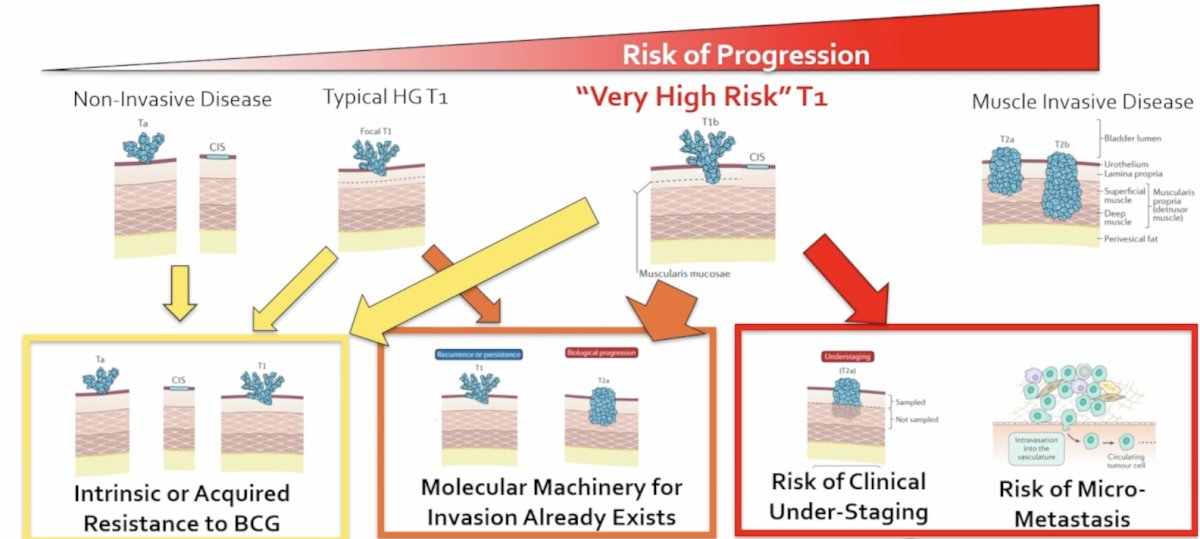
(UroToday.com) The 2026 AUA annual meeting featured practice-changing, paradigm-shifting clinical trials in urology and a presentation by Dr. Eugene Pietzak discussing intravenous pembrolizumab combined with intravesical BCG for patients with BCG-naïve very high risk T1 non muscle invasive bladder cancer. Dr. Pietzak notes that high grade non muscle invasive bladder cancer is not one homogeneous disease, with several factors suggesting patients are “very high risk” T1 disease: (i) intrinsic or acquired resistance to BCG, (ii) molecular machinery for invasion already exists, and (iii) risk of clinical understaging/risk of micrometastatic disease:
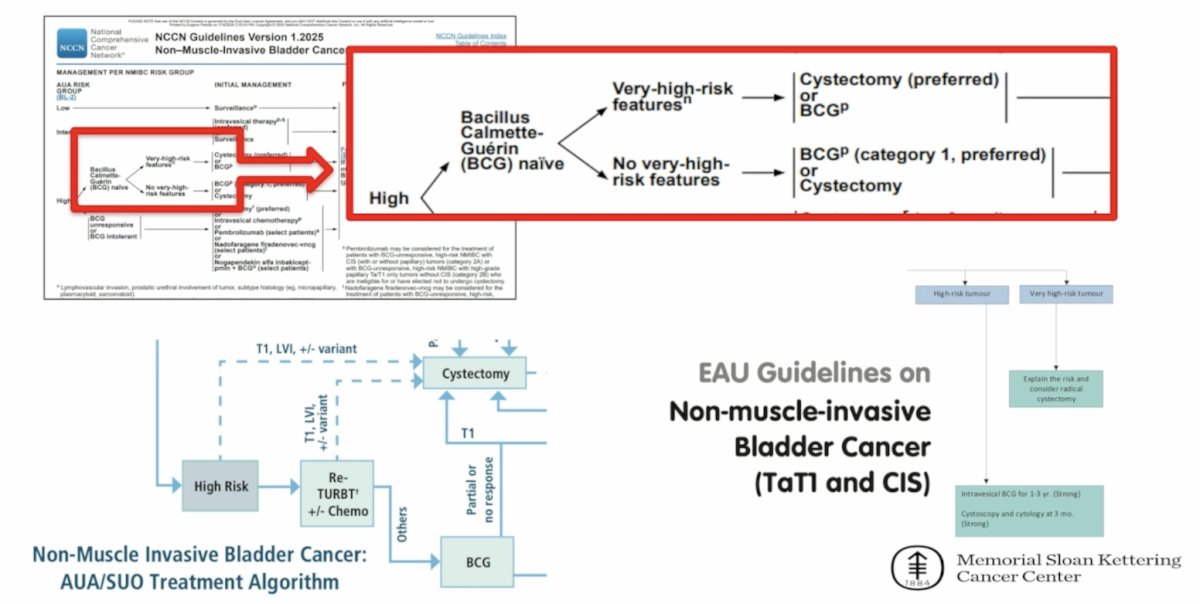
Across the NCCN, AUA, and EAU guidelines, the recommendation for these very high risk T1 patients is to undergo radical cystectomy:
However, the choice of radical cystectomy is difficult for very high risk T1 non muscle invasive bladder cancer patients, given that upfront cystectomy is over treatment for ~50-75% of patients and BCG alone is under treatment for ~25-50% of patients. Thus, there is a major unmet need for patients with very high risk T1 disease, and we need different approaches to balance under versus over treatment.
The rationale for adding an anti-PD1/PDL1 to BCG is that PD1/PDL1 may be a mechanism of resistance to BCG, especially for “very high risk” T1 + CIS non muscle invasive disease. Additionally, immune checkpoint blockade alone has minimal efficacy after BCG, but with possible synergism for anti-PD1/PDL1 + BCG. Generally, there is a suboptimal benefit to risk ratio for immune checkpoint blockade + BCG for most patients with non muscle invasive bladder cancer, but the role for adding immune checkpoint blockade to BCG remains undefined for patients with very high risk T1 + CIS:
