(UroToday.com) The American Urological Association's 2026 Annual Meeting, in Washington D.C., was host to the Interactive Poster (IP20): Bladder Cancer: Non-invasive II session. Dr. Timothy Clinton presented interactive poster IP20-13: ADVANCED-2 (Cohort B): Interim Efficacy and Safety Data in BCG-Unresponsive Participants with High-Grade Non-Muscle Invasive Bladder Cancer (NMIBC).
Dr. Clinton began his presentation by emphasizing that, despite the emergence of several new therapies for BCG-unresponsive NMIBC, there remains a significant unmet clinical need for treatments that improve efficacy, durability of response, and tolerability while helping patients avoid radical cystectomy. He introduced TARA-002, a novel immunopotentiator and TLR2/NOD2 agonist derived from the Streptococcus pyogenes Su strain. Its proposed mechanism of action involves activation of both innate and adaptive immune pathways within the bladder microenvironment, aiming to enhance local antitumor immune responses.
From a practical standpoint, Dr. Clinton highlighted that TARA-002 may offer logistical advantages compared with other intravesical therapies. The agent does not require special handling or thawing and can be rapidly administered through a catheter in a standard office-based setting.
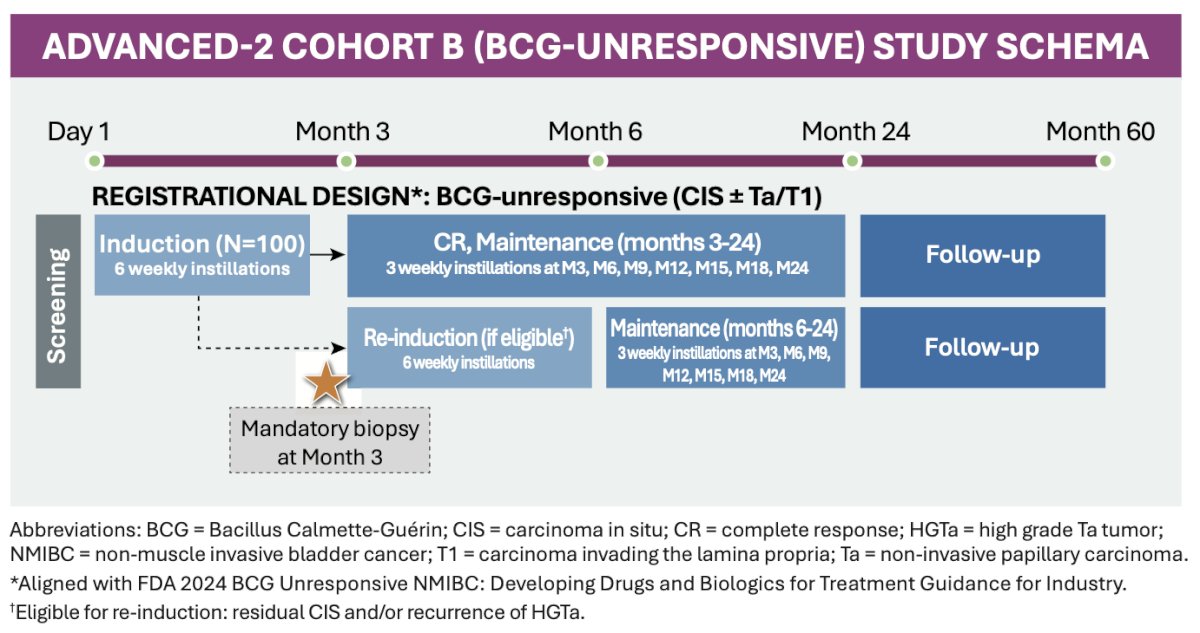
ADVANCED-2 (NCT05951179) Cohort B is an ongoing, open-label phase 2 study evaluating the safety and efficacy of intravesical TARA-002 in adults with BCG-unresponsive high-grade NMIBC with CIS ± Ta/T1 disease. Eligible patients included those previously treated with BCG and non-BCG therapies, including prior investigational agents. The primary endpoint was centrally reviewed high-grade complete response at any time, while a key secondary endpoint was duration of response at 12 months. The data cutoff for the presented analysis was January 28, 2026.
As outlined in the study schema, patients initially received a 6-week induction course of weekly intravesical TARA-002 instillations. A mandatory biopsy was performed at month 3 to assess response. Patients achieving a complete response proceeded to a maintenance phase consisting of 3 weekly instillations administered at months 3, 6, 9, 12, 15, 18, and 24, followed by long-term follow-up through 60 months. Patients with residual CIS and/or recurrent high-grade Ta disease were eligible for re-induction with an additional 6 weekly instillations before resuming maintenance therapy.
Dr Clinton noted that the presented dataset included 43 patients with BCG-unresponsive NMIBC, with a median age of 75 years (range 47–92 years). Most participants were male (72%) and White (81%). Importantly, the study population reflected a heavily pretreated cohort, including patients previously exposed to BCG, non-BCG intravesical therapies, and investigational agents.
