(UroToday.com) The American Urological Association's 2026 Annual Meeting, in Washington D.C., was host to the Clinical Trials in Progress: Bladder Cancer Session. Dr. Seth Lerner presented the trial in progress: A Phase 2 Multicenter, Open-Label Study Evaluating the Efficacy and Safety of Dabogratinib (TYRA-300) in Participants with FGFR3-Altered Low-Grade, Intermediate Risk Non-Muscle Invasive Bladder Cancer (SURF302).
Dr. Lerner began by highlighting that early-stage urothelial carcinoma remains a major source of morbidity worldwide, with approximately 75% of patients presenting with NMIBC at diagnosis. He noted that despite generally favorable oncologic outcomes, recurrence rates remain high, particularly among patients with intermediate-risk disease, with up to 30% recurring within 1 year and nearly 40% within 2 years.
He emphasized that although progression rates in intermediate-risk NMIBC are relatively low, patients often experience a substantial physical and emotional burden related to repeated TURBT procedures and ongoing intravesical therapy. As a result, there remains an important unmet need for more innovative and patient-friendly treatment approaches in this disease setting.
Dr. Lerner noted that targeting FGFR3 may be particularly relevant in intermediate-risk NMIBC, where more effective therapies are needed to reduce recurrence and disease burden. He explained that FGFR signaling plays a central role in cellular growth, differentiation, and homeostasis, with FGFR3 alterations identified in up to 80% of NMIBC cases and up to 96% of low-grade UTUC tumors.
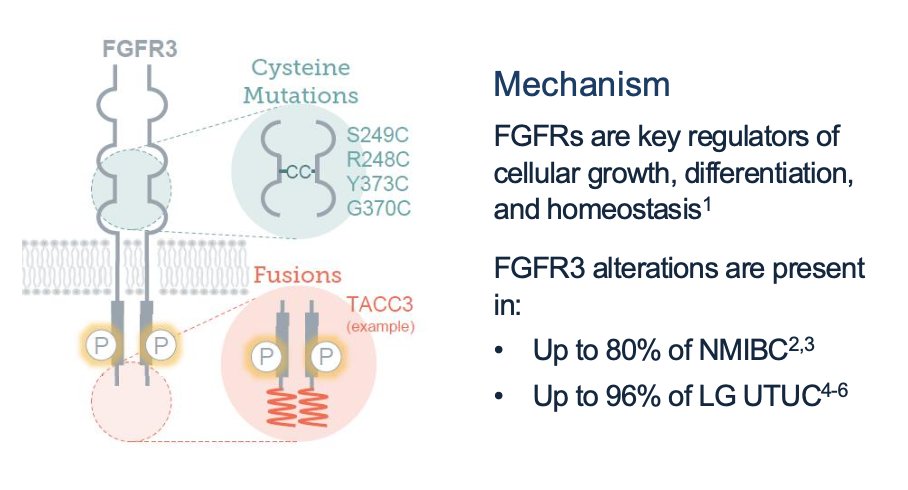
He further highlighted that several pan-FGFR inhibitors, including erdafitinib in advanced urothelial carcinoma, have already received regulatory approval across multiple malignancies. However, currently available FGFR inhibitors lack selectivity for FGFR3 and inhibit FGFR1, 2, and 4 as well, contributing to off-target toxicities such as hyperphosphatemia, nail disorders, stomatitis, and central serous retinopathy. These limitations underscore the need for more selective FGFR3-targeted therapies with improved tolerability profiles.
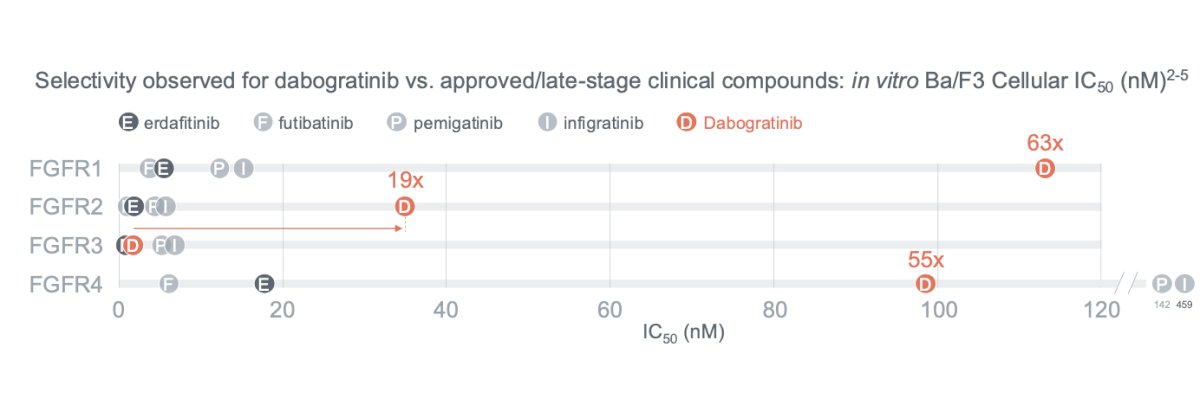
Dabogratinib was specifically designed as a highly selective oral FGFR3 inhibitor with substantially lower activity against FGFR1, FGFR2, and FGFR4 compared with currently available FGFR-targeted therapies. Preclinical data demonstrated markedly greater selectivity for FGFR3 relative to other FGFR isoforms (as shown in the figure below), which may help minimize the off-target toxicities commonly observed with less selective pan-FGFR inhibitors.
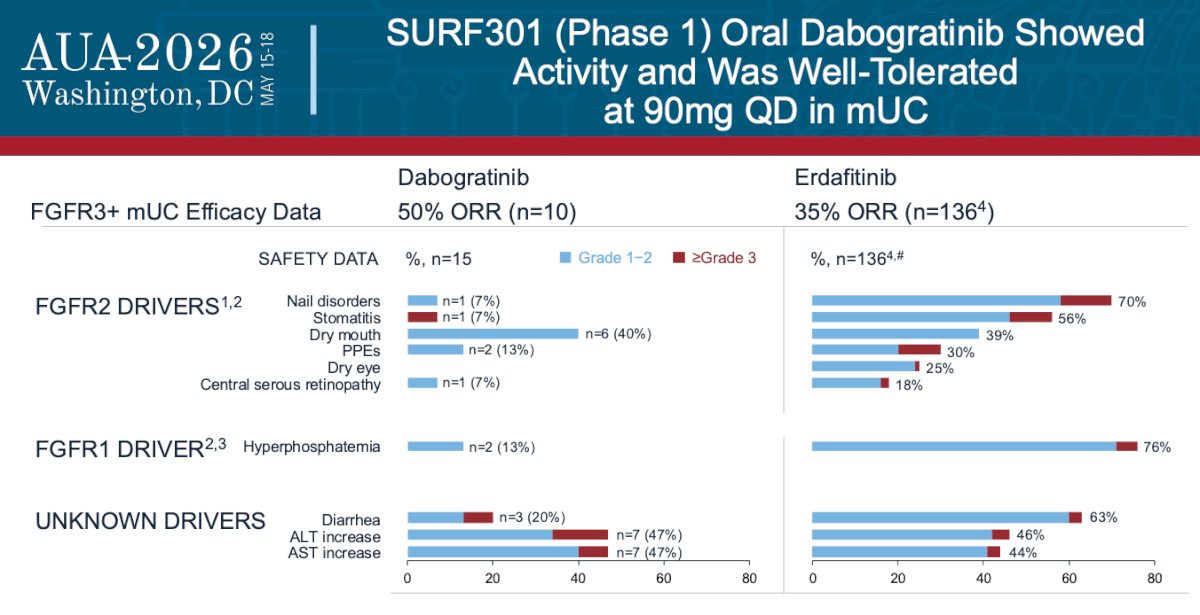
SURF301 was a phase 1 study evaluating oral dabogratinib in patients with metastatic urothelial carcinoma harboring FGFR3 alterations. Dr. Lerner highlighted that dabogratinib demonstrated encouraging preliminary activity, achieving an objective response rate of 50% in a small cohort of evaluable patients treated at the 90 mg once-daily dose level. Importantly, the treatment appeared to be well tolerated, with lower rates of FGFR1- and FGFR2-driven toxicities compared with historical data for erdafitinib. Rates of hyperphosphatemia, stomatitis, nail disorders, and ocular toxicities were notably limited, supporting the potential safety advantage of selective FGFR3 inhibition.
