(UroToday.com) The 2026 American Urological Association annual meeting featured an invasive bladder cancer session and a presentation by Dr. Pietro Scilipoti discussing a study evaluating the surrogacy of intermediate clinical endpoints for overall survival after perioperative treatment in muscle-invasive bladder cancer patients undergoing radical cystectomy.
Overall survival remains the gold standard endpoint in muscle-invasive bladder cancer trials, but requires prolonged follow-up, delaying the evaluation of novel perioperative strategies. Intermediate clinical endpoints such as event-free survival, pathological complete response, and pathological objective response are increasingly reported, yet their formal validation as surrogates for overall survival in muscle-invasive bladder cancer is lacking.
Dr. Scilipoti and colleagues performed a systematic review and meta-analysis (PROSPERO CRD420251050357) of prospective randomized controlled trials and non-randomized trials published between January 2003 and April 2025, evaluating perioperative systemic therapy in muscle-invasive bladder cancer. Intermediate clinical endpoints included event-free survival, pathological complete response, and pathological objective response. A two-stage meta-analytic surrogacy validation was conducted:
- Trial-level association between intermediate clinical endpoint and overall survival (R2 ≥ 0.7 threshold) was tested using weighted linear regression (inverse variance weighting)
- Correlation of treatment effects [log(HR-overall survival) versus log(HR-intermediate clinical endpoint)] was assessed with weighted linear regression (inverse variance weighting), to estimate R2 and the surrogate threshold effect
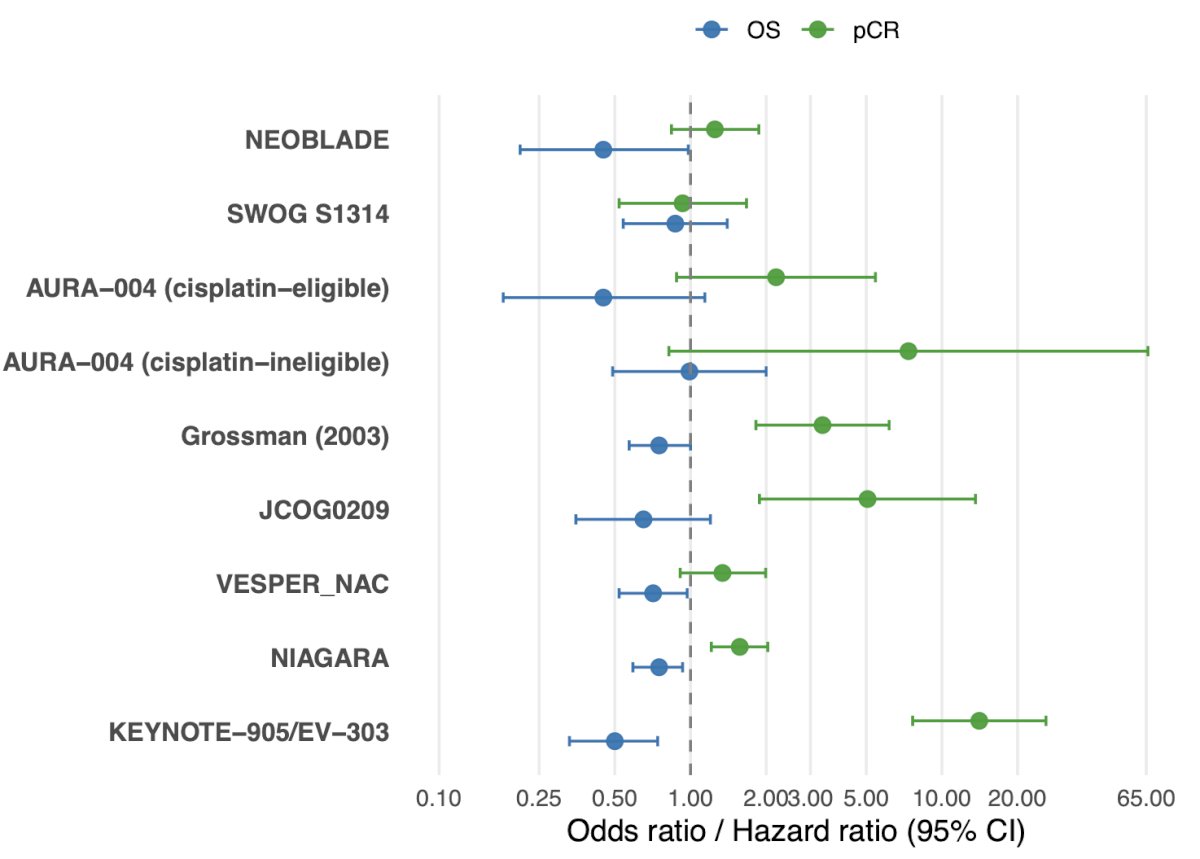
This study included 23 trials on perioperative therapy in muscle-invasive bladder cancer, with 12 reporting on pathological complete response and overall survival. The following figure highlights pathologic complete response odds ratios and overall survival hazard ratios for included trials:
