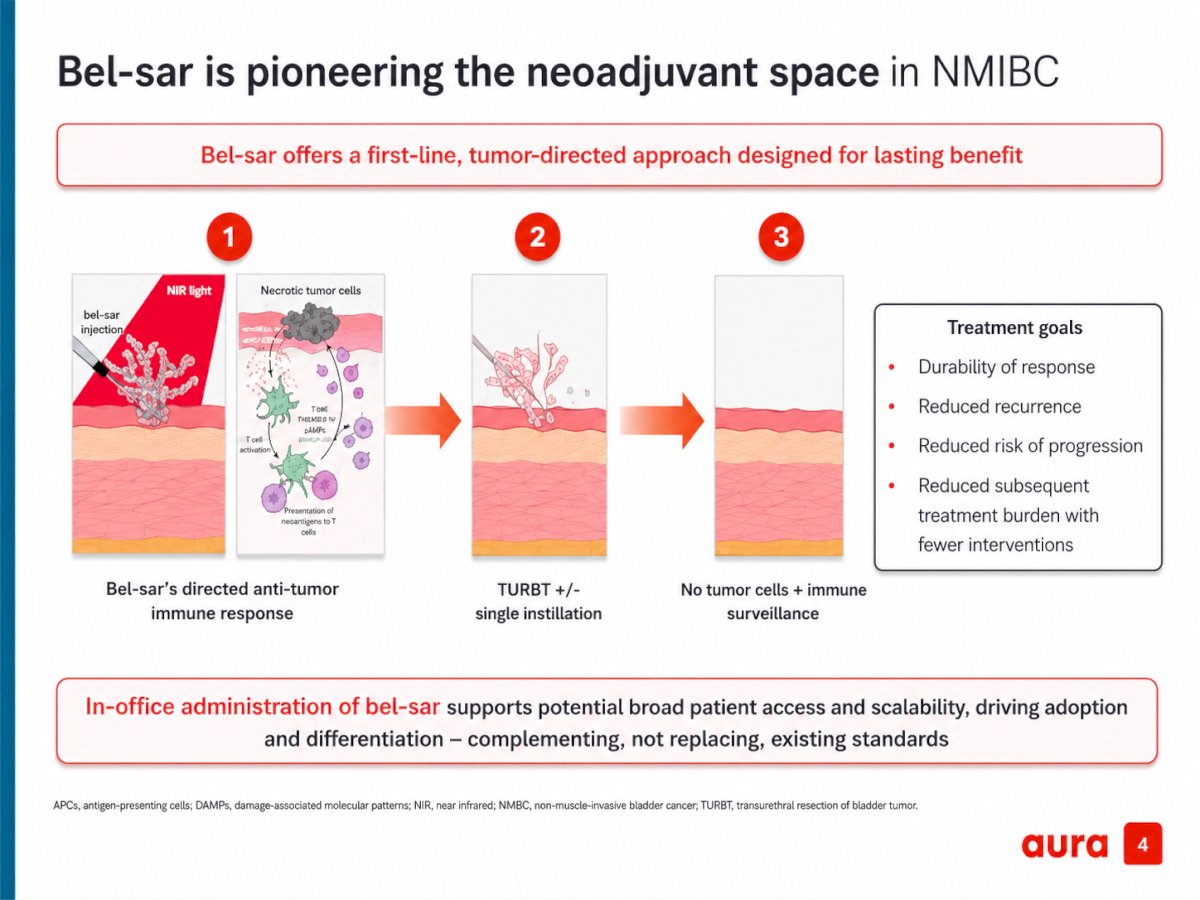
Bel-sar is a novel tumor-directed therapy being explored in the neoadjuvant setting for NMIBC. The proposed treatment strategy involves intratumoral administration of bel-sar followed by near-infrared light activation, leading to tumor cell necrosis and stimulation of a localized anti-tumor immune response prior to TURBT with or without single-dose intravesical therapy. The approach is intended to reduce residual disease burden and potentially improve long-term oncologic control while decreasing recurrence, progression risk, and the need for repeated interventions. He also emphasized the feasibility of in-office administration, positioning bel-sar as a scalable adjunctive strategy designed to complement, rather than replace, existing standards of care.