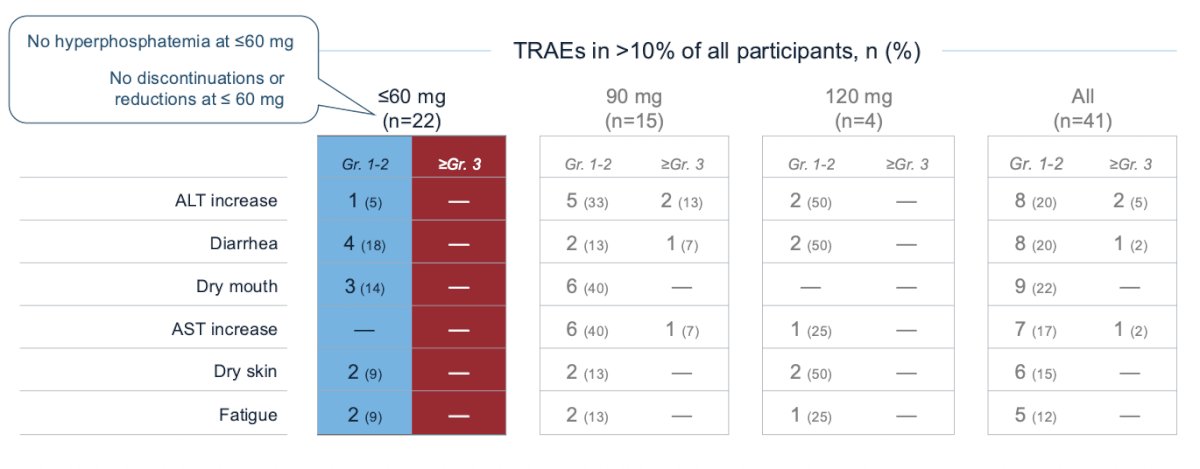
From a safety standpoint, dabogratinib demonstrated a favorable tolerability profile across dose levels. Among patients treated at doses ≤60 mg, no cases of hyperphosphatemia were observed, and there were no dose reductions or treatment discontinuations. The most common treatment-related adverse events were predominantly grade 1–2 and included diarrhea, dry mouth, fatigue, dry skin, and transient ALT elevation. At the 90 mg dose level, a small number of grade ≥3 ALT and AST elevations were reported, while overall rates of FGFR-associated toxicities remained relatively limited.
SURF302 (NCT06995677) is an open-label, phase 2, global study that is designed to explore oral dabogratinib as monotherapy in patients with low-grade intermediate risk non-muscle invasive bladder cancer with activating FGFR3 pathway alterations. Two doses will be initially tested (50 and 60 mg daily, n = 30 each) in a randomized fashion. The study design is presented below:
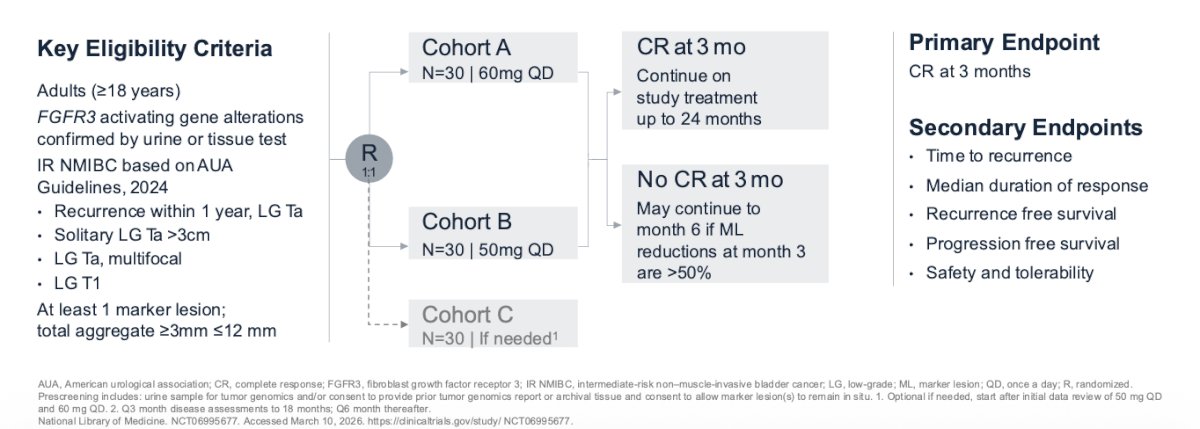
Adult patients with confirmed low-grade intermediate risk non-muscle invasive bladder cancer, at least 1 marker lesion, documented FGFR3 mutation or fusion, no evidence of upper tract disease, and adequate organ function are generally eligible. Participants with a history of muscle-invasive bladder cancer or metastatic disease, who have the presence of disease in the ureter or prostatic urethra or have received prior FGFR inhibitor therapy are excluded. The primary endpoint is the 3-month complete response rate in this population. Additional secondary endpoints include duration of response, safety and tolerability, as well as recurrence-free survival.
Dr Lerner concluded by highlighting that the study is planned for approximately 36 centers in North America, Australia, and Europe, the site list is shown below:

Presented by: Seth Lerner, MD, FACS, Professor of Urology, Baylor College of Medicine, Houston, TX
Written by: Julian Chavarriaga, MD, Clinical Assistant Professor, Urologic Oncologist, Department of Urology at Penn State Health @chavarriagaj on Twitter during the American Urological Association (AUA) 2026 Annual Meeting, Washington, DC, Fri, May 15 – Mon, May 18, 2026.
Reference: