(UroToday.com) The American Urological Association's 2026 Annual Meeting, between May 15 – May 18, 2026 in Washington D.C., was host to the Interactive Poster (IP20): Bladder Cancer: Non-invasive II session. Dr. Takumi Okazaki presented an interactive poster, IP20-07: Improved Outcomes in High-Risk Non-Muscle Invasive Bladder Cancer with Oral 5- Aminolevulinic Acid Fluorescence Cystoscopy–Assisted Transurethral Resection of Bladder Tumors.
Dr. Okazaki began by highlighting that fluorescence cystoscopy using oral 5-aminolevulinic acid improves the visualization of malignant urothelial lesions and has been shown to reduce intravesical recurrence compared with standard white-light cystoscopy. However, its impact on disease progression in patients with NMIBC undergoing TURBT remains less well defined. In this context, the study they presented today aimed to evaluate risk migration based on fluorescence findings compared with white-light cystoscopy and to assess differences in intravesical recurrence and disease progression among patients undergoing TURBT with and without fluorescence guidance for primary NMIBC.
This was a single-center study including patients who underwent initial TURBT for primary bladder cancer between 2019 and 2024. After excluding patients with muscle-invasive disease, prior upper tract urothelial carcinoma, non-urothelial histology, use of narrow-band imaging, incomplete TURBT, or bladder involvement from prostate cancer, a total of 240 patients with primary NMIBC were included in the analysis as illustrated below.
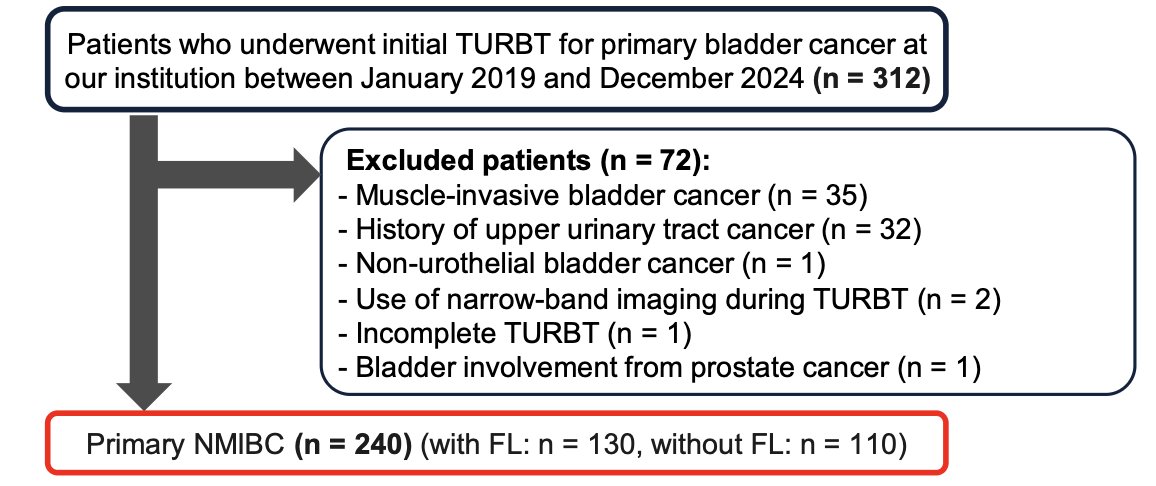
Among these 240 patients, 130 patients underwent fluorescence-guided TURBT and 110 underwent standard white-light TURBT. In the fluorescence group, oral ALA was administered 2–8 hours prior to surgery. Fluorescence-guided TURBT had been implemented at the institution since 2018 and was used in most patients, except those with significant cardiovascular comorbidities.
From a methodological standpoint, fluorescence findings were prospectively recorded and analyzed separately from white-light findings during TURBT. The study evaluated the impact of fluorescence cystoscopy on tumor detection and risk stratification using the CUETO model for recurrence and progression. Oncologic outcomes included intravesical recurrence-free survival and progression-free survival, which were compared between the fluorescence and white-light groups based on CUETO risk classification derived from white-light findings.