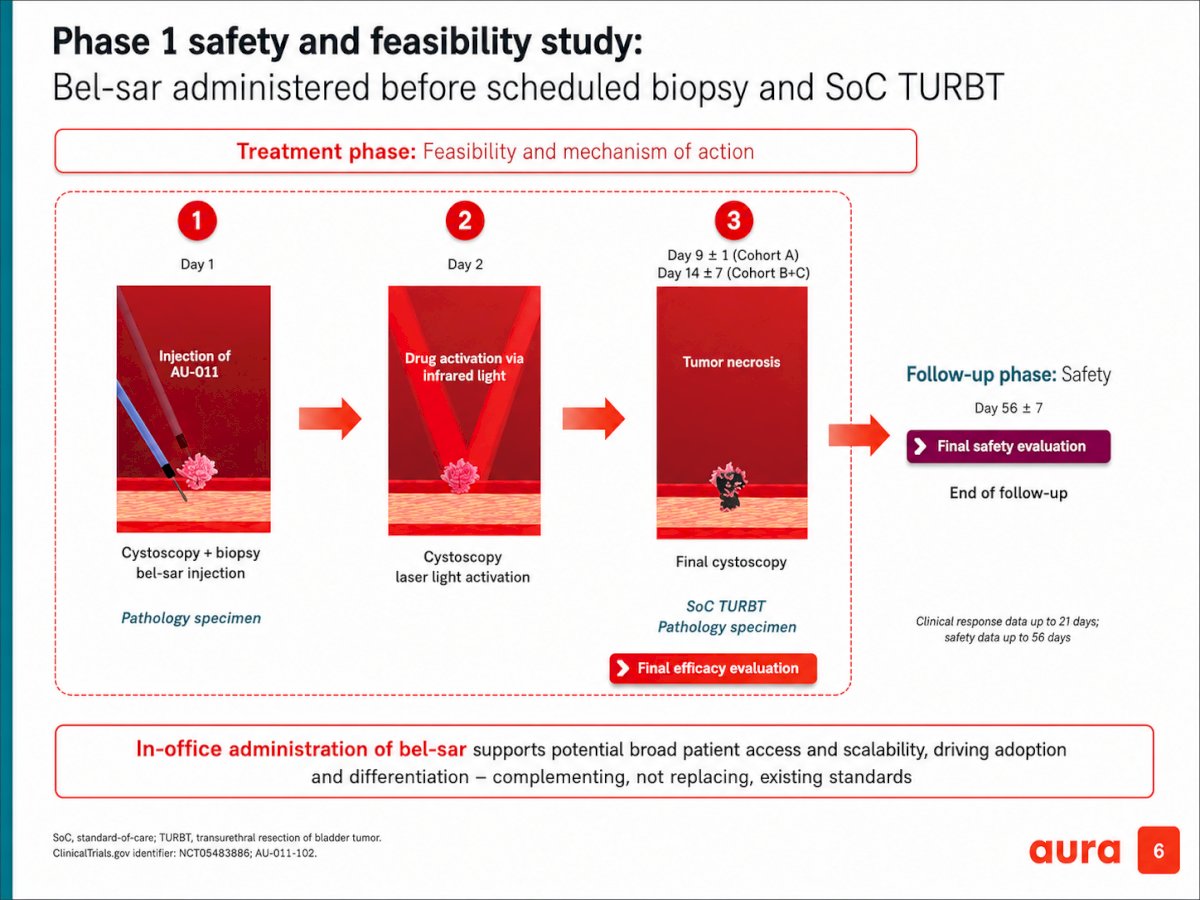
The phase 1 safety and feasibility study evaluated bel-sar administered prior to scheduled biopsy and standard-of-care TURBT. On day 1, patients underwent cystoscopy with biopsy and intratumoral injection of bel-sar (AU-011), followed on day 2 by cystoscopic near-infrared light activation. Final cystoscopic assessment and TURBT were subsequently performed on day 9 ±1 for cohort A and day 14 ±7 for cohorts B and C to evaluate tumor necrosis and obtain pathology specimens for efficacy assessment. The study also incorporated a dedicated safety follow-up phase, with final safety evaluation performed at day 56 ±7. Clinical response data were collected for up to 21 days, while safety outcomes were monitored through 56 days following treatment.