In the perioperative population, event-free survival showed moderate correlation (R2 = 0.59, surrogate threshold effect = 0.67), improving to strong correlation (R2 = 0.87, surrogate threshold effect = 0.79) when excluding high-bias trials and deferred adjuvant chemotherapy:
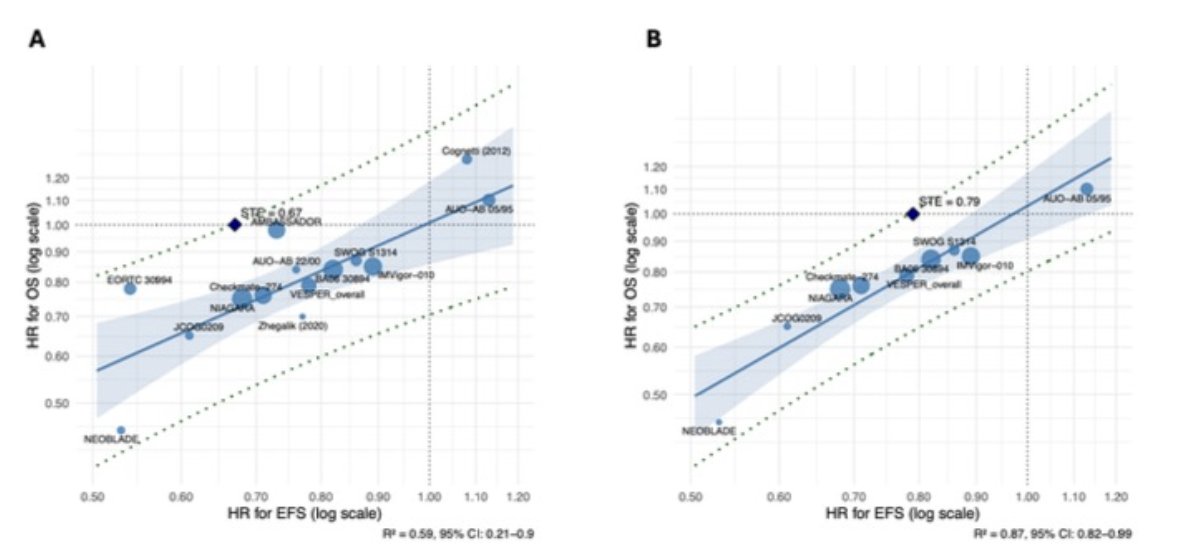
Event-free survival in the neoadjuvant setting met surrogacy criteria in both steps, with the correlation between treatment effect estimates of R2 = 0.87 and surrogate threshold effect = 0.73. Excluding high-risk-of-bias trials yielded R2 of 0.94 and a surrogate threshold effect of 0.76. While event-free survival did not meet surrogacy criteria in the overall analysis of adjuvant trials, a strong correlation was established in sensitivity analyses that excluded high-risk-of-bias trials and those permitting deferred chemotherapy (R2 = 0.95; surrogate threshold effect = 0.81). Neither pathological complete response (R2 = 0.42) nor pathological objective response met full surrogacy criteria, despite prognostic value in first-step analyses.
Dr. Scilipoti concluded his presentation discussing a study evaluating the surrogacy of intermediate clinical endpoints for overall survival after perioperative treatment in muscle-invasive bladder cancer patients undergoing radical cystectomy with the following take-home points:
- These findings support the use of event-free survival as a primary or co-primary endpoint in future perioperative muscle-invasive bladder cancer trials, potentially accelerating regulatory approval and patient access to effective therapies
- Although pathological complete response is prognostically informative, it does not meet formal trial-level surrogacy criteria for overall survival
- These findings do not support the use of pathological complete response as a stand-alone surrogate endpoint for designing or powering registrational neoadjuvant-based muscle-invasive bladder cancer trials
Presented by: Pietro Scilipoti, MD, Urologist, IRCCS Ospedale San Raffaele, Vita-Salute San Raffaele University, Milan, Italy
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the American Urological Association (AUA) 2026 Annual Meeting, Washington, DC, Fri, May 15 – Mon, May 18, 2026.