(UroToday.com) The 2026 AUA annual meeting featured an invasive bladder cancer session and a presentation by Dr. Zhuo Su discussing a cost-effectiveness analysis of competing treatment strategies for cisplatin-eligible muscle invasive bladder cancer in the era of immune checkpoint inhibitors. For cisplatin-eligible patients with localized muscle invasive bladder cancer, cisplatin-based neoadjuvant chemotherapy followed by radical cystectomy has long been the standard of care. However, immune checkpoint inhibitors have transformed this paradigm, with risk-adapted adjuvant nivolumab,1 and more recently, neoadjuvant durvalumab + gemcitabine + cisplatin and adjuvant durvalumab (“perioperative/sandwich” immunotherapy)2 showing oncological and survival benefits. At the AUA 2026 annual meeting, Dr. Su and colleagues evaluated the cost-effectiveness of these emerging treatment strategies for cisplatin-eligible muscle invasive bladder cancer.
For this study, the investigators created a decision-analytic Markov model using efficacy and safety data from the NIAGARA trial for neoadjuvant gemcitabine + cisplatin + durvalumab followed by radical cystectomy and adjuvant durvalumab, and neoadjuvant gemcitabine + cisplatin followed by radical cystectomy (“comparison”). In the comparison arm, patients with pT3-4 or pN+ disease after radical cystectomy were considered high risk and modeled to receive adjuvant nivolumab, with added survival benefit and impact on quality of life modeled using the CheckMate 274 trial efficacy data. Dr. Su calculated life years, quality adjusted life years, and direct medical costs from a Medicare payer perspective over a 5-year time horizon. Additionally, probabilistic sensitivity analysis was conducted.
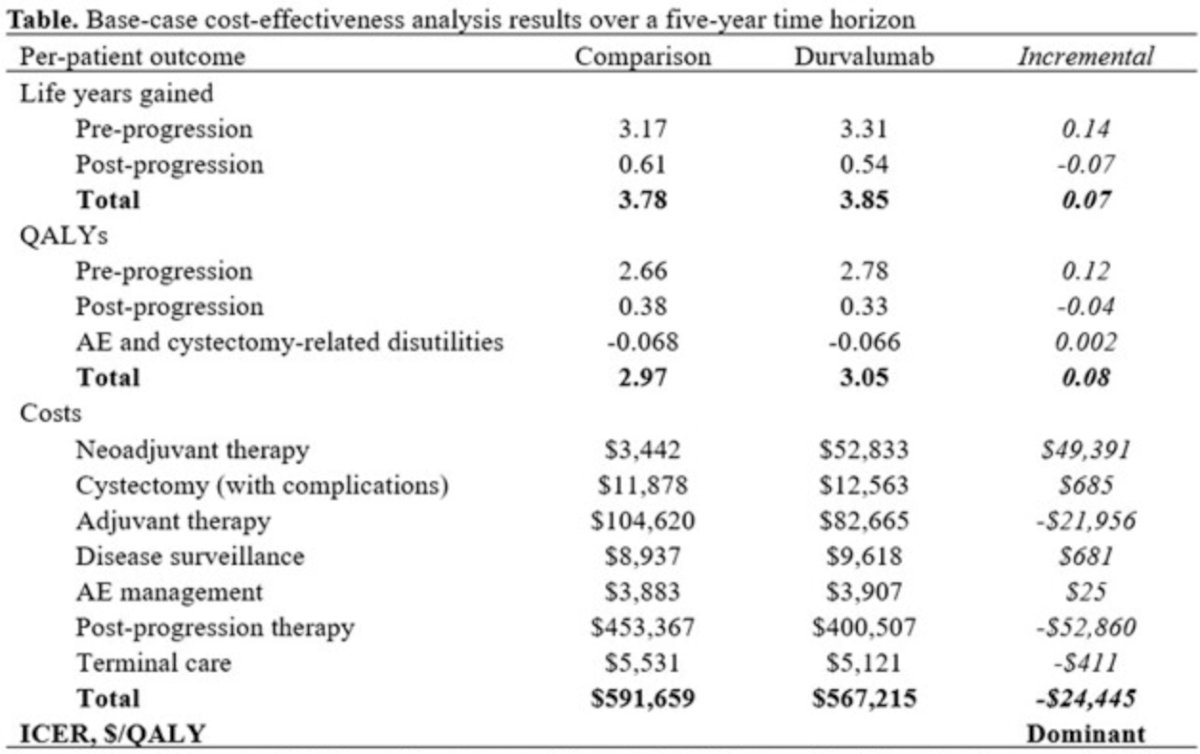
