(UroToday.com) The 2026 American Urological Association annual meeting featured practice-changing, paradigm-shifting clinical trials in urology and a presentation by Dr. Neal Shore discussing expanded efficacy and safety analyses from POTOMAC assessing durvalumab with BCG therapy for high-risk non-muscle invasive bladder cancer. In non-muscle invasive bladder cancer, early high-risk disease recurrence is associated with worse outcomes, and BCG-unresponsive disease is an indication for radical cystectomy.
Reducing the risk of early recurrence and BCG-unresponsive disease, and therefore the need for cystectomy, is important from a clinical