(UroToday.com) The American Urological Association's 2026 Annual Meeting, between May 15 – May 18, 2026 in Washington D.C., was host to the Interactive Poster (IP20): Bladder Cancer: Non-invasive II session. Dr. - Roger Li presented an interactive poster, IP20-12: Association of a Computational Histology AI (CHAI) Prognostic Biomarker with High Grade Recurrence Independent of Traditional Risk Factors in Low Grade Non-Muscle Invasive Bladder Cancer.
Dr. Li began his interactive poster presentation by highlighting that, according to current guidelines, low-grade NMIBC can be managed with a range of strategies, including active surveillance, intravesical chemotherapy, or BCG.1,2 However, a key clinical challenge remains identifying which patients are at risk for grade progression, as this can directly influence decisions regarding treatment initiation, escalation, or duration.
In this context, he introduced the Computational Histology AI (CHAI) platform, which has previously been used to develop prognostic biomarkers in high-grade NMIBC.3,4 Building on this work, the investigators applied the CHAI platform to develop and validate a novel biomarker using routine H&E slides aimed at predicting the risk of grade progression in patients with low-grade NMIBC.
To develop the biomarker, a pathologist selected representative diagnostic slides from low-grade NMIBC tumor specimens collected across multiple centers, resulting in a cohort of 783 cases. Digitized 40x whole-slide images were then analyzed using the CHAI platform, an artificial intelligence–based computational histology system previously developed for biomarker discovery in NMIBC.
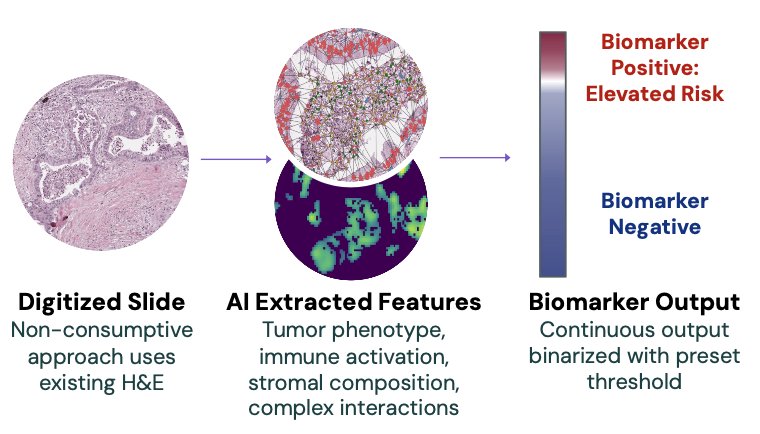
Feature data derived from the development cohort (n=275) that were most strongly associated with high-grade recurrence-free survival were incorporated into the low-grade biomarker model. Each tumor was assigned a continuous risk score, which was subsequently categorized into risk groups using a predefined 20% threshold established in the development cohort. The biomarker was then evaluated in an independent validation cohort (n=508), where its association with progression-free survival was assessed using a Cox proportional hazards model.
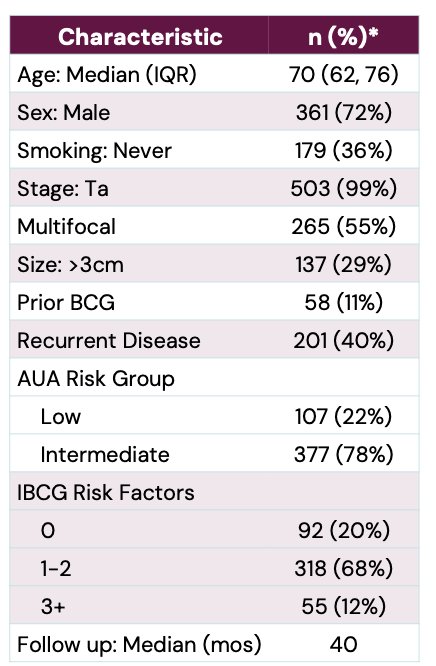
The validation cohort included 508 patients with predominantly Ta low-grade NMIBC. Median age was 70 years, and most patients were male (72%). Multifocal disease was present in 55% of patients, while 29% had tumors larger than 3 cm. Prior BCG exposure was reported in 11% of cases, and 40% of patients had recurrent disease at presentation. Most patients were classified as intermediate-risk according to AUA criteria (78%), with the remainder categorized as low risk. Using IBCG risk stratification, the majority of patients had 1–2 risk factors, while 12% had 3 or more risk factors. Median follow-up for the validation cohort was 40 months, as shown in the table below.
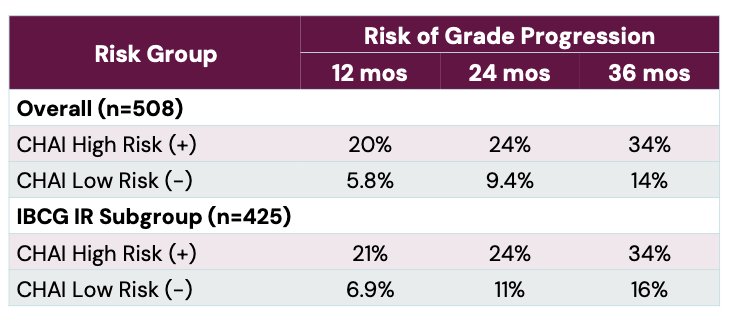
The CHAI low-grade biomarker successfully stratified patients according to risk of grade progression. Patients identified as CHAI biomarker–positive had a significantly higher risk of progression to higher-grade disease compared with biomarker-negative patients, with a hazard ratio of 3.06 (p<0.05).
At 36 months, the risk of grade progression reached 34% in the CHAI high-risk group compared with 14% in the low-risk group. Importantly, the prognostic value of the biomarker remained significant within the IBCG intermediate-risk subgroup, where CHAI-positive patients also demonstrated substantially higher progression risk (HR 2.65, p<0.05). These findings suggest that AI-driven histologic analysis may help identify low-grade NMIBC patients at greater risk for biologic progression despite otherwise favorable clinical features.
Dr. Li highlighted that the CHAI biomarker provided prognostic information independent of established clinicopathologic risk models. Even after accounting for traditional IBCG risk factors, CHAI biomarker risk groups remained independently associated with high-grade recurrence-free survival (HR 2.86, p<0.05).
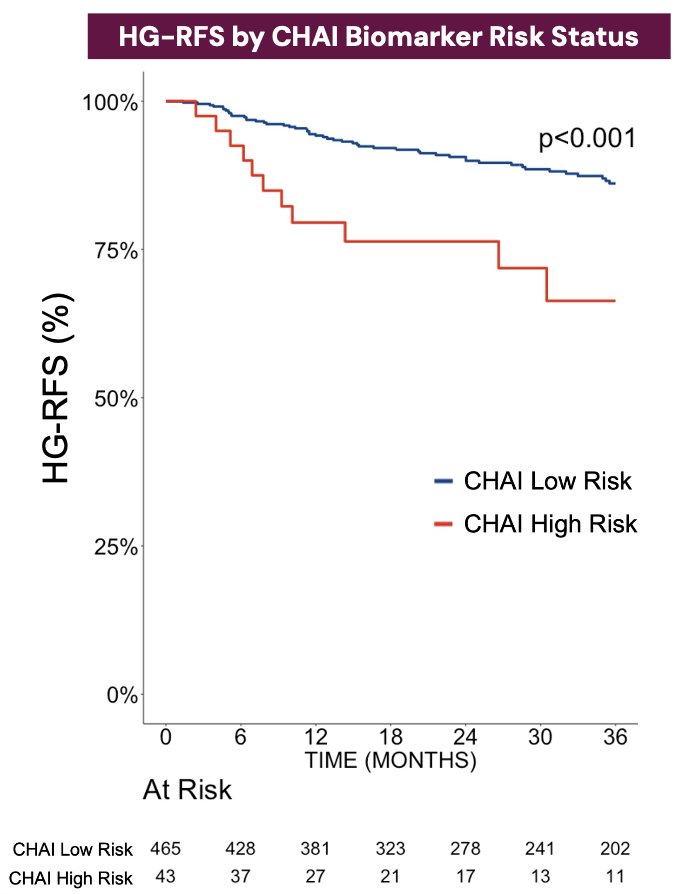
Lastly, Kaplan-Meier analysis demonstrated clear separation between CHAI high- and low-risk groups, with significantly worse HG-RFS observed among biomarker-positive patients (p<0.001). These findings suggest that AI-driven computational histology may capture biologic features of progression risk not fully reflected by conventional clinical and pathologic variables alone.
Dr. Li concluded with the following key points:
- Using routine pretreatment H&E tumor specimens, the CHAI low-grade biomarker identified a subset of LG NMIBC patients at substantially increased risk of grade progression
- CHAI biomarker–positive patients demonstrated a 34% risk of grade progression at 36 months, approaching rates typically observed in high-grade NMIBC
- The biomarker retained independent prognostic significance beyond established clinicopathologic and IBCG risk factors
- AI-driven computational histology may provide clinically meaningful biologic risk stratification not captured by conventional pathology alone
- The CHAI platform represents a potential precision medicine tool that could help identify patients with LG NMIBC who may benefit from treatment intensification or closer surveillance
Presented by: Roger Li, MD, Genitourinary Oncologist, Moffitt Cancer Center, Tampa, FL
Written by: Julian Chavarriaga, MD, Clinical Assistant Professor, Urologic Oncologist, Department of Urology at Penn State Health @chavarriagaj on Twitter during the American Urological Association's 2025 Annual Meeting, between May 15 – May 18, 2026, in Washington, D.C
Related content: Computational AI for Predicting Grade Progression in Intermediate-Risk Bladder Cancer - Roger Li
- Holzbeierlein J, et al. Management of low-grade non–muscle-invasive bladder cancer: contemporary considerations. J Urol. 2024;211(4):533–538.
- National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology: Bladder Cancer. Version 1.2026. Plymouth Meeting, PA: NCCN; 2026.
- Lotan Y, et al. Development and validation of computational histology biomarkers in non–muscle-invasive bladder cancer. J Urol. 2025;213(2):192–204.
- Chang SL, et al. Artificial intelligence and computational pathology in urothelial carcinoma: emerging clinical applications. Eur Urol. 2025;88(4):411–413.