Baseline characteristics were similar between the fluorescence-guided and white-light groups. Median age was similar at 74 years in both cohorts, and the majority of patients were male. Tumor size and the presence of concomitant CIS were also balanced between groups. There was a trend toward a higher proportion of multiple tumors in the fluorescence group, while single tumors were more common in the white-light group. Pathologically, the fluorescence group had a higher proportion of high-grade tumors (70% vs 56%), with similar distributions of T stage. Based on CUETO classification using white-light findings, recurrence risk categories were comparable between groups as shown in the table below.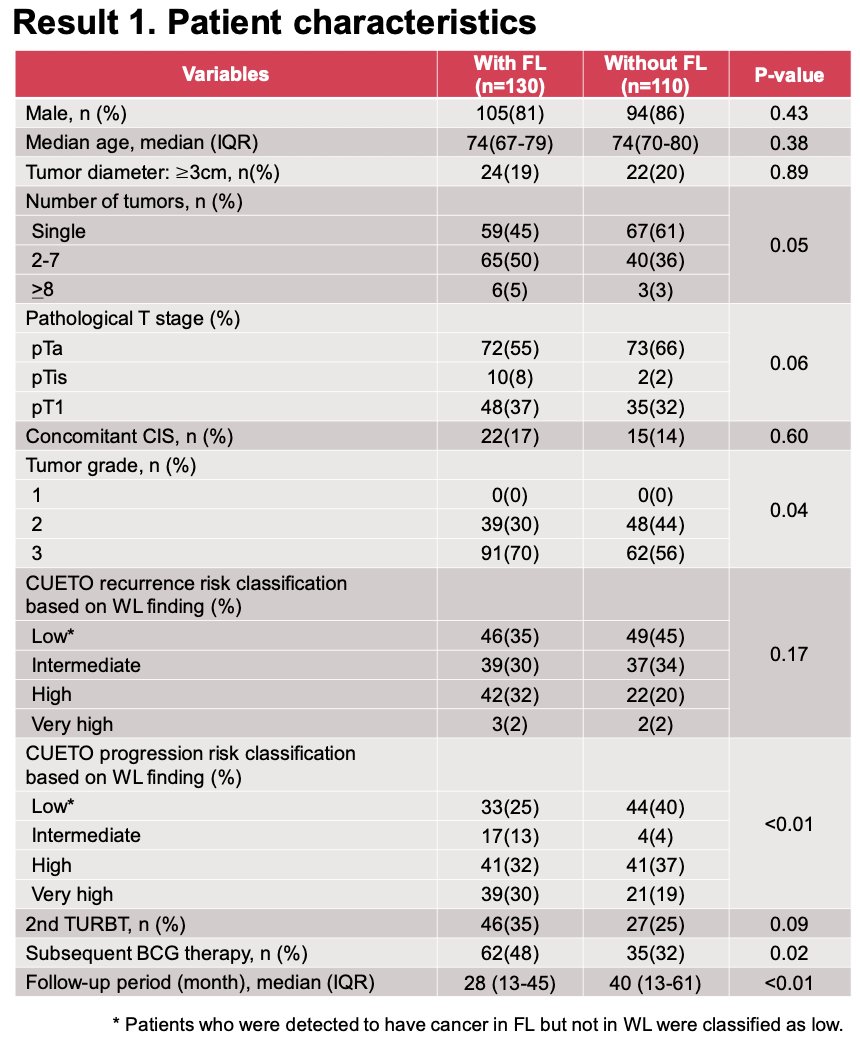
Notably, Fluorescence cystoscopy led to meaningful risk reclassification compared with white-light findings alone. Additional tumor-positive specimens detected exclusively with fluorescence resulted in changes in CUETO risk categories, including both recurrence and progression risk. In several cases, patients initially classified as low risk based on white-light cystoscopy were upstaged to intermediate or high-risk groups after incorporation of fluorescence findings, driven by detection of additional lesions such as CIS or higher-grade disease.
