(UroToday.com) The 2026 American Urologic Association (AUA) Annual Meeting was host to an invasive bladder cancer poster session. Matthew Kirschenbaum presented findings from the University of Washington Bounceback Cohort study assessing patient-reported recovery trajectories following radical cystectomy.
Recovery after radical cystectomy varies substantially among older patients, yet the longitudinal patterns of recovery across functional domains remain incompletely characterized. The investigators hypothesized that baseline frailty would be associated with distinct multidomain patient-reported recovery trajectories following RC.
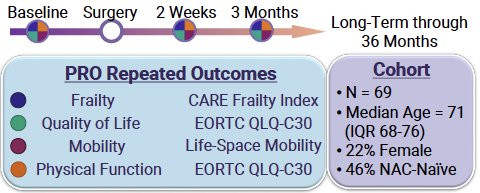
This was a prospective cohort study with planned follow-up extending to three years. Eligible patients were aged 60 years or older with non-metastatic bladder cancer undergoing radical cystectomy. Baseline frailty was assessed using the Cancer and Aging Resilience Evaluation Frailty Index (CARE-FI), a continuous measure ranging from 0 (less frailty) to 1 (greater frailty). Patients were stratified into quartiles according to baseline frailty, with Q1 representing the least frail and Q4 the frailest.
Patient-reported outcomes (PROs) were collected at baseline, two weeks after surgery, three months after surgery, and longitudinally through 36 months. Four domains were evaluated:
- Frailty, using repeated CARE-FI assessments
- Quality of life, using the EORTC QLQ-C30 global quality of life score
- Mobility, using the Life-Space Mobility Questionnaire
- Physical function, using the EORTC QLQ-C30 physical function scale
Recovery trajectories were analyzed using linear mixed-effects models, which demonstrated significant differences across frailty quartiles for all four domains, with marginal R² values of 0.70 for frailty, 0.52 for physical function, 0.46 for quality of life, and 0.28 for mobility, indicating that baseline frailty explained a substantial proportion of variation in postoperative recovery patterns.
The study included 69 patients, with a median age of 71 years (interquartile range 68–76). Seventy-eight percent were male, and approximately half received neoadjuvant chemotherapy. Frailty quartiles were balanced, with 17–18 patients per subgroup.
The central figure displayed four parallel line plots illustrating trajectories for mobility, global quality of life, physical function, and frailty from baseline to two weeks and three months after surgery. Across all domains, statistically significant differences were observed by baseline frailty quartile (mobility p<0.001, quality of life p=0.02, physical function p=0.03, frailty p<0.001).
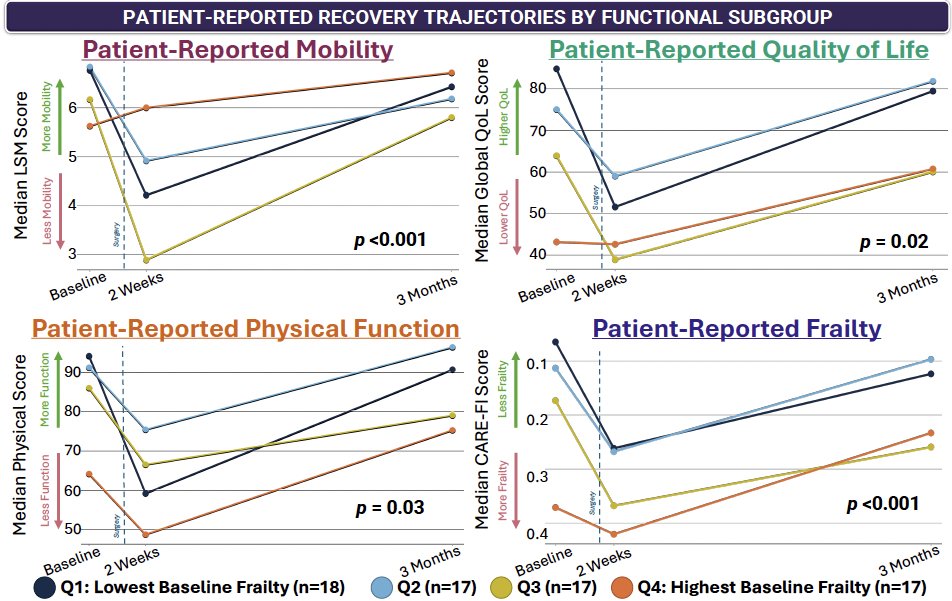
Patients in the least frail quartile (Q1) experienced a pronounced early postoperative decline across mobility, quality of life, and physical function, with approximately 40% reductions at two weeks. However, these patients demonstrated robust recovery by three months, returning to approximately 95–96% of their baseline function.
In contrast, patients in the frailest quartile (Q4) began with the lowest baseline scores but were the only subgroup to improve beyond their preoperative baseline by three months across all four domains, including mobility, physical function, quality of life, and frailty. As noted by the authors, this pattern may reflect either meaningful functional gains resulting from definitive treatment and recovery support or floor effects inherent to baseline patient-reported outcome measures.
These divergent trajectories translated into clinically relevant perioperative differences. Median hospital length of stay increased from approximately 6 days in Q1 to 8 days in Q4 (p<0.05). New mobility aid use ranged from 0% in the least frail patients to 41% in the frailest patients (p<0.05). Rates of postoperative complications and readmissions did not differ significantly across frailty quartiles.
The investigators concluded that baseline frailty is associated with distinct multidomain recovery phenotypes following radical cystectomy, with important implications for personalized preoperative risk assessment, shared decision-making, and perioperative supportive care. Patients with lower baseline frailty may benefit from early rehabilitation to accelerate return to baseline, whereas those with greater frailty may require more sustained postoperative support despite demonstrating meaningful gains over time.
Presented by: Matthew Kirschenbaum, Medical Student, University of Washington, Seattle, WA
Written by: Rashid K. Sayyid, MD, MSc, Assistant Professor, Urologic Oncologist, Department of Urology at The University of Arizona and Banner University Medical Center, Tucson, AZ – @rksayyid on X during the American Urological Association (AUA) 2026 Annual Meeting, Washington, DC, Fri, May 15 – Mon, May 18, 2026.