(UroToday.com) The American Urological Association's 2026 Annual Meeting, between May 15 and May 18, 2026, in Washington, D.C., was host to the Interactive Poster (IP20): Bladder Cancer: Non-invasive II session. Dr. Mark Tyson presented interactive poster IP20-24: Blue Light Cystoscopy Enables Earlier CIS Recognition and Can Guide Risk-Appropriate Management of High-Risk Non–Muscle-Invasive Bladder Cancer: Real-World Outcomes from a U.S. Claims Cohort.
Dr. Tyson began by highlighting that bladder cancer remains among the 10 most commonly diagnosed cancers worldwide, with approximately 75% of patients presenting with NMIBC.1 Although survival outcomes are generally favorable, disease management often involves prolonged surveillance and repeated interventions, contributing to reduced quality of life and making bladder cancer one of the most costly malignancies to treat.1 He noted that both Blue Light Cystoscopy (BLC®) and White Light Cystoscopy (WLC) are commonly used in the diagnosis and surveillance of NMIBC, though comparative real-world outcomes between these approaches remain incompletely understood. Importantly, BLC may improve the detection of CIS and other high-grade flat lesions that are often missed under white light evaluation.
In this study, the investigators evaluated whether BLC improves early identification of CIS and other high-risk disease features in real-world practice and whether this influences downstream clinical management. While no statistically significant differences were observed in recurrence or progression outcomes in initial analyses, trends suggested higher recurrence rates in the BLC cohort, possibly reflecting improved detection of occult disease. Additionally, fewer therapy changes and radiation-related procedures were observed following index cystoscopy in the BLC group, supporting the need for further evaluation of the clinical impact of BLC-guided management strategies.
The investigators performed a retrospective real-world analysis of patients with bladder cancer undergoing either BLC or standard WLC between 2011 and 2023 using the Optum Research Database. Overall, 794 patients treated with BLC were compared with a matched cohort of 4,764 patients who underwent WLC. To reduce baseline differences between groups, the analysis incorporated 1:6 matching and inverse probability of treatment weighting (IPTW), accounting for demographic characteristics, comorbidities, and prior bladder cancer treatments, including previous BCG exposure.
Inclusion criteria included the following:
- Patients who underwent either more than one or at least one BLC or WLC between June 1, 2011, and May 31, 2023. The index date was defined as the earliest BLC procedure, while patients in the WLC cohort were matched 6:1 based on year of service and time from cystoscopy to bladder cancer diagnosis. Patients in the WLC cohort had no prior evidence of BLC exposure
- A diagnosis of bladder cancer is defined by at least two non-diagnostic medical claims on separate dates between January 1, 2011, and November 30, 2023, with the earliest claim considered the diagnosis date
- Continuous enrollment with both medical and pharmacy coverage for at least 24 months prior to index cystoscopy and a minimum of 6 months of follow-up afterward
Exclusion criteria included:
- Evidence of participation in a clinical trial at any point during the study period
- Pregnancy during the study period
- Age <18 years at the time of cystoscopy or missing demographic data, including gender, insurance type, or geographic region
Dr Tyson highlighted that all patients were required to have continuous enrollment for at least 6 months prior to index cystoscopy and a minimum of 6 months of follow-up. Follow-up continued until disenrollment, death, or the end of the study period (November 30, 2023), whichever occurred first. Mean follow-up was 734 days in the BLC cohort and 770 days in the WLC cohort.