The objective of this investigator initiated study presented at the 2026 AUA annual meeting was to define the role of adding immune checkpoint blockade to BCG for very high risk T1 + CIS.
This is a single arm, phase II, investigator initiated trial of intravenous pembrolizumab + intravesical BCG in patients with BCG-naïve very high risk T1 non muscle invasive bladder cancer (data cutoff January 24, 2026; median follow-up 22 months; follow-up is still ongoing). The key inclusion criteria for this trial are as follows:
- BCG-naïve (no prior BCG)
- Histologic confirmed high grade T1N0M0 urothelial bladder cancer
- Histologic confirmed concomitant CIS
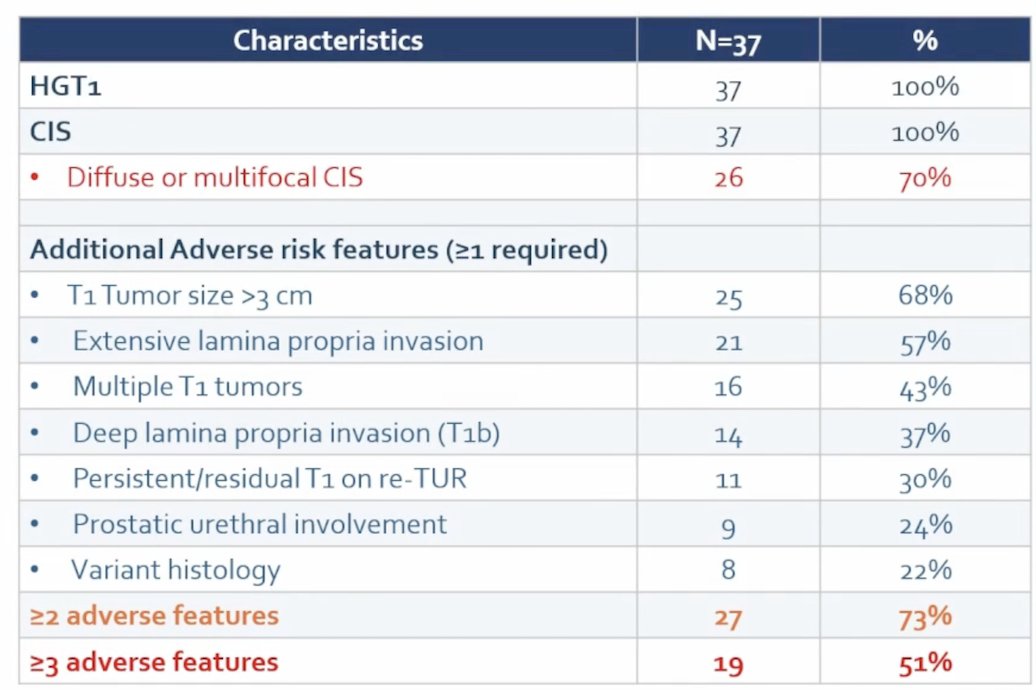
- ≥1 additional adverse feature associated with risk of progression:
- Persistent T1 disease on restaging TURBT
- Recurrent T1 disease (without prior BCG)
- Multiple T1 tumors
- T1b disease (deep/extensive lamina propria invasion)
- T1 tumor size ≥3 cm
- Urothelial carcinoma with variant histologic subtypes
- Urothelial carcinoma involving the prostatic urethra (Ta, Tis, or T1)
- Lymphovascular invasion
- All patients were recommended to undergo immediate radical cystectomy but declined surgery
The key exclusion criteria include:
- Any prior intravesical BCG
- Any prior immune checkpoint inhibitors or other T cell–directed agents
- Pure squamous carcinoma, pure adenocarcinoma, or any small cell/neuroendocrine
- History of muscle-invasive bladder cancer or prostatic stromal invasion
- Prior radiation therapy for bladder cancer
- Radiation for prostate and other pelvic radiation was allowed
- Patients with active autoimmune disease requiring systemic treatment
- Immunodeficiency, active hepatitis B or C infection, or the need for systemic immunosuppression
- Glomerular filtration rate <30 mL/min
