(UroToday.com) The American Urological Association's 2026 Annual Meeting, was host to the IP50: Bladder Cancer: Non-Invasive IV Session. Dr. Kyle Richards presented interactive poster IP50-10: A Histopathology-Driven AI Biomarker for Predicting Progression, High-Grade Recurrence, and Early BCG Failure in NMIBC.
Dr. Richards began by noting that intravesical BCG remains the standard of care for patients with intermediate- and high-risk NMIBC. However, despite appropriate treatment, a substantial proportion of patients ultimately experience recurrence, progression, or treatment failure. He emphasized that currently available clinicopathologic variables provide only limited ability to accurately stratify risk and predict outcomes following BCG therapy
The investigators developed and validated an AI-based prognostic model using H&E-stained whole-slide images from BCG-naïve NMIBC TURBT specimens. The training cohort included 355 patients, of whom 291 received adequate BCG therapy, while external validation was performed in an independent cohort of 176 patients.
The AI framework utilized foundation model–derived tile embeddings aggregated through attention-based multiple instance learning to generate a continuous AI-derived risk score. The model was trained to identify patients with persistent disease or relapse within 2 years. In addition to the standalone AI model, the investigators also evaluated a multimodal approach combining the AI risk score with tumor focality to improve predictive performance.
Clinical endpoints included progression-free survival, defined as progression to muscle-invasive disease, nodal involvement, or distant metastasis; high-grade disease-free survival, defined as time to high-grade recurrence, progression, cystectomy, or NMIBC-related death; and early BCG failure, defined as persistent high-grade disease within 9 months of diagnosis. Associations between AI-derived risk scores and clinical outcomes were evaluated using Cox proportional hazards models and logistic regression analyses.
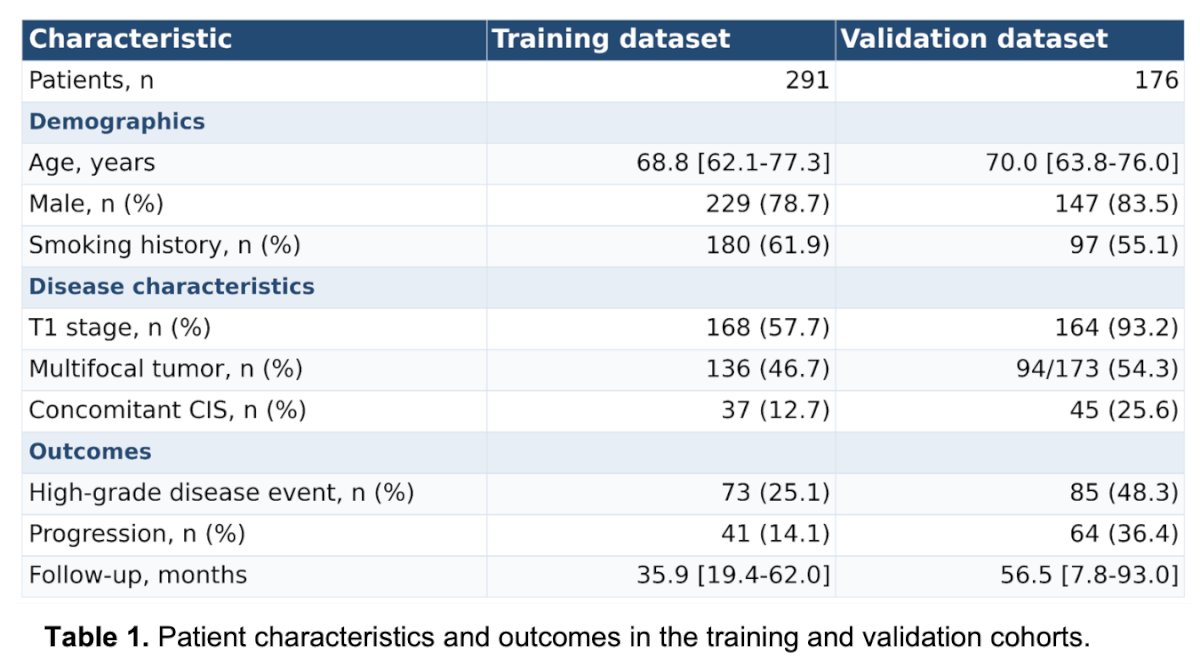
Baseline characteristics were generally comparable between the training and validation cohorts, which included 291 and 176 patients, respectively. Median age was approximately 69–70 years, and most patients were male with a history of smoking. The validation cohort demonstrated a higher proportion of T1 disease and concomitant CIS compared with the training cohort. Clinical outcomes were also more adverse in the validation dataset, with higher rates of high-grade disease events (48.3% vs 25.1%) and progression (36.4% vs 14.1%), along with longer median follow-up duration.
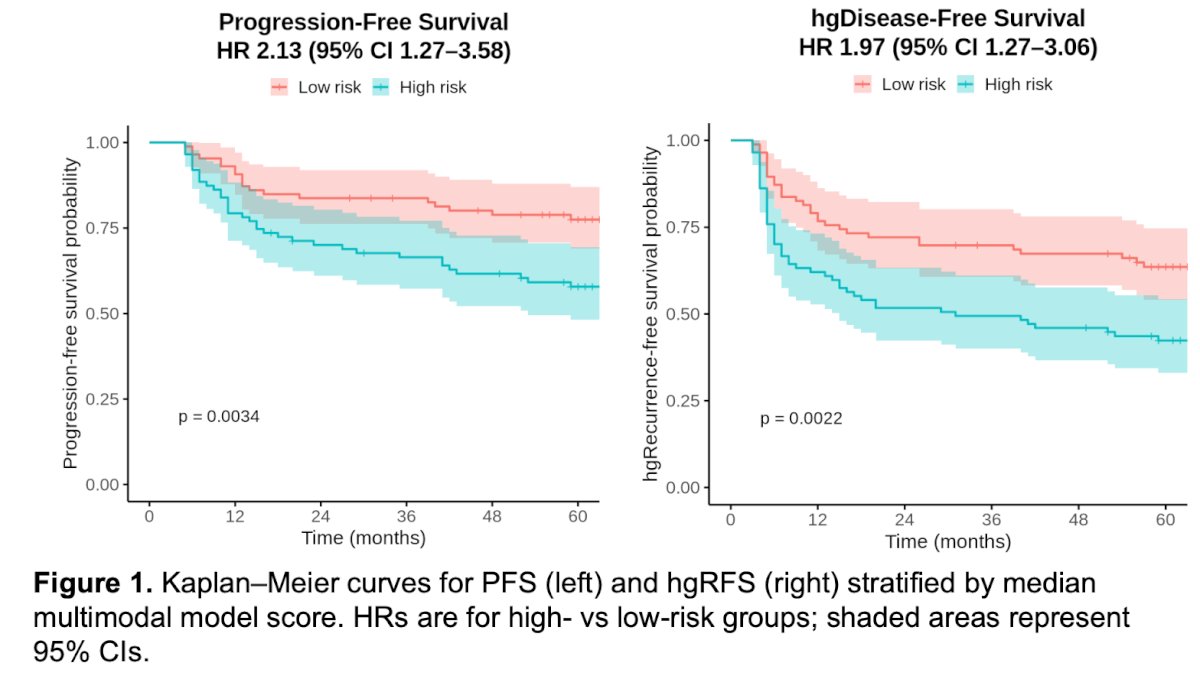
Moreover, the multimodal AI model successfully stratified patients into distinct risk groups with significantly different oncologic outcomes. Patients classified as high risk demonstrated significantly worse progression-free survival compared with low-risk patients (HR 2.13, 95% CI 1.27–3.58; p=0.0034). Similarly, high-risk patients had inferior high-grade disease-free survival (HR 1.97, 95% CI 1.27–3.06; p=0.0022). Kaplan–Meier analyses demonstrated early and sustained separation between the risk groups across follow-up.
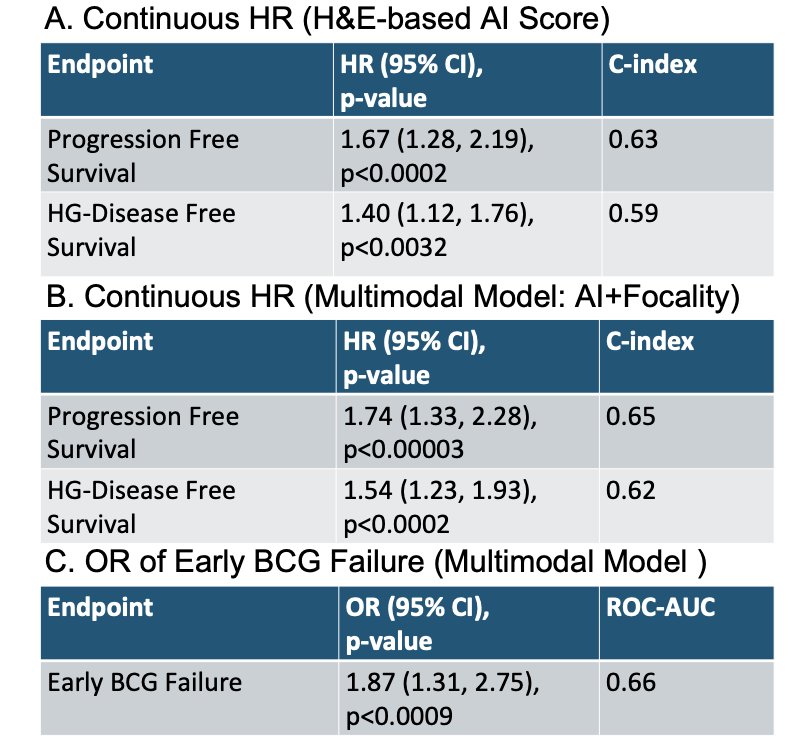
Similarly, both the standalone H&E-based AI score and the multimodal model incorporating tumor focality were significantly associated with adverse clinical outcomes in BCG-treated NMIBC. The multimodal model demonstrated improved predictive performance for progression-free survival (HR 1.74, p<0.00003) and high-grade disease-free survival (HR 1.54, p<0.0002), with C-index values of 0.65 and 0.62, respectively. In addition, the multimodal model was significantly associated with early BCG failure (OR 1.87, 95% CI 1.31–2.75; p<0.0009), achieving an area under the curve (AUC) of 0.66.
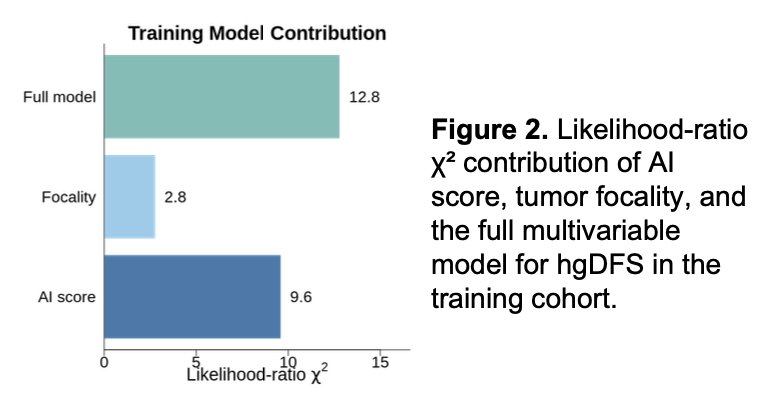
Lastly, the investigators demonstrated that the AI-derived score contributed substantially to the predictive performance of the multimodal model for high-grade disease-free survival in the training cohort. The H&E-based AI score accounted for a larger likelihood-ratio χ² contribution than tumor focality alone (9.6 vs 2.8), supporting the independent prognostic value of the AI biomarker within the combined model.
Dr. Richards concluded with the following key messages:
- The AI-derived biomarker successfully stratified BCG-treated NMIBC patients according to risk of progression-free survival, high-grade disease-free survival, and early BCG failure
- Integration of the AI score with tumor focality improved predictive performance, supporting complementary prognostic value beyond standard clinicopathologic factors
- The multimodal model may help identify patients at higher risk of progression or high-grade recurrence following BCG therapy
- These findings support the potential role of AI-based pathology biomarkers in improving personalized risk stratification and treatment decision-making in NMIBC
Presented by: Kyle Richards, MD, FACS, Associate Professor, University of Wisconsin School of Medicine and Public Health, Madison, WI
Written by: Julian Chavarriaga, MD, Clinical Assistant Professor, Urologic Oncologist, Department of Urology at Penn State Health @chavarriagaj on Twitter during the American Urological Association (AUA) 2026 Annual Meeting, Washington, DC, Fri, May 15 – Mon, May 18, 2026.