The American Urological Association's 2026 Annual Meeting, in Washington D.C., was host to the Clinical Trials in Progress: Bladder Cancer Session. Dr. Brian Mazzarella presented the trial in progress: MoonRISe-3: a phase 3 study of erda-iDRS, an erdafitinib intravesical drug-releasing system, vs intravesical chemotherapy in patients with bacillus Calmette-Guérin–treated high-risk non–muscle-invasive bladder cancer with susceptible FGFR alterations.
Dr. Mazzarella began by noting that TURBT followed by induction and maintenance intravesical BCG remains the standard of care for patients with high-risk papillary NMIBC. However, despite adequate treatment, long-term outcomes remain suboptimal, with 5-year recurrence rates approaching 70% and progression rates reaching up to 40%.
She further highlighted several important clinical challenges associated with BCG therapy, including intolerance in up to 20% of patients and the ongoing global BCG shortage, which has limited the ability of many eligible patients to receive a full induction course. Although radical cystectomy is recommended after failure of BCG and alternative intravesical therapies, the procedure is associated with substantial morbidity, perioperative mortality, and negative effects on quality of life, resulting in relatively low real-world utilization rates.
Importantly, Dr. Mazzarella emphasized that FGFR alterations are identified in approximately 40% of papillary-only high-risk NMIBC tumors and may serve as oncogenic drivers. Despite this biologic rationale, there are currently no approved therapies specifically targeting FGFR-altered, BCG-treated papillary-only high-risk NMIBC.
Oral erdafitinib, a selective pan-FGFR tyrosine kinase inhibitor, is currently approved for the treatment of metastatic urothelial carcinoma harboring susceptible FGFR3 alterations after progression on prior systemic therapy. Dr. Mazzarella highlighted findings from THOR-2 Cohort 1, which evaluated oral erdafitinib in patients with FGFR-altered papillary-only high-risk NMIBC. In that study, erdafitinib prolonged recurrence-free survival compared with intravesical chemotherapy, with median recurrence-free survival not reached versus 11.6 months, respectively. However, systemic treatment was associated with class-related toxicities including hyperphosphatemia, skin and nail toxicities, and central serous retinopathy.
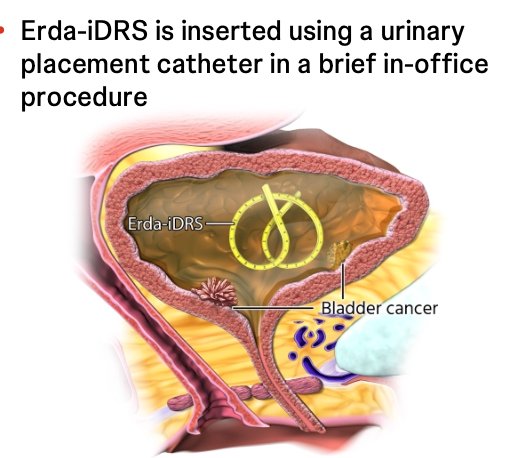
She then introduced Erda-iDRS (TAR-210), a novel intravesical drug-releasing system designed to provide sustained local delivery of erdafitinib directly within the bladder over approximately three months. The device is inserted during a brief in-office procedure using a urinary placement catheter, with the goal of maximizing local drug exposure while minimizing systemic toxicity.
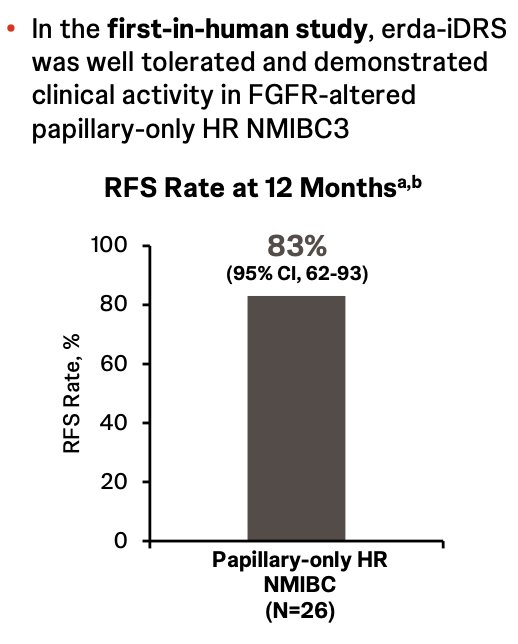
Dr. Mazzarella also reviewed findings from the first-in-human study evaluating Erda-iDRS in FGFR-altered papillary-only high-risk NMIBC. The treatment was reported to be well tolerated and demonstrated encouraging clinical activity, with a 12-month recurrence-free survival rate of 83% (95% CI: 62–93) among 26 treated patients.
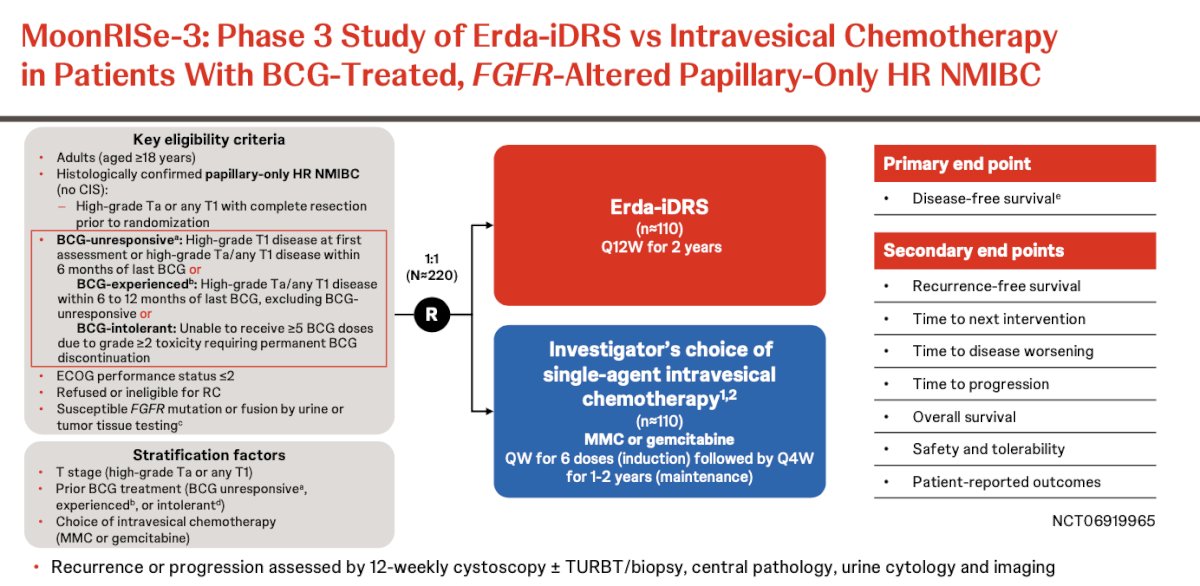
MoonRISe-3 is a phase 3 study evaluating TAR-210 versus intravesical chemotherapy in patients with BCG-treated, FGFR-altered papillary-only high-risk NMIBC. Eligible patients include those with high-grade Ta or T1 disease following complete resection who were either BCG-unresponsive, BCG-exposed, or BCG-intolerant, with FGFR alterations identified through urine or tumor tissue testing.Patients are randomized 1:1 to receive TAR-210 (Erda-iDRS) administered every 12 weeks for up to 2 years or investigator’s choice of single-agent intravesical chemotherapy with mitomycin C or gemcitabine. Chemotherapy is administered weekly for 6 induction doses followed by maintenance every 4 weeks for 1–2 years.
The primary endpoint of the study is disease-free survival. Key secondary endpoints include recurrence-free survival, time to next intervention, time to disease worsening, time to progression, overall survival, safety and tolerability, and patient-reported outcomes. Disease recurrence or progression is assessed with cystoscopy every 12 weeks in combination with TURBT/biopsy, urine cytology, central pathology review, and imaging. The study design is shown below.
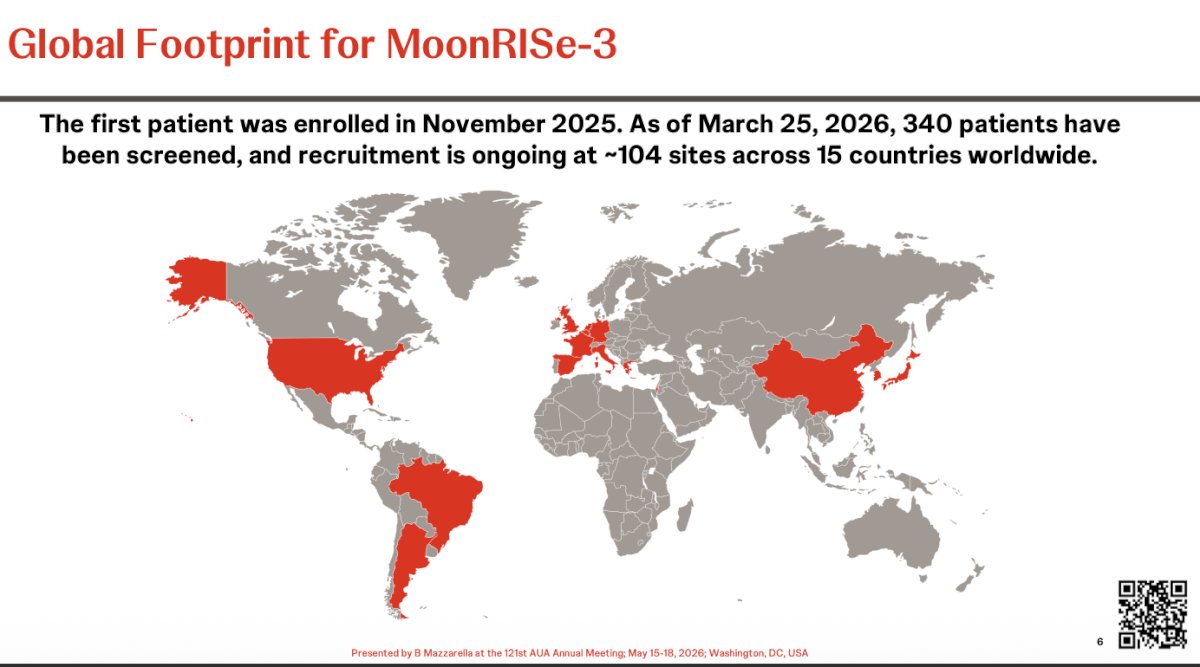
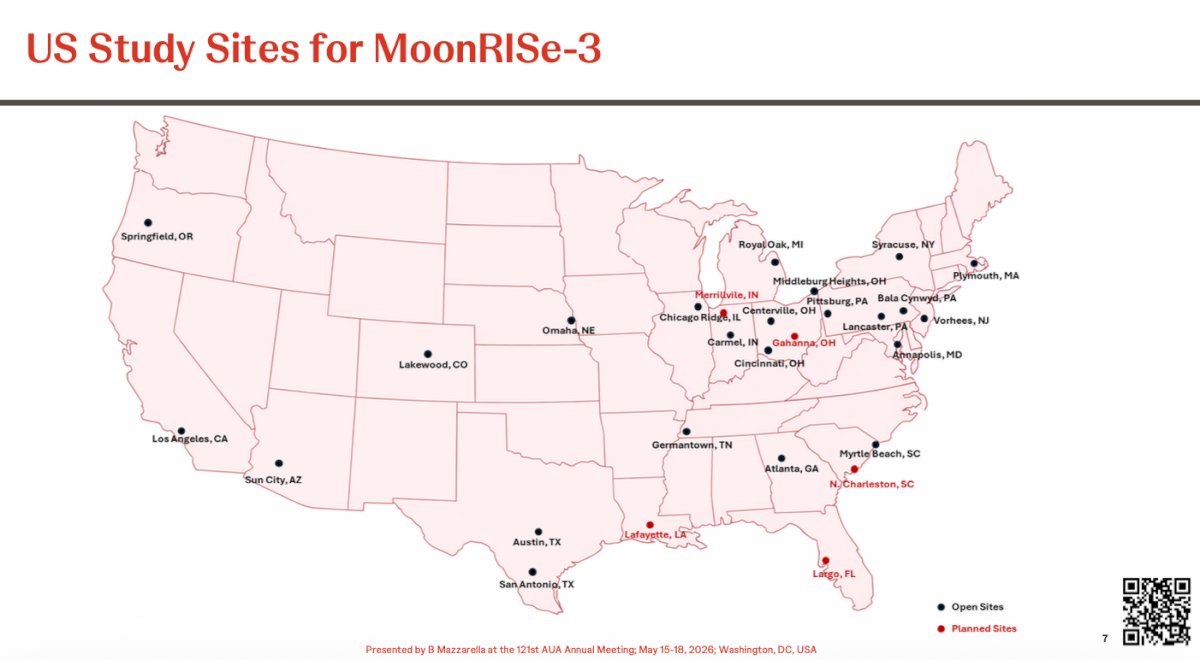
