(UroToday.com) The American Urological Association's 2026 Annual Meeting, between May 15 – May 18, 2026 in Washington D.C., was host to the Clinical Trials in Progress: Bladder Cancer Session. Dr. Christopher Pieczonka presented the trial in progress: MoonRISe-2, a Phase 2 Dose Expansion Within the Study of Erdafitinib Intravesical Drug Releasing System (TAR-210) for Localized Bladder Cancer: Study Design and Baseline Characteristics.
Dr. Pieczonka highlighted that there remains a significant unmet need in recurrent intermediate-risk NMIBC. He noted that while TURBT followed by adjuvant intravesical therapy remains the current standard of care, many patients continue to experience frequent recurrences and repeated procedures that contribute to cumulative morbidity and diminished quality of life.
He emphasized that recurrent TURBT is associated with procedural risks, including bleeding, infection, perforation, LUTS, and UTIs, in addition to the burden of repeated anesthesia exposure. Despite current treatment approaches, recurrence rates remain high, exceeding 60% at 5 years in some patients, with progression rates reaching up to 17%, particularly among those harboring additional IBCG risk factors. As a result, there remains a substantial need for more durable, patient-friendly therapeutic strategies in intermediate-risk NMIBC.
Dr. Pieczonka noted that FGFR alterations are present in a substantial proportion of intermediate-risk NMIBC tumors, occurring in approximately 70% of cases, and may serve as important oncogenic drivers in this disease setting. He emphasized that this biology provides a strong rationale for targeted therapeutic approaches in recurrent IR NMIBC.
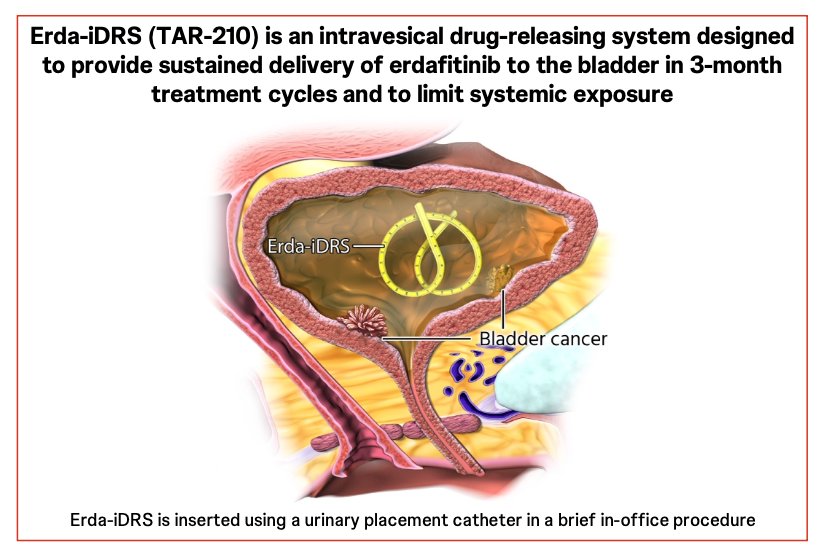
He further explained that erdafitinib, an oral selective pan-FGFR inhibitor currently approved for FGFR3-altered metastatic urothelial carcinoma, has demonstrated encouraging activity in earlier-stage disease when delivered locally through the Erda-iDRS platform. In a first-in-human ablative study of patients with FGFR-altered IR NMIBC, Erda-iDRS was well tolerated and achieved a high complete response rate of 89%, with a median duration of response of 18 months.
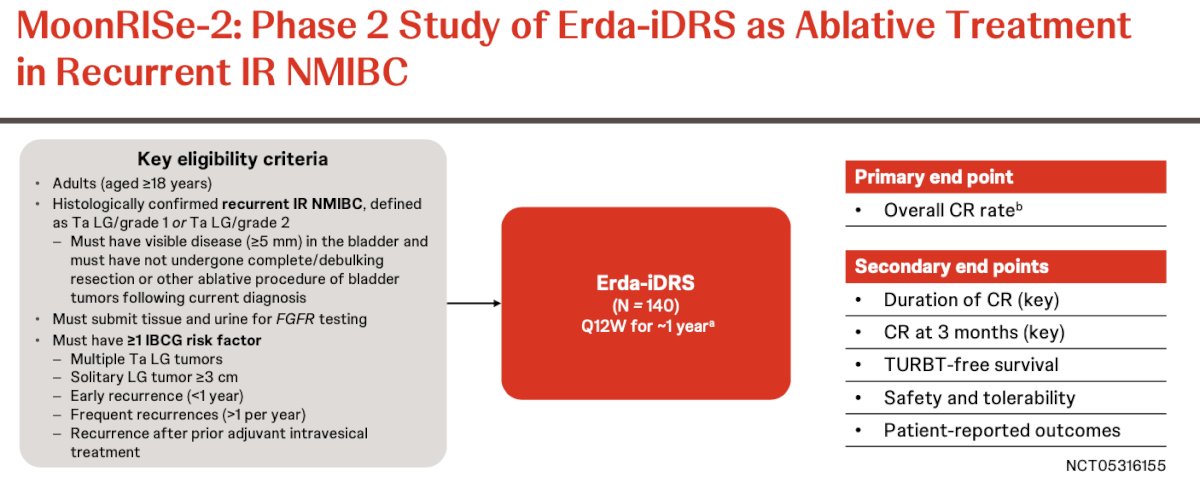
MoonRISe-2 is a phase 2 study evaluating Erda-iDRS (TAR-210) as an ablative treatment strategy in patients with recurrent intermediate-risk NMIBC. Eligible patients include adults with histologically confirmed recurrent low-grade Ta disease who have visible tumors measuring at least 5 mm and who have not undergone complete resection or other ablative procedures following the current diagnosis. Patients are also required to undergo FGFR testing using tissue and urine samples and must harbor at least one IBCG risk factor, including multiple low-grade tumors, solitary tumors ≥3 cm, early recurrence within 1-year, frequent recurrences, or recurrence following prior intravesical therapy.
Patients receive Erda-iDRS every 12 weeks for approximately 1 year. The primary endpoint is overall complete response rate, while key secondary endpoints include duration of complete response, complete response at 3 months, TURBT-free survival, safety and tolerability, and patient-reported outcomes. The study design is shown below:
Dr. Pieczonka noted that MoonRISe-2 represents a phase 2 expansion of the earlier first-in-human study evaluating Erda-iDRS in recurrent IR NMIBC. Treatment response is assessed through cystoscopic evaluation every 12 weeks, with biopsy performed when clinically indicated. He further highlighted that the study began enrollment in April 2025 and has already completed accrual, enrolling 140 patients across 52 sites in 7 countries.
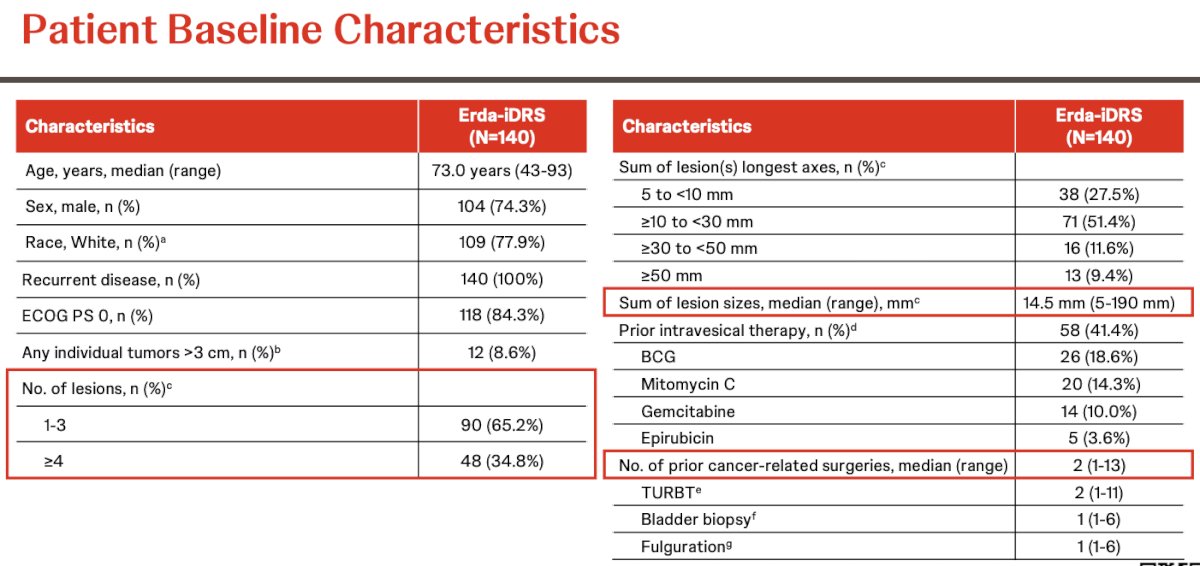
MoonRISe-2 has now fully enrolled, and Dr. Pieczonka reviewed the baseline characteristics of the 140 enrolled patients. The median age was 73 years (range 43–93), and most patients were male (74.3%) and White (77.9%). All patients had recurrent disease, with the majority demonstrating good performance status, including 84.3% with ECOG PS 0.
Notably, tumor burden varied across the cohort. Most patients had between 1–3 lesions (65.2%), while 34.8% had ≥4 lesions. The median cumulative lesion size was 14.5 mm, with a wide range extending from 5–190 mm. Although only 8.6% of patients had an individual tumor larger than 3 cm, over 60% of patients had cumulative lesion burdens ≥10 mm. Dr. Pieczonka also noted that many patients had previously received intravesical therapies, including BCG (18.6%), mitomycin C (14.3%), gemcitabine (10.0%), and epirubicin (3.6%). The cohort was heavily pretreated overall, with a median of 2 prior cancer-related surgeries, including TURBTs, bladder biopsies, and fulgurations. Baseline characteristics are shown in the table below:
Dr. Pieczonka concluded his presentation with the following key messages:
- MoonRISe-2 has successfully completed enrollment in patients with recurrent intermediate-risk NMIBC.
- The enrolled population demonstrated a substantial disease burden, with approximately 35% of patients presenting with ≥4 tumors at baseline.
- Patients were heavily pretreated, with the number of prior TURBT procedures ranging from 1 to 11, and 41% having previously received intravesical BCG or chemotherapy.
- Ongoing phase 3 trials are further evaluating Erda-iDRS in earlier-stage bladder cancer settings, including MoonRISe-1 in FGFR-altered intermediate-risk NMIBC and MoonRISe-3 in BCG-treated papillary-only high-risk NMIBC.
Presented by: Christopher Pieczonka, MD, Associated Medical Professionals of NY, Syracuse, NY
Written by: Julian Chavarriaga, MD, Clinical Assistant Professor, Urologic Oncologist, Department of Urology at Penn State Health @chavarriagaj on Twitter during the American Urological Association (AUA) 2026 Annual Meeting, Washington, DC, Fri, May 15 – Mon, May 18, 2026.
Related content: The MoonRISe-2 Trial and FGFR-Targeted Ablative Therapy in NMIBC - Christopher Pieczonka