- Absolute contraindication to BCG
A re-TURBT and examination under anesthesia at Memorial Sloan Kettering Cancer Center (MSKCC) were required within 8 weeks of study entry. Treatments included intravenous pembrolizumab 400 mg every 6 weeks for up to 9 doses (48 weeks) and intravesical BCG (TICE strain, 50 mg). Induction BCG began 3 weeks after the first dose of pembrolizumab, with SWOG style maintenance BCG given at 3, 6, and 12 months. Additional maintenance was permitted, if available, given the global shortage:

Treatment assessments included the following:
- Cystoscopy and urine cytology at 3, 6, 9, and 12 months from start of treatment
- Biopsy/TURBT was performed only for cause
- All patients with baseline prostatic urethral involvement were recommended post- treatment biopsies/TURP
- Narrow band imaging was routinely used at TURBT and surveillance
- cystoscopies
- Biopsy/TURBT was performed only for cause
- CT/MR urogram were performed at baseline, 12 months, and as clinically indicated
- Patients with CIS or HG Ta at 3 months were allowed to stay on study with maintenance BCG
- ≥T1 at 3 months or any time point was treatment failure
- Any high grade recurrence at or beyond 6 months was treatment failure
- Low grade Ta recurrences were recorded but not considered treatment failure
With regards to statistical considerations, Dr. Pietzak noted that the primary outcome is 6 month clinical complete response (by cystoscopy/cytology), with a Simon’s minimax two-stage design, and a null hypothesis that complete response rate ≤50% would not be worthy of further investigation. Historically, there have been poor outcomes with BCG alone for HGT1 with CIS + additional adverse feature. The alternative hypothesis is that a ≥70% clinical complete response would be clinically meaningful.