Dr. Mazzarella noted that MoonRISe-3 is being conducted across a broad international network, underscoring the significant global interest in FGFR-targeted bladder-preserving strategies for high-risk NMIBC. The first patient was enrolled in November 2025, and as of March 25, 2026, a total of 340 patients had been screened. Recruitment remains ongoing across approximately 104 sites spanning 15 countries worldwide.
Notably, in the United States, MoonRISe-3 has established a broad network of participating study sites distributed across multiple geographic regions, including major academic and community centers. Active sites are located throughout the Northeast, Midwest, South, and West Coast, with additional planned expansion sites highlighted in states such as Ohio, Louisiana, South Carolina, and Florida, reflecting ongoing efforts to support enrollment and improve patient access nationwide.
Presented by: Brian Mazzarella, MD, FACS, Urologist, Urology Austin, Austin, TX
Written by: Julian Chavarriaga, MD, Clinical Assistant Professor, Urologic Oncologist, Department of Urology at Penn State Health @chavarriagaj on Twitter during the American Urological Association (AUA) 2026 Annual Meeting, Washington, DC, Fri, May 15 – Mon, May 18, 2026.
Related content: MoonRISe-3 Trial Design and Enrollment: Erdafitinib Drug-Releasing System in FGFR-Altered Bladder Cancer - Brian Mazzarella