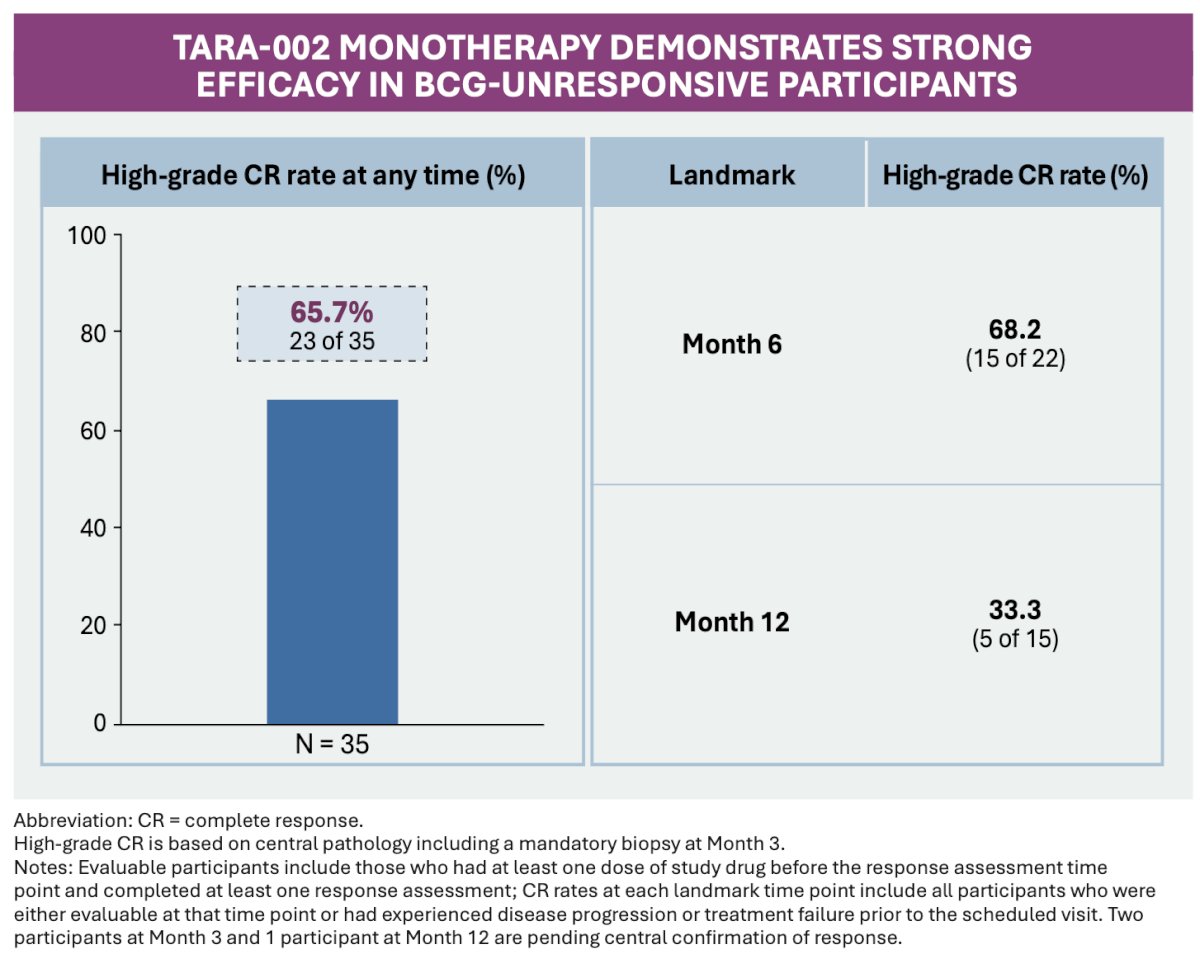
Efficacy results demonstrated encouraging activity with intravesical TARA-002. The high-grade complete response rate at any time was 65.7% among evaluable patients. At predefined time points, the high-grade CR rate was 68.2% at 6 months and 33.3% at 12 months, suggesting durable responses in a subset of patients with BCG-unresponsive disease.
Durability of response appeared encouraging among initial responders. All evaluable patients who achieved an initial complete response maintained their response through month 6, while 80% remained disease-free through month 9, and all evaluable patients maintained response through month 12.
