(UroToday.com) The 2026 Society of Urologic Oncology (SUO) Annual Meeting at the American Urological Association (AUA) Annual Meeting featured an important educational session on emerging bladder-preserving strategies for patients with muscle-invasive bladder cancer (MIBC).
In a presentation titled, “How to Assess Response After Perioperative Enfortumab Vedotin and Pembrolizumab in MIBC,” Dr. Elaine Lam reviewed the rapidly evolving evidence supporting perioperative enfortumab vedotin plus pembrolizumab (EV+P), discussed how to define and measure clinical complete response (cCR), and outlined the key unanswered questions that will shape next-generation bladder-sparing clinical trials.

Dr. Lam noted that EV+P has transformed the treatment landscape across both advanced and perioperative bladder cancer settings. In metastatic urothelial carcinoma, the phase 3 EV-302/KEYNOTE-A39 trial established EV+P as the standard first-line therapy.1 In this study of previously untreated locally advanced or metastatic urothelial carcinoma, patients were randomized to EV+P or platinum-based chemotherapy.

The combination significantly improved progression-free survival (median 12.5 vs 6.3 months; HR 0.45, 95% CI 0.38–0.54; p<0.001) and overall survival (median 31.5 vs 16.1 months; HR 0.47, 95% CI 0.38–0.58; p<0.001), with a confirmed objective response rate of 67.7% compared with 44.4% for chemotherapy, including complete response rates of 29.1% versus 12.5%. At 2.5 years of follow-up, durable separation of both progression-free and overall survival curves remained evident, reinforcing the magnitude and durability of the benefit.
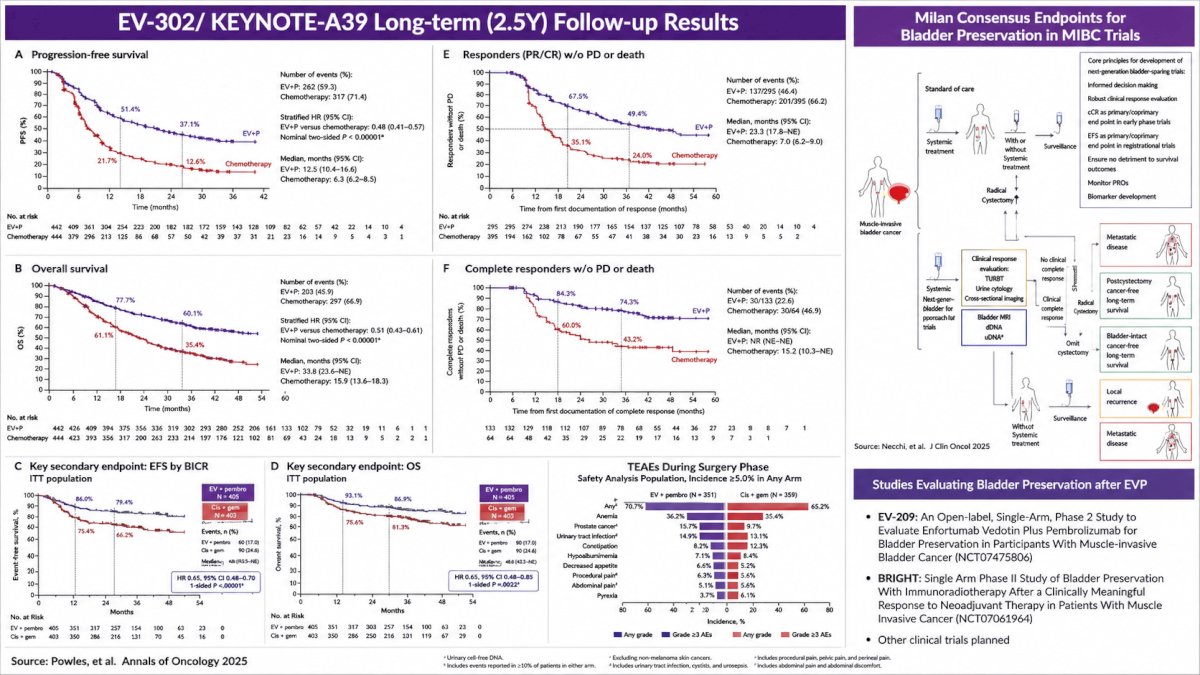
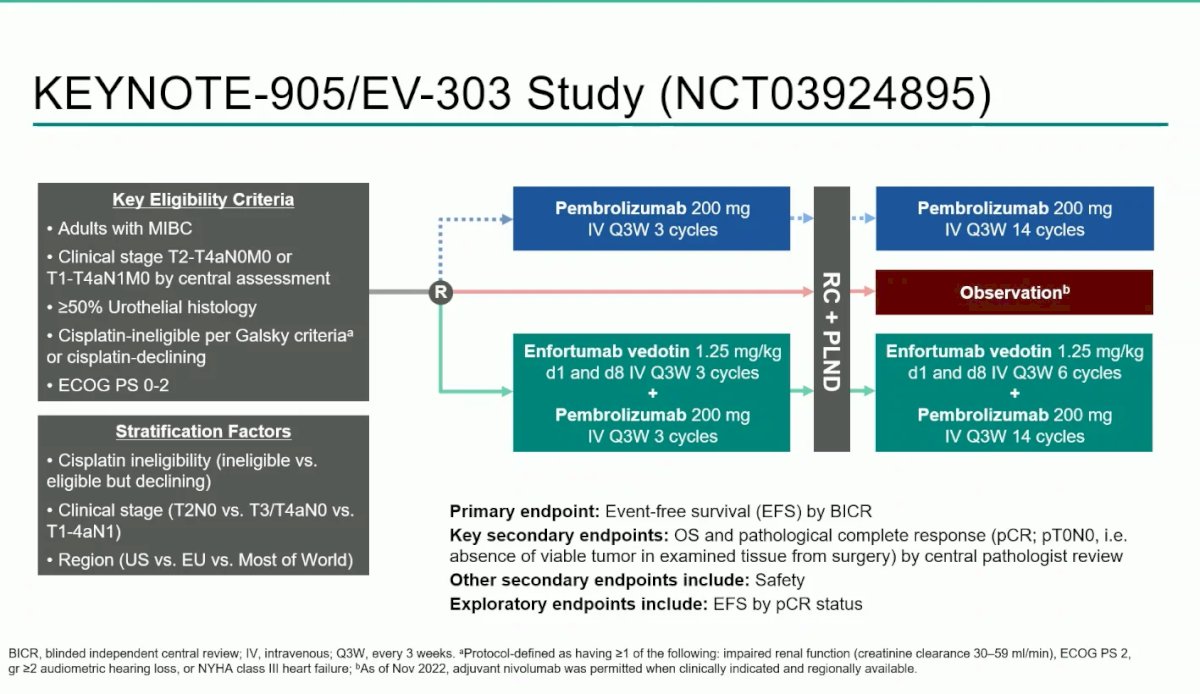
These results prompted the evaluation of EV+P in the perioperative setting. Dr. Lam first reviewed the phase 3 KEYNOTE-905/EV-303 trial (NCT03924895), which enrolled cisplatin-ineligible patients or those declining cisplatin with clinical stage T2–T4aN0M0 or T1–T4aN1M0 urothelial carcinoma.2 Patients were randomized to perioperative EV+P (three neoadjuvant cycles followed by radical cystectomy and pelvic lymph node dissection, then adjuvant EV and pembrolizumab) or surgery with observation/adjuvant pembrolizumab. The trial met both co-primary endpoints. Event-free survival was significantly improved (median not reached vs 15.7 months; HR 0.40, 95% CI 0.28–0.57; p<0.001), and overall survival was also superior (median not reached vs 41.7 months; HR 0.50, 95% CI 0.33–0.74; p<0.001). Pathologic complete response (pT0N0) was achieved in 57.1% of patients receiving EV+P compared with 8.6% in the control arm, representing an absolute improvement of 48.3 percentage points. Overall pathologic downstaging to <pT2N0 occurred in 65.9% versus 12.6%, and among patients who underwent cystectomy, the pCR rate increased to 65.1%.
Dr. Lam then reviewed the phase 3 KEYNOTE-B15/EV-304 trial (NCT04700124), which enrolled cisplatin-eligible patients with clinical stage T2–T4aN0M0 or T1–T4aN1M0 disease. Participants were randomized to four cycles of neoadjuvant EV+P followed by radical cystectomy and adjuvant EV+P, or to four cycles of neoadjuvant gemcitabine/cisplatin followed by cystectomy and observation or adjuvant nivolumab according to standard practice.
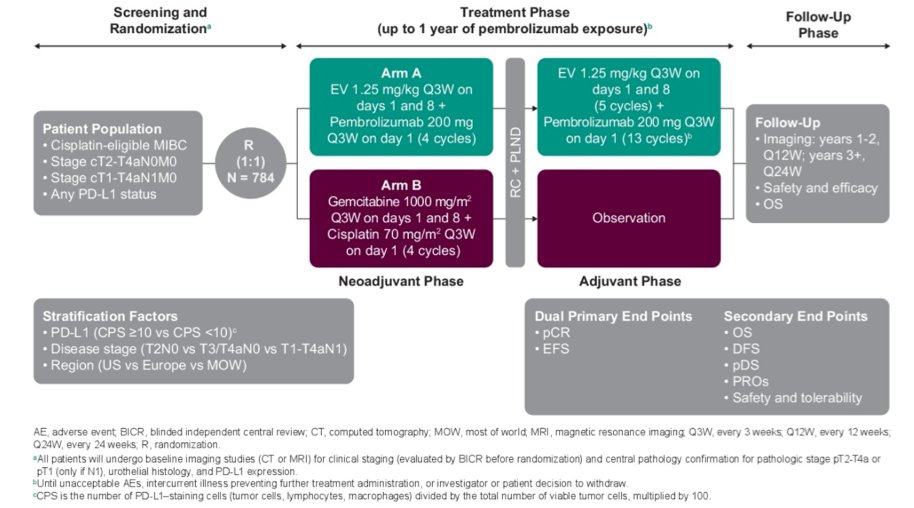
The study demonstrated significant improvements in both event-free survival and overall survival. Event-free survival by blinded independent central review improved with a hazard ratio of 0.53 (95% CI 0.41–0.70; p<0.001), while overall survival improved with a hazard ratio of 0.65 (95% CI 0.48–0.89; p=0.0029). Pathologic complete response was achieved in 55.8% of patients receiving EV+P compared with 32.5% with gemcitabine/cisplatin. Overall pathologic downstaging to <pT2N0 occurred in 63.7% versus 45.2%, and among those undergoing cystectomy, the pCR rate was 64.4%. Importantly, the surgical safety profile was favorable, with no unexpected perioperative toxicities.

Taken together, EV-303 and EV-304 demonstrated consistent pathologic results despite enrolling different patient populations. In the cisplatin-ineligible setting, EV+P produced a pCR rate of 57.1% and reduced non-downstaged disease to 19.4%. In cisplatin-eligible patients, pCR was 55.8%, with only 21% failing to achieve pathologic downstaging. Dr. Lam emphasized that these response rates are among the highest ever reported in perioperative MIBC and substantially exceed historical benchmarks with chemotherapy alone.
A central concept in the presentation was the definition of event-free survival, particularly because it has implications for bladder-preserving approaches. In KEYNOTE-B15, EFS was defined as the time from randomization to radiographic progression precluding surgery, biopsy-proven residual MIBC in patients who did not undergo surgery, inability to complete curative-intent surgery due to unresectable or metastatic disease, local or distant recurrence after surgery, or death from any cause. Importantly, the mere omission of cystectomy was not considered an event; patients who did not undergo surgery continued to be followed with serial imaging. Dr. Lam highlighted that this design feature is especially relevant when considering risk-adapted strategies in which selected patients with robust responses may defer cystectomy.