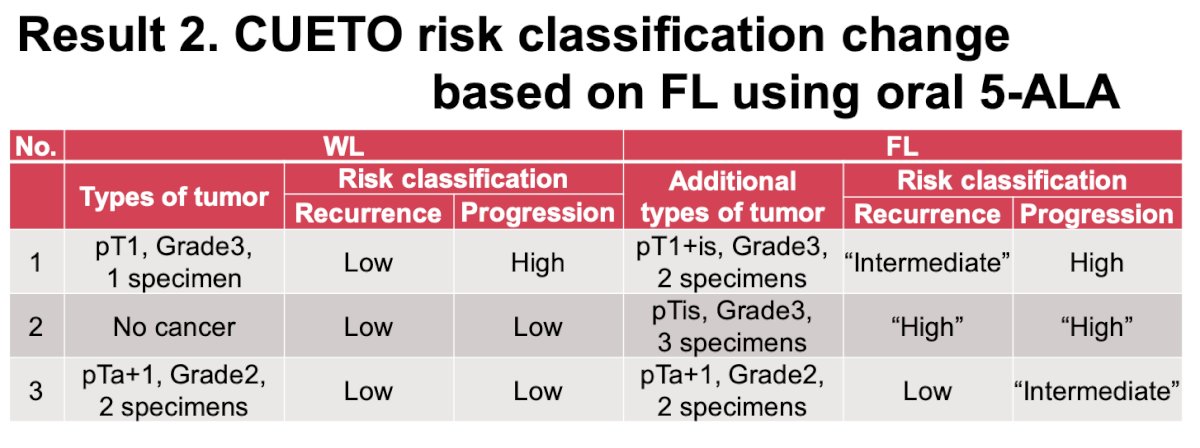
Overall, 11 patients had additional tumor-positive specimens identified only with fluorescence cystoscopy. This translated into upgraded CUETO risk classification for a subset of patients, with approximately 2% reclassified to higher risk categories for both recurrence and progression. These findings highlight the potential of fluorescence-guided TURBT to improve risk stratification by identifying otherwise occult disease.
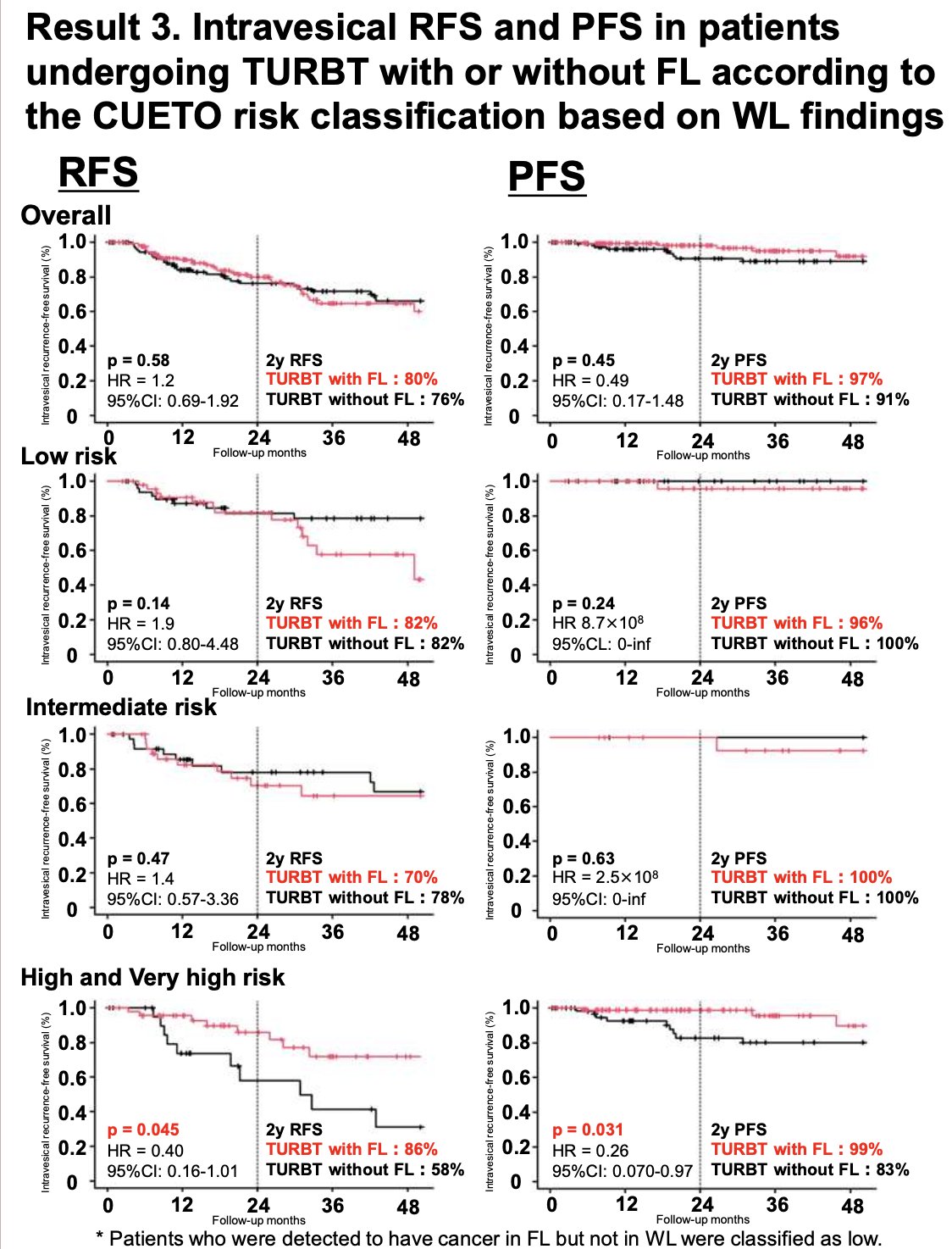
Moreover, the addition of fluorescence cystoscopy did not significantly impact recurrence-free or progression-free survival in the overall cohort. Two-year RFS and PFS rates were similar between groups, with no statistically significant differences observed across low- and intermediate-risk patients based on CUETO classification. However, in patients with high- and very high-risk disease, fluorescence-guided TURBT was associated with improved outcomes. Two-year RFS was higher in the fluorescence group (86% vs 58%), with a corresponding reduction in recurrence risk. Similarly, two-year PFS favored the fluorescence arm (99% vs 83%), reaching statistical significance. These findings suggest that the benefit of fluorescence cystoscopy may be most pronounced in higher-risk NMIBC, where improved tumor detection and resection may translate into meaningful oncologic gains.
Dr. Okazaki concluded with the following key points:
- Fluorescence cystoscopy findings led to upgraded CUETO risk classification for both recurrence and progression in a small subset of patients (approximately 2% each)
- The addition of fluorescence using oral 5-ALA improved risk stratification by identifying otherwise occult disease
- Use of fluorescence-guided TURBT was associated with improved RFS and PFS in patients with high- and very high-risk NMIBC
- These findings suggest that the clinical benefit of fluorescence cystoscopy may be most relevant in higher-risk patient populations
Presented by: Takumi Okazaki, MD, Department of Urology, Institute of Science Tokyo, Tokyo, Japan.
Written by: Julian Chavarriaga, MD, Clinical Assistant Professor, Urologic Oncologist, Department of Urology at Penn State Health @chavarriagaj on Twitter during the American Urological Association's 2025 Annual Meeting, between May 15 – May 18, 2026, in Washington, D.C