Dr. Cahn noted that a single dose of bel-sar produced encouraging clinical complete responses in both intermediate- and high-risk NMIBC cohorts. Among intermediate-risk patients (n=5), 4 of 5 treated tumors achieved clinical complete response (cCR), while the remaining treated tumor demonstrated visible shrinkage. Additionally, 3 of 5 patients achieved cCR in at least one untreated tumor, suggesting a potential broader immune-mediated effect.In the high-risk cohort (n=5), 3 of 5 treated tumors demonstrated visible tumor shrinkage, and 1 patient achieved cCR in both treated and untreated tumors. Visual cystoscopic changes were observed in 4 of 5 patients in both cohorts, and all treated and untreated tumors demonstrated evidence of immune response.
From a safety standpoint, the treatment demonstrated a favorable profile among 17 evaluable patients. Fewer than 10% experienced grade 1 treatment-emergent adverse events related to study drug, with no grade 2 or 3 treatment-related adverse events, serious adverse events, or dose-limiting toxicities reported.
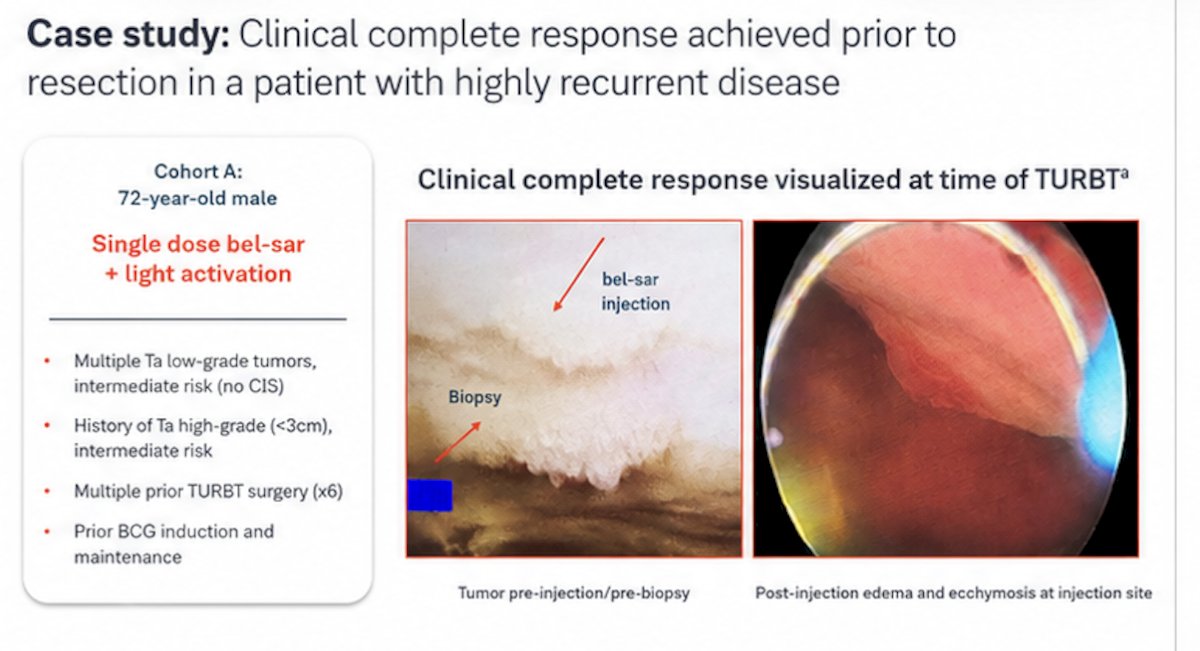
Dr. Cahn presented a representative case from cohort A involving a 72-year-old male with highly recurrent intermediate-risk NMIBC who received a single dose of bel-sar followed by light activation. The patient had multiple Ta low-grade tumors without CIS, a prior history of Ta high-grade disease (<3 cm), six prior TURBT procedures, and previous BCG induction plus maintenance therapy. Cystoscopic images demonstrated the tumor prior to injection and biopsy, followed by post-treatment edema and ecchymosis at the injection site. At the time of TURBT, a clinical complete response was visualized, supporting the localized anti-tumor activity observed with bel-sar treatment.
Multiplex immunofluorescence analyses further suggested that bel-sar may induce adaptive immune memory through the generation of mature tertiary lymphoid structures (TLS). Pre- and post-treatment tissue samples from both target and non-target lesions demonstrated increased immune cell organization following treatment, including CD3+, CD20+, CD23+, PanCK+, and PNAd+ immune infiltrates associated with TLS formation.
Among 5 evaluable participants, mature TLS was identified within target lesions in all patients, including de novo TLS formation in 3 cases, which was associated with clinical complete responses. Additionally, mature TLS was also observed in non-target lesions in 2 of 5 participants, supporting the possibility of a broader urothelial field effect and systemic anti-tumor immune activation beyond the directly treated lesion.
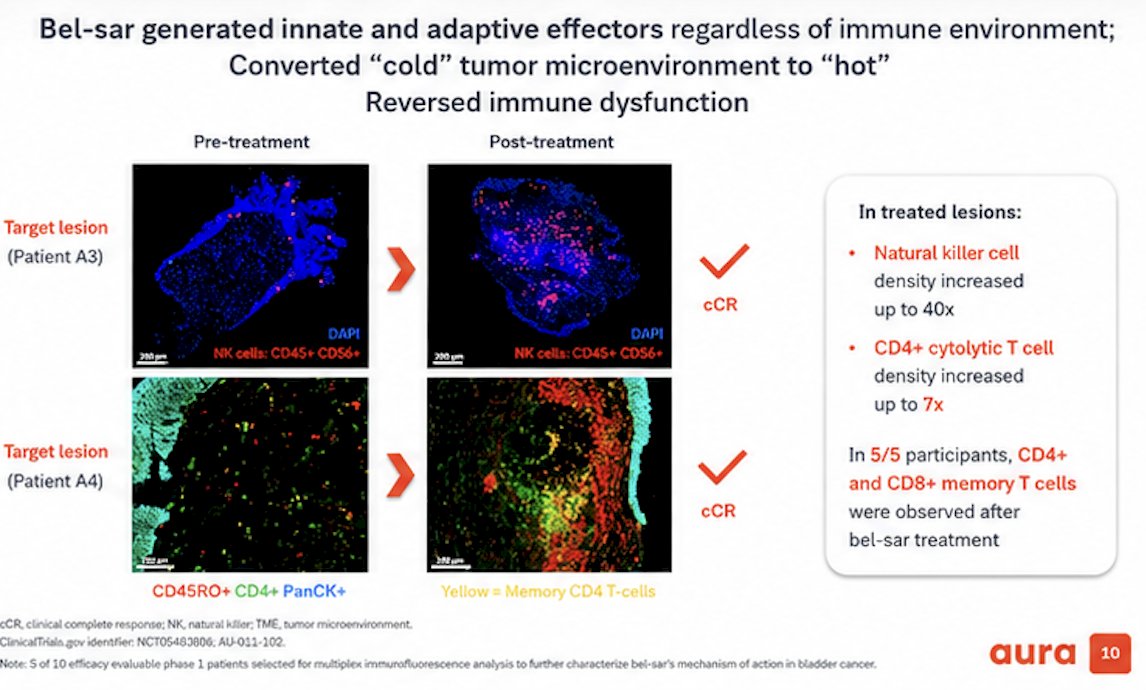
Moreover, additional translational analyses demonstrated that bel-sar generated both innate and adaptive immune effectors regardless of the baseline immune microenvironment, effectively converting immunologically “cold” tumors into “hot” tumors while reversing immune dysfunction. Post-treatment tissue analyses showed marked increases in immune infiltration within treated lesions, including up to a 40-fold increase in natural killer (NK) cell density and up to a 7-fold increase in CD4+ cytolytic T-cell density.
The presentation also highlighted the emergence of immune memory signatures following treatment. In 5 of 5 evaluable participants, both CD4+ and CD8+ memory T cells were identified after bel-sar administration, further supporting the potential for durable immune-mediated anti-tumor activity associated with treatment.
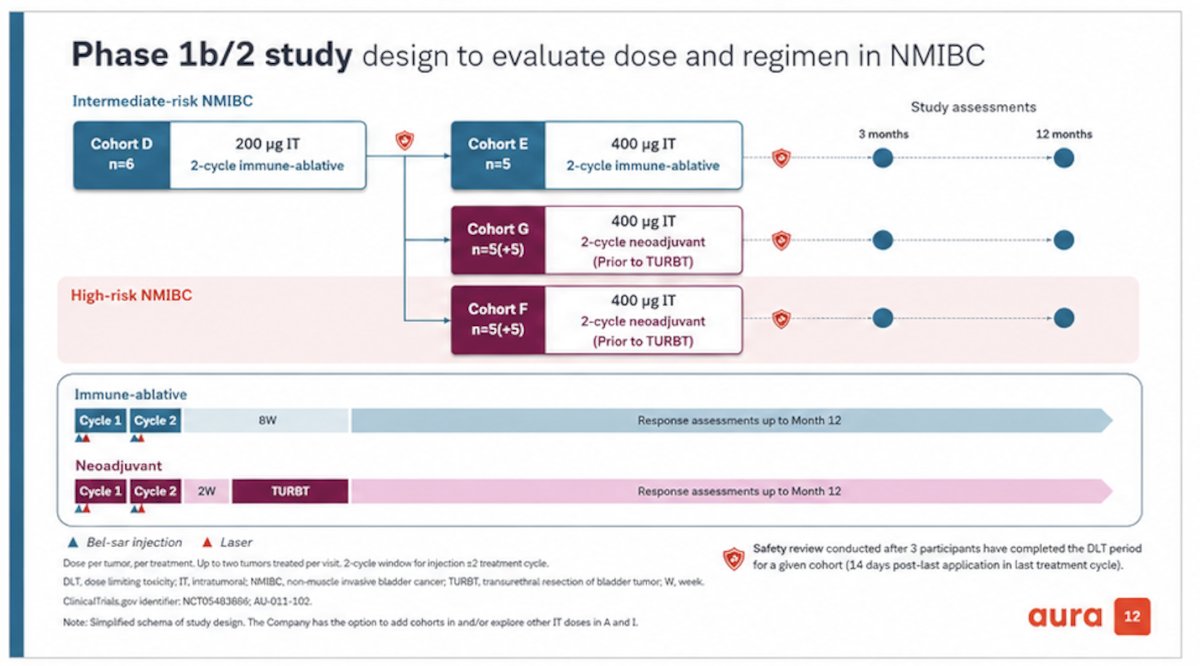
Lastly, Dr. Cahn presented the ongoing phase 1b/2 study evaluating bel-sar dose escalation and treatment regimens in NMIBC. The trial includes intermediate-risk and high-risk NMIBC cohorts exploring both immune-ablative and neoadjuvant strategies. Intermediate-risk cohorts include cohort D evaluating 200 μg intratumoral bel-sar with a two-cycle immune-ablative approach and cohort E evaluating a 400 μg regimen. Additional neoadjuvant cohorts include cohort G for intermediate-risk disease and cohort F for high-risk disease, both utilizing two treatment cycles prior to TURBT.
The immune-ablative strategy consists of two treatment cycles followed by longitudinal response assessments through 12 months, while the neoadjuvant approach administers two cycles prior to TURBT with subsequent follow-up assessments extending to 12 months. Safety reviews are performed after completion of dose-limiting toxicity evaluation periods within each cohort. The study design is presented below:
Dr. Cahn concluded his presentation with the following key takeaway points:
- In both intermediate- and high-risk NMIBC, local administration of a single low dose of bel-sar induced clinical complete responses through rapid tumor necrosis, immune cell infiltration, localized immune memory, and a potential urothelial field effect.
- Only grade 1 drug-related adverse events were observed, supporting a favorable early safety profile.
- Translational analyses demonstrated generation of adaptive immune memory through de novo mature tertiary lymphoid structures in 3 of 5 evaluable participants.
- Bel-sar generated both innate and adaptive anti-tumor immune responses, converting immunologically “cold” tumors into “hot” tumors and reversing immune dysfunction.
- Ongoing phase 1b/2 studies are evaluating the longitudinal safety and efficacy of escalating bel-sar doses and multiple treatment cycles in patients with NMIBC.
Presented by: David Cahn, MD, Colorado Clinical Research, Colorado Urology, Lakewood, CO
Written by: Julian Chavarriaga, MD, Clinical Assistant Professor, Urologic Oncologist, Department of Urology at Penn State Health @chavarriagaj on Twitter during the American Urological Association (AUA) 2026 Annual Meeting, Washington, DC, Fri, May 15 – Mon, May 18, 2026.