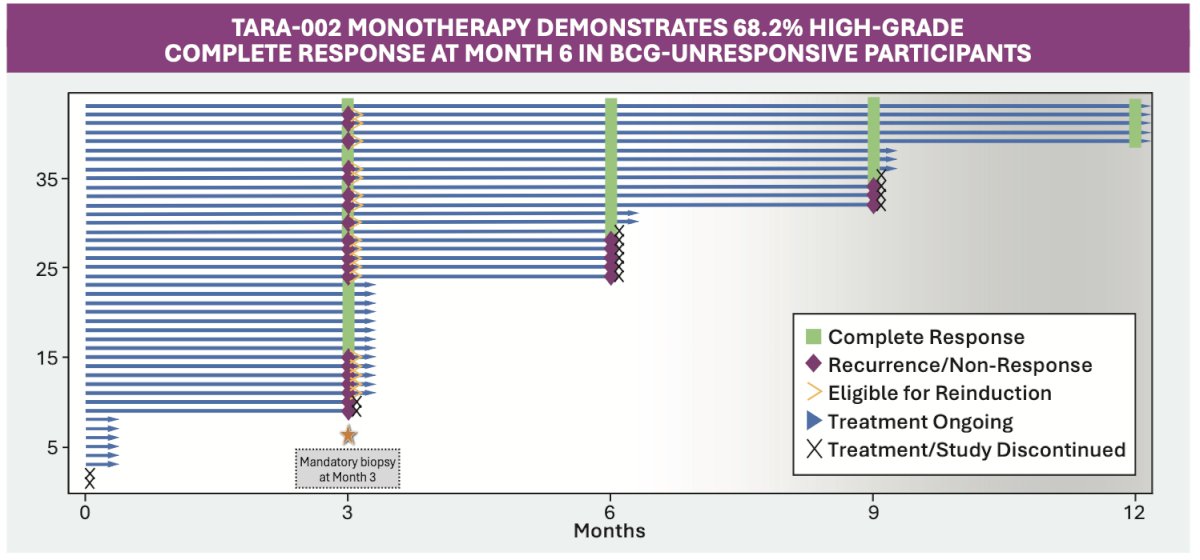
Importantly, Dr. Clinton also highlighted the activity observed with re-induction therapy. Among patients who did not initially respond and subsequently underwent re-induction with TARA-002, 61.5% converted to a complete response by month 6. Among these delayed responders, durability also appeared favorable, with most maintaining response through month 9 and all evaluable patients remaining in complete response through month 12. These findings suggest that re-induction may provide an additional therapeutic opportunity for selected patients with initially resistant disease.
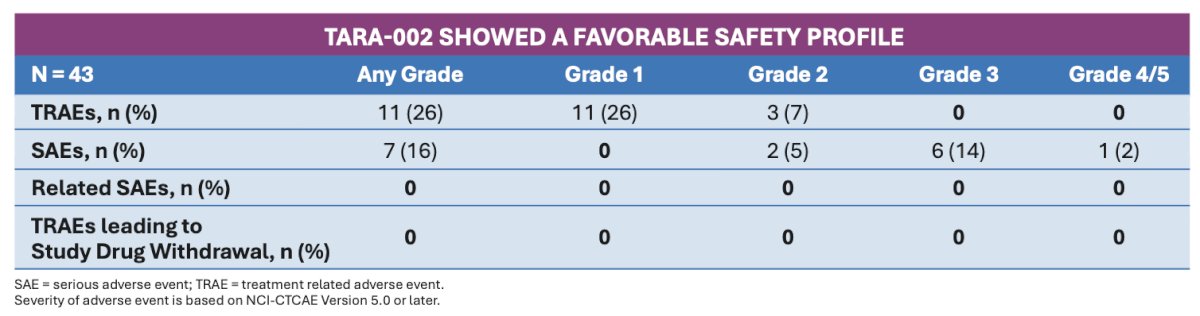
From a safety standpoint, TARA-002 demonstrated a favorable tolerability profile. Treatment-related adverse events were predominantly low grade and transient, with the most commonly reported events including dysuria, bladder spasms, and urinary urgency. Importantly, no patients experienced grade ≥3 treatment-related adverse events, treatment-related serious adverse events, or adverse events leading to treatment discontinuation. These findings support the feasibility of office-based intravesical administration and suggest that TARA-002 may offer a manageable safety profile in this heavily pretreated BCG-unresponsive population.
Dr. Clinton concluded by highlighting several future directions for research:
- In patients with BCG-unresponsive high-grade NMIBC with CIS ± Ta/T1 disease, intravesical TARA-002 demonstrated encouraging clinical activity with a favorable tolerability profile
- The observed efficacy and safety findings support the continued accrual and ongoing evaluation of the ADVANCED-2 study
- Re-induction therapy appeared to successfully salvage a substantial proportion of initial non-responders, leading to meaningful conversion rates to complete response
- Responses following re-induction also appeared durable, supporting further investigation of adaptive treatment strategies with TARA-002 in BCG-unresponsive disease
Presented by: Timothy Clinton, MD, Associate Surgeon, Assistant Professor, Department of Urology, Brigham and Women’s Hospital, Boston, MA
Written by: Julian Chavarriaga, MD, Clinical Assistant Professor, Urologic Oncologist, Department of Urology at Penn State Health @chavarriagaj on Twitter during the American Urological Association (AUA) 2026 Annual Meeting, Washington, DC, Fri, May 15 – Mon, May 18, 2026.