The striking pathologic response rates observed in EV-303 and EV-304 have fundamentally altered expectations for bladder preservation. Dr. Lam posed several key unanswered questions: How should cCR be defined after EV+P? Should response assessment occur after three versus four cycles of therapy? Can patients achieving cCR safely omit radical cystectomy without compromising long-term oncologic outcomes? If cystectomy is omitted, should systemic therapy continue in an “adjuvant” fashion?
To address these issues, Dr. Lam reviewed the 2025 Milan Consensus statement published in the Journal of Clinical Oncology by Andrea Necchi and colleagues.4 This multidisciplinary effort established core design principles for next-generation bladder-preservation trials. The recommended definition of cCR includes:- No evidence of high-grade malignancy on repeat transurethral resection and directed biopsies of all visually abnormal areas and the original tumor site;
- Negative urine cytology;
- No definitive local or metastatic disease on cross-sectional imaging. Additional emerging biomarkers, including bladder MRI, circulating tumor DNA, and urine tumor DNA, may further refine response assessment.
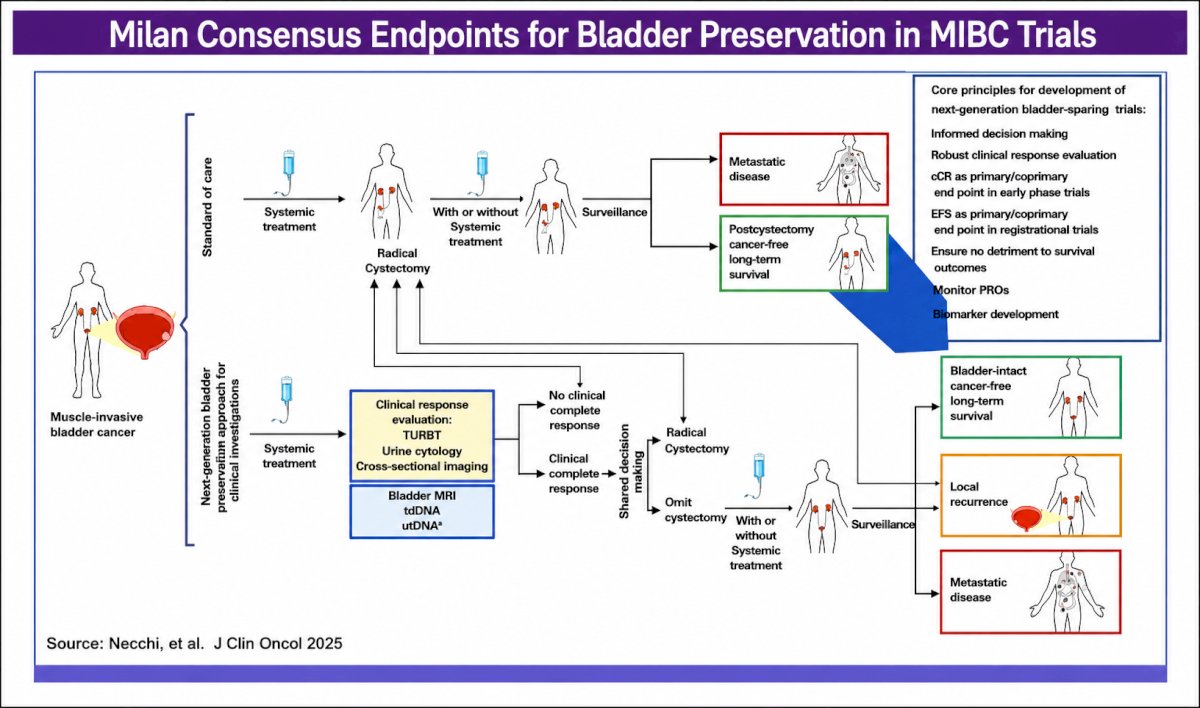
The consensus group recommended that cCR be used as a primary or co-primary endpoint in early-phase studies, whereas event-free survival should serve as the preferred primary endpoint in registrational bladder-preservation trials. Secondary endpoints should include overall survival, patient-reported outcomes, bladder-intact cancer-free survival, local recurrence, and biomarker development. Above all, new strategies must demonstrate no detriment to long-term survival compared with standard radical cystectomy.
Dr. Lam also reviewed prior risk-adapted bladder-sparing experiences that provide proof of concept. In the RETAIN-1 and RETAIN-2 studies, patients with DNA damage response gene alterations (ATM, RB1, FANCC, or ERCC2) who achieved cCR after neoadjuvant dose-dense MVAC underwent active surveillance with or without nivolumab, resulting in 2-year metastasis-free survival rates of 72.9% and 77.4%, respectively. In HCRN GU16-257, patients received gemcitabine, cisplatin, and nivolumab followed by extensive restaging with cystoscopy, biopsies, urine cytology, and MRI/CT. Those achieving cCR deferred cystectomy and received maintenance nivolumab, with 2-year overall survival of 100%, metastasis-free survival of 96.6%, and bladder-intact survival of 72.2%.
The next generation of EV+P-based bladder-preservation trials is already underway. The phase 2 EV-209 trial (NCT07475806) is evaluating EV+P as a bladder-preserving strategy in MIBC. The BRIGHT trial (NCT07061964) is assessing bladder preservation with immunoradiotherapy in patients achieving a clinically meaningful response after neoadjuvant therapy. Additional studies are in development and are expected to further clarify whether the exceptional response rates observed with EV+P can be translated into durable bladder-intact survival.
Dr. Lam concluded that perioperative EV+P has fundamentally changed the therapeutic landscape in muscle-invasive bladder cancer. The extraordinarily high pathologic complete response and downstaging rates observed in EV-303 and EV-304 provide a strong biologic rationale for carefully designed bladder-preservation strategies. However, the success of these approaches will depend on rigorous and standardized response assessment, thoughtful endpoint selection, incorporation of novel biomarkers, and, most importantly, confirmation that omission of radical cystectomy does not compromise long-term survival outcomes.
Presented by: Elaine Lam, MD, Professor, Department of Medicine, Division of Medical Oncology, University of Colorado, Denver, CO
Written by: Rashid K. Sayyid, MD, MSc, Assistant Professor, Urologic Oncologist, Department of Urology at The University of Arizona and Banner University Medical Center, Tucson, AZ – @rksayyid on X during the American Urological Association (AUA) 2026 Annual Meeting, Washington, DC, Fri, May 15 – Mon, May 18, 2026.
References:
- Powles T, Valderrama BP, Gupta S, et al. Enfortumab vedotin and pembrolizumab in untreated advanced urothelial cancer. N Engl J Med. 2024;390(10):875–888.
- Vulsteke C, Adra N, Danchaivijitr P, et al. Perioperative Enfortumab Vedotin and Pembrolizumab in Bladder Cancer. N Engl J Med. 206;394:1257-1269.
- Galsky MD, Pérez-Valderrama B, Maruzzo M, et al. Neoadjuvant and Adjuvant Enfortumab Vedotin Plus Pembrolizumab for Participants With Muscle-Invasive Bladder Cancer Who Are Eligible for Cisplatin: Randomized, Open-Label, Phase 3 KEYNOTE-B15 Study. J Clin Oncol. 2026;44(7 Suppl):LBA630.
- Necchi A, Galsky MD, Dizman N, et al. End Points for the Next-Generation Bladder-Sparing Perioperative Trials for Patients With Muscle-Invasive Bladder Cancer. J Clin Oncol. 2025;43(32):3536-3544.