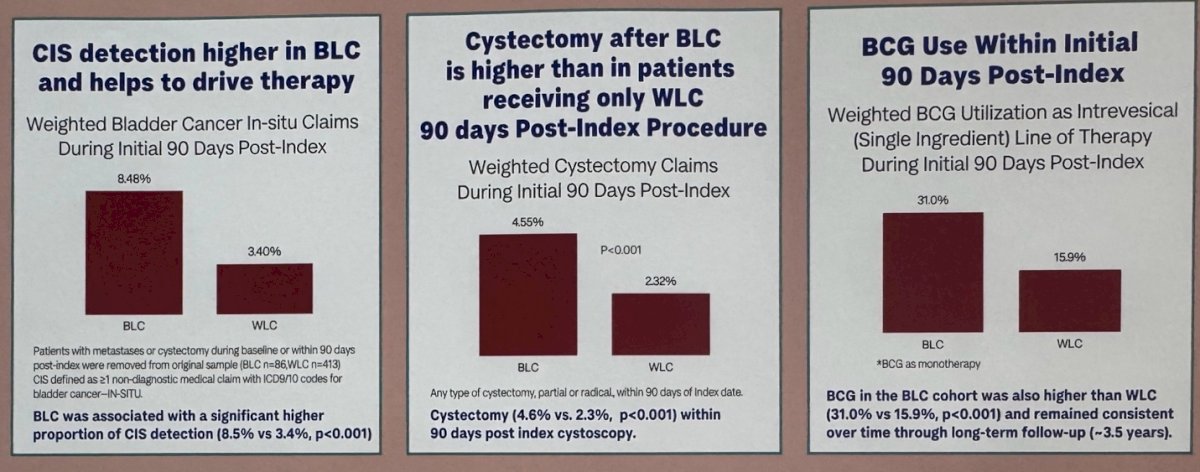
Notably, the use of BLC was associated with significantly higher detection of CIS during the first 90 days following index cystoscopy compared with WLC alone (8.5% versus 3.4%, p<0.001). Dr. Tyson highlighted that improved identification of occult high-risk disease may help explain differences in downstream management observed between cohorts.
Patients treated with BLC were also more likely to receive intravesical BCG within 90 days of index cystoscopy (31.0% versus 19.9%), with this trend persisting throughout longer-term follow-up. Additionally, early cystectomy rates were higher in the BLC cohort compared with WLC (4.0% versus 2.3%, p<0.001), as illustrated in the graphics below.
Consistent with earlier findings, time-to-BCG initiation remained higher in the BLC cohort throughout follow-up. Dr. Tyson highlighted that the difference in BCG utilization between groups persisted over time, extending to approximately 3.5 years following index cystoscopy. These findings further support the notion that improved detection of high-risk disease with BLC may influence long-term treatment patterns and subsequent clinical management.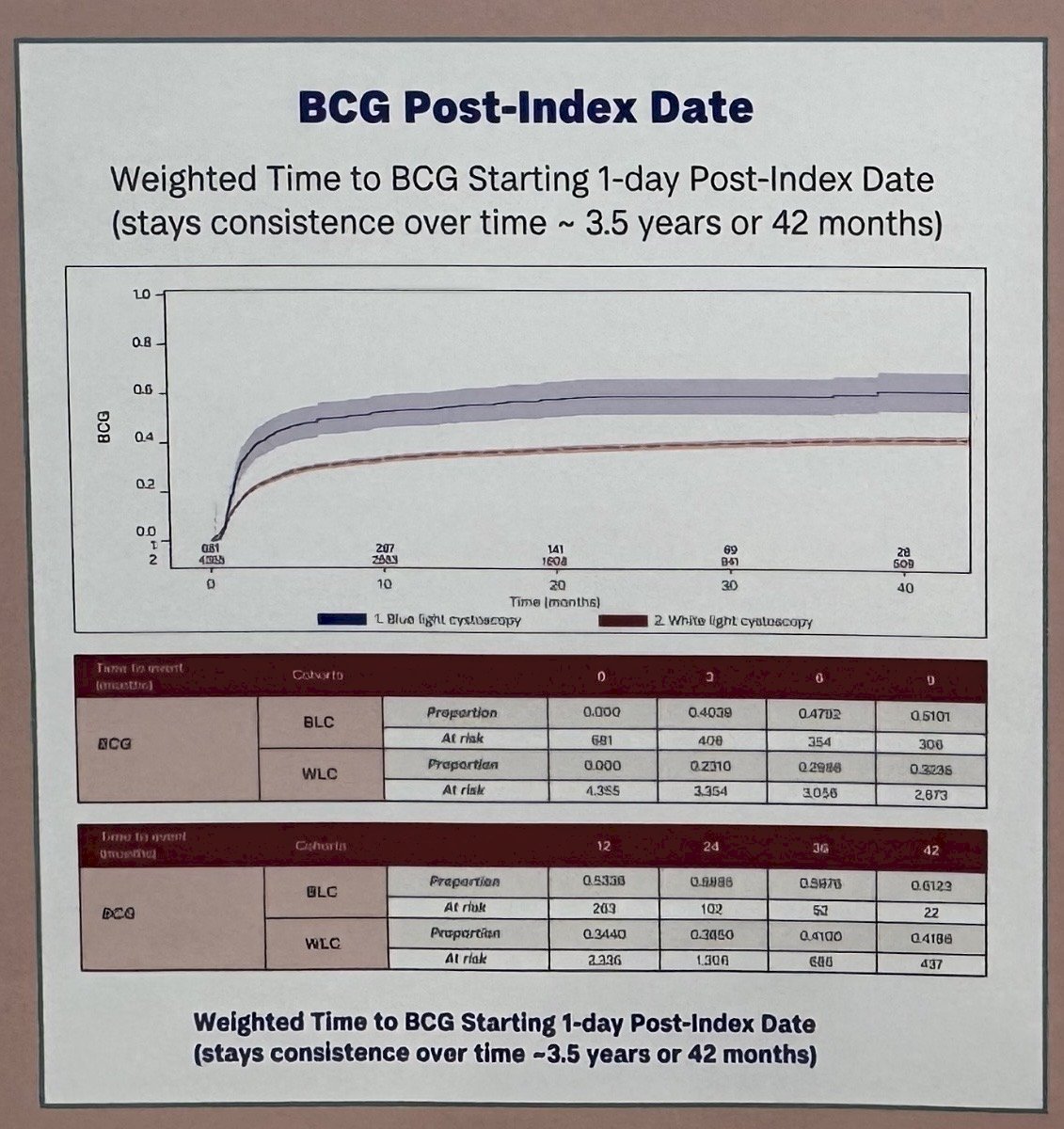