Over a 5-year horizon the durvalumab arm achieved greater life years (3.85 versus 3.78) and quality adjusted life years (3.05 versus 2.97). Higher upfront treatment costs incurred by adding durvalumab were offset by a greater reduction of post-progression treatment costs, leading to lower total costs ($567,215 versus $591,659):
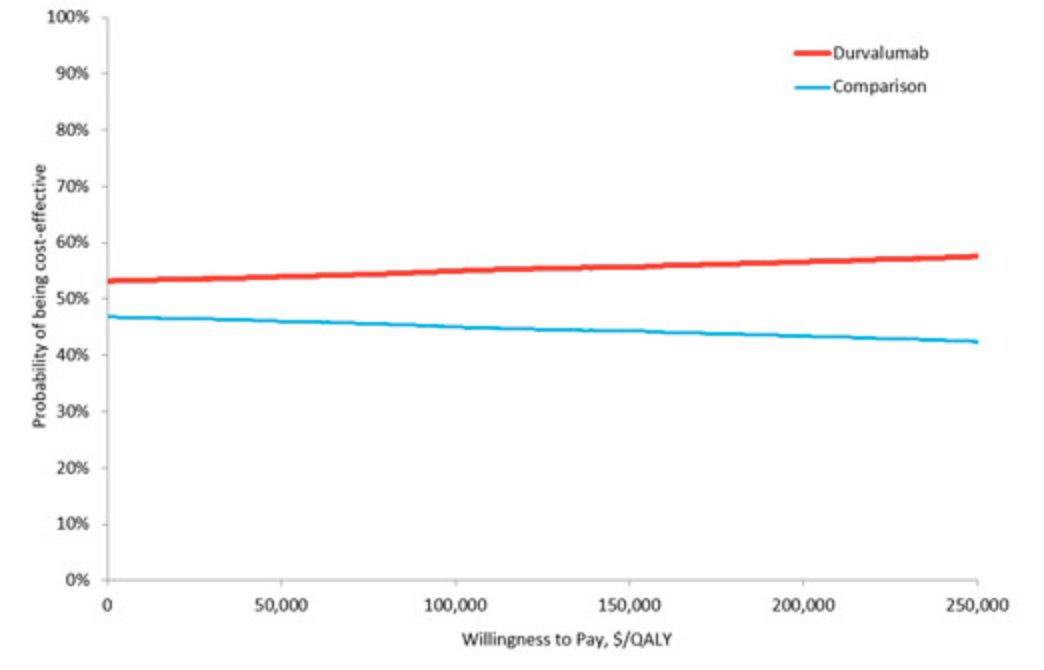
The results were robust in the probabilistic sensitivity analysis:
Dr. Su concluded this presentation discussing a cost-effectiveness analysis of competing treatment strategies for cisplatin-eligible muscle invasive bladder cancer in the era of immune checkpoint inhibitors with the following take home points:
- In the US, adding perioperative durvalumab to neoadjuvant gemcitabine + cisplatin for treating cisplatin-eligible muscle invasive bladder cancer is likely life-extending and cost-effective compared with the current standard strategy of cisplatin-based neoadjuvant chemotherapy followed by risk-adapted adjuvant nivolumab
- These findings support adopting perioperative durvalumab with neoadjuvant gemcitabine + cisplatin as potentially the new standard treatment for cisplatin-eligible muscle invasive bladder cancer
Presented by: Zhuo Su, MD, Johns Hopkins Hospital, Baltimore, MD
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the American Urological Association (AUA) 2026 Annual Meeting, Washington, DC, Fri, May 15 – Mon, May 18, 2026.
References:
- Bajorin DF, Witjes JA, Gschwend JE, et al. Adjuvant nivolumab versus placebo in muscle-invasive urothelial carcinoma. N Engl J Med. 2021 Jun 3;384(22):2102-2114.
- Powles T, Catto JWF, Galsky MD, et al. Perioperative Durvalumab with Neoadjuvant Chemotherapy in Operable Bladder Cancer. N Engl J Med. 2024 Nov 14;391(1):1773-1786.