The planned sample size was 37 patients, with ≥13 of 23 patients needing a clinical complete response in the first stage, and ≥24 of 37 patients needing a clinical complete response to reject the null hypothesis. This design provided 80% power with a one-sided type I error rate of 5%. Secondary endpoints included recurrence free survival, cystectomy free survival, and safety, with a post hoc analysis of bladder intact disease free survival.
There were 43 patients assessed for eligibility and 37 patients enrolled with a median age of 67 years (range: 34-86), 86% male, and 84% White:
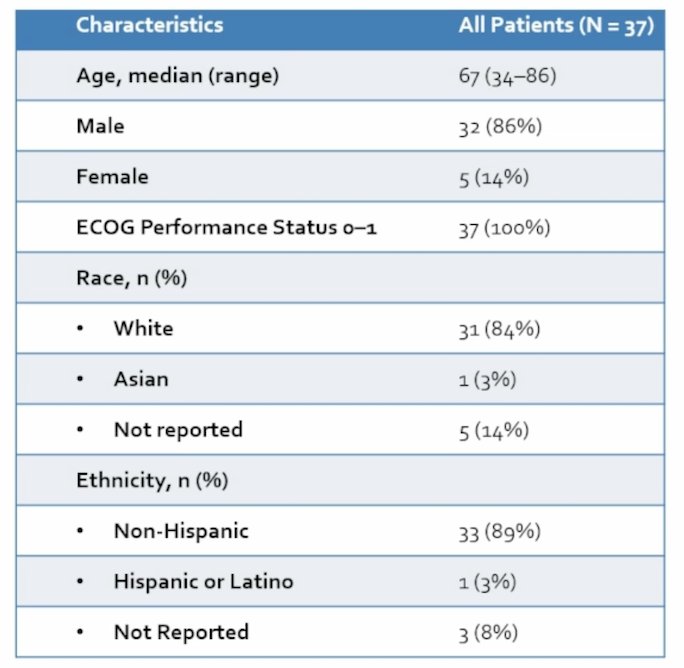
Clinicopathologic features of this very high risk T1 cohort are highlighted in the following table:
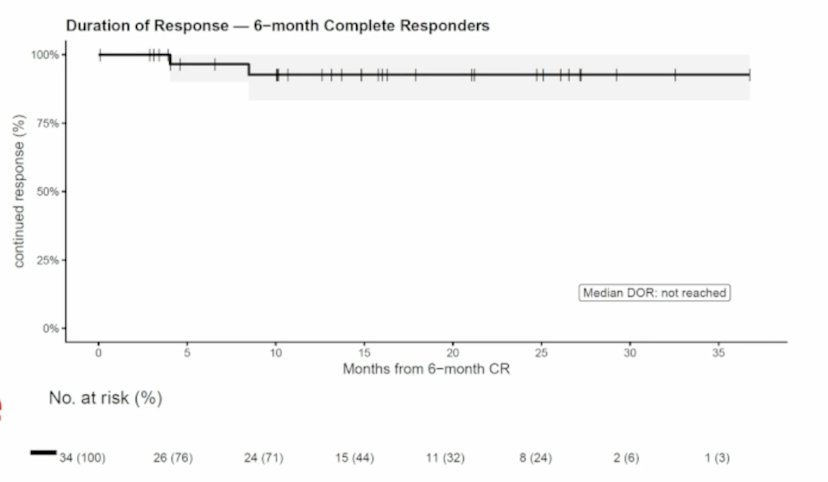
The trial met its primary endpoint, exceeding the pre-specified ≥70% clinical complete response rate with a 92% complete response rate (34 of 37 patients) at 6 months:
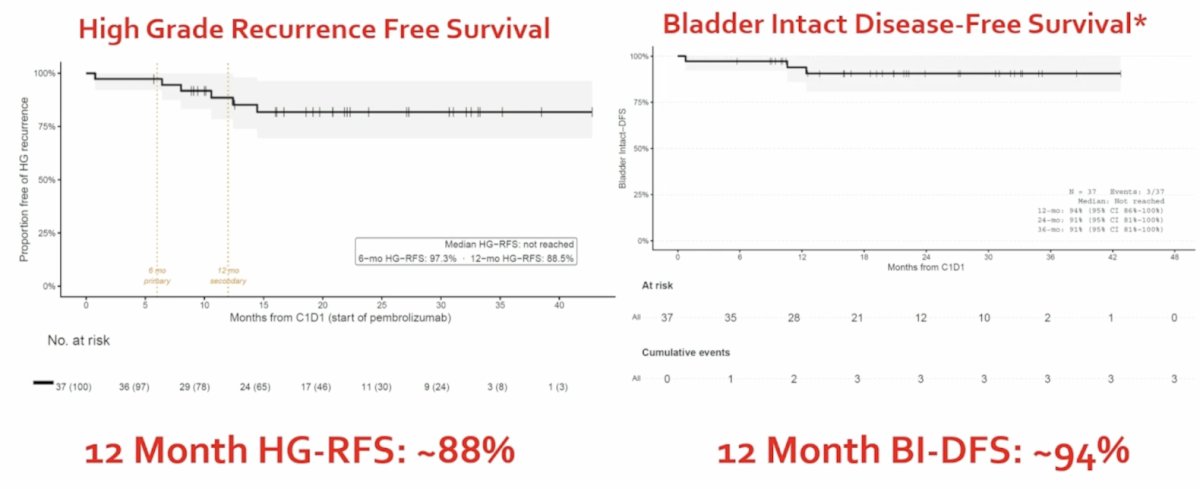
At a median follow-up of 22 months, no patients progressed to muscle invasive bladder cancer or metastasis. There were 4 (11%) patients with high grade recurrence (2 with recurrent HG T1, 1 with CIS, 1 with prostatic urethral CIS), and 2 (5%) patients underwent radical cystectomy (1 for recurrent HG T1 – final path pTisN0; 1 for pubovesical fistula secondary to prior RP/RT – final path pT0N0). The 12 month high grade recurrence free survival rate was 88%, and the 12 month bladder intact disease free survival rate was 94%:
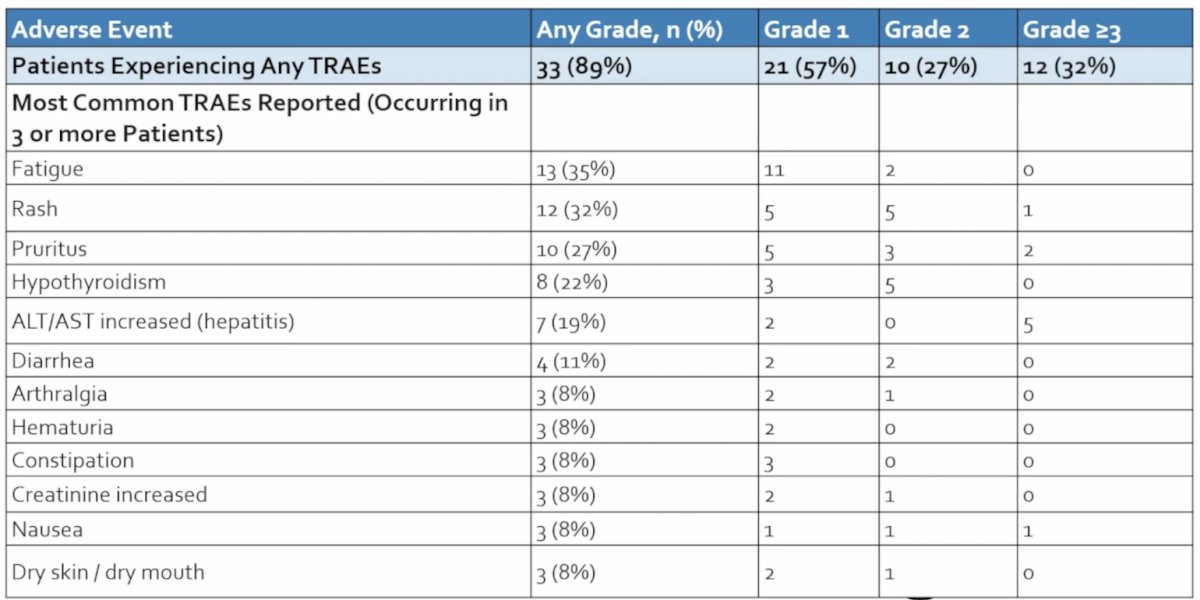
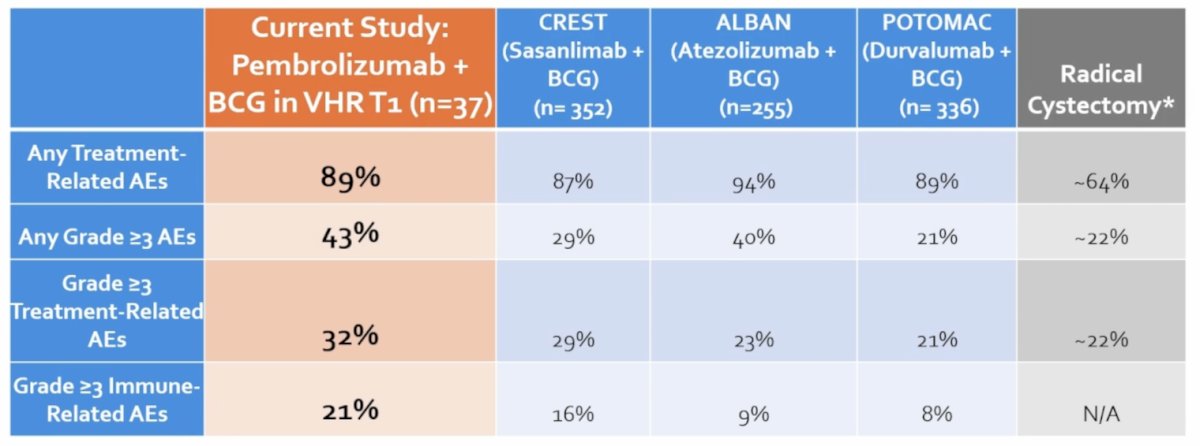
Overall, 89% of patients had any grade treatment related adverse event, including 32% with grade 3+ adverse events. The most common treatment related adverse events were fatigue, rash, pruritus, and hypothyroidism:
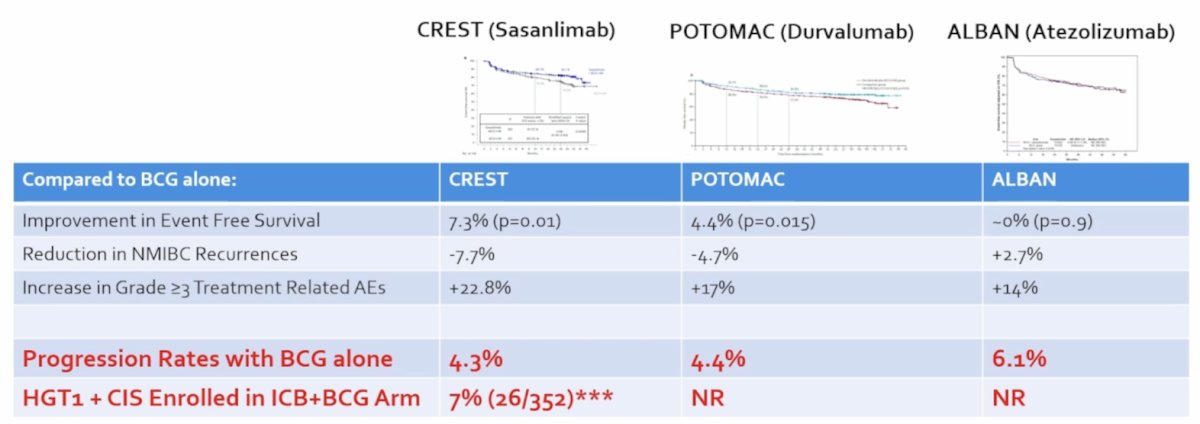
Dr. Pietzak provided the following table comparing the treatment related adverse events associated with immune checkpoint blockade + BCG in this trial with the CREST,1 ALBAN,2 and POTOMAC3 trials, as well as the general adverse event rates associated with radical cystectomy:
There are several limitations with this trial that Dr. Pietzak highlighted:
- A relatively small, single arm, non-randomized trial
- Results for KEYNOTE 676 are pending and should be informative
- Generalizability of results may be limited
- Conducted at a single, high volume cancer center
- Multi-disciplinary team specializing in bladder cancer
- All participants had re-TURBT/EUA at MSKCC, and routine use of NBI at TUR/follow-up
- Pembrolizumab treatments were overseen by GU medical oncologists
- BCG treatments overseen by urologic oncologists
- Pathology/cytology review was overseen by expert GU pathologists and cytopathologists
- Absence of mandated post-treatment biopsies may overestimate response
- Longer follow-up may mitigate these concerns
- Patient reported outcomes were not assessed
- Important when deciding between treatment options
Dr. Pietzak concluded his presentation discussing intravenous pembrolizumab combined with intravesical BCG for patients with BCG-naïve very high risk T1 non muscle invasive bladder cancer with the following take home points:
- Pembrolizumab + BCG had a 92% clinical complete response rate at 6 months
- Disease control appears durable, although longer follow-up is needed
- There was no progression to muscle invasive or metastatic disease at a median follow-up of 22 months
- These results compare favorably to historical outcomes for BCG alone in very high risk T1 non muscle invasive bladder cancer
- However, this was at the cost of 21% grade 3+ immune related adverse events
- These findings support pembrolizumab + BCG as a potential bladder preserving option in carefully selected patients who decline cystectomy, but are at very high risk for progression with BCG alone
Presented by: Eugene Pietzak, MD, Memorial Sloan Kettering Cancer Center, New York, NY
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the American Urological Association (AUA) 2026 Annual Meeting, Washington, DC, Fri, May 15 – Mon, May 18, 2026.
References:
- Shore ND, Powles TB, Bedke J, et al. Sasanlimab plus BCG in BCG-naïve, high-risk non-muscle invasive bladder cancer: The randomized phase 3 CREST trial. Nat Med. 2025 Aug;31(8):2806-2814.
- Roupret M, Bertaut A, Pignot G, et al. ALBAN (GETUC-AFU 37): A phase 3, randomized, open-label, international trial of intravenous atezolizumab and intravesical Bacillus Calmette-Guerin (BCG) versus BCG alone in BCG-naïve high-risk, non-muscle invasive bladder cancer (NMIBC). Ann Oncol. 2025 Dec 31:S0923-7534(25):04787-8 [Epub ahead of print].
- De Santis M, Palou Redorta J, Nishiyama H, et al. Durvalumab in combination with BCG for BCG-naïve, high-risk, non-muscle-invasive bladder cancer (POTOMAC): Final analysis of a randomized, open-label, phase 3 trial. Lancet. 2025 Nov 8;406(10516):2221-2234.