Lastly, on adjusted Cox proportional hazards analysis, patients undergoing BLC demonstrated significantly higher rates of both CIS detection and cystectomy within 90 days of index cystoscopy compared with those treated with WLC alone. The hazard ratio for CIS detection was 2.13 (95% CI 1.46–3.11), while the hazard ratio for cystectomy was 1.66 (95% CI 1.21–2.28).
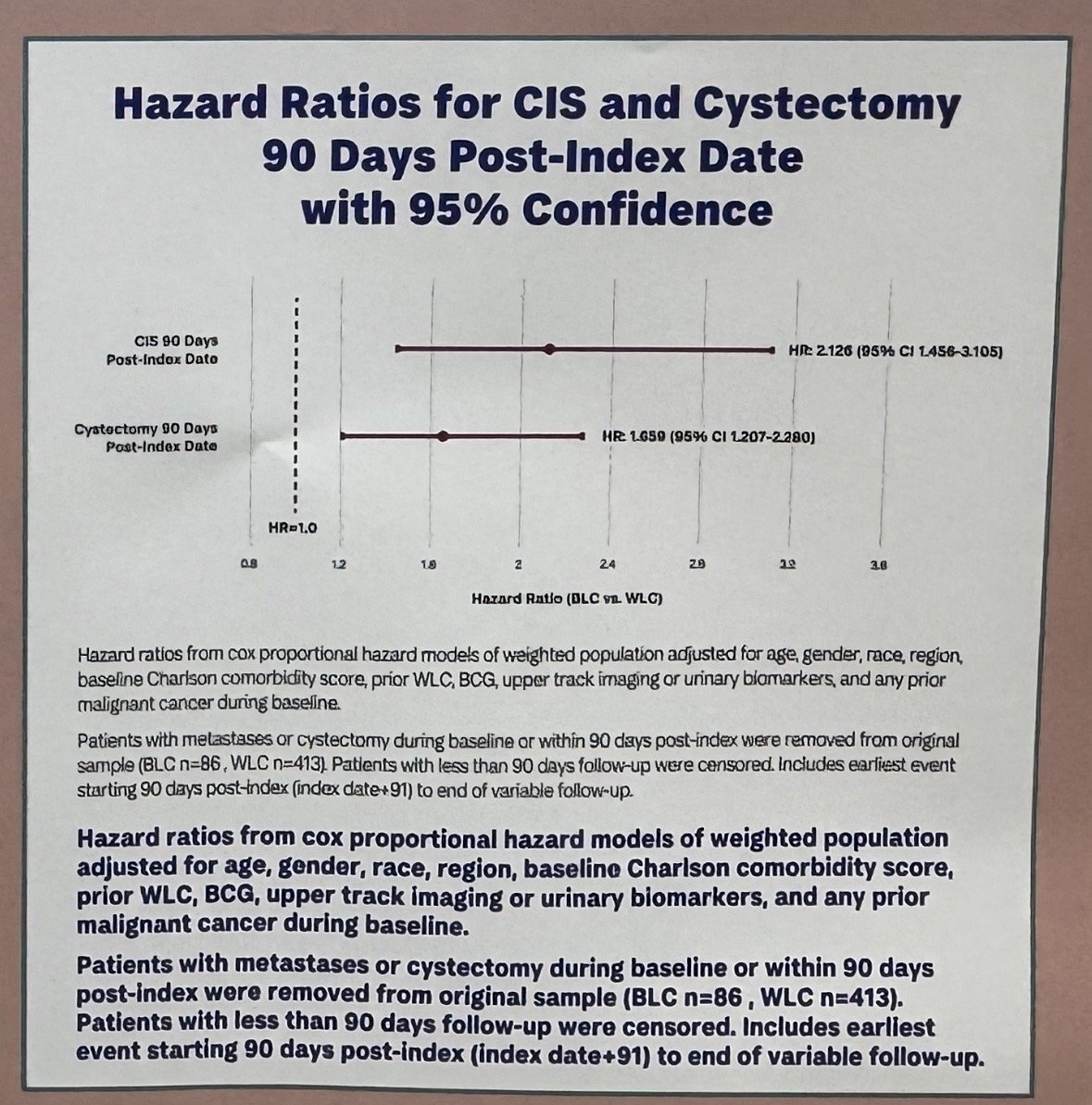
These analyses were adjusted for multiple baseline factors, including demographics, comorbidity burden, prior BCG exposure, prior WLC, upper tract imaging, urinary biomarkers, and history of malignancy. Dr. Tyson noted that these findings further support the potential role of BLC in improving the identification of higher-risk disease that may warrant earlier treatment escalation.
Dr. Tyson concluded his presentation with the following key points:
- BLC demonstrated durable diagnostic sensitivity for CIS and was associated with higher rates of BCG utilization and earlier treatment initiation
- Patients undergoing BLC were more likely to receive BCG and undergo earlier cystectomy, suggesting improved identification of higher-risk disease
- BLC may serve as a triage tool, helping identify patients who may benefit from bladder-sparing approaches while directing truly high-risk patients toward earlier definitive treatment
- These findings support both the clinical and economic rationale for broader adoption of BLC in real-world practice, particularly as newer bladder-sparing therapies continue to emerge
Presented by: Mark Tyson II, MD, MPH, Urologic Oncologist, Mayo Clinic, Scottsdale, AZ
Written by: Julian Chavarriaga, MD, Clinical Assistant Professor, Urologic Oncologist, Department of Urology at Penn State Health @chavarriagaj on Twitter during the American Urological Association's 2025 Annual Meeting, between May 15 – May 18, 2026, in Washington, D.C
Related content: Retrospective Cohort Analysis of Blue-Light Cystoscopy Using a Claims Database - Mark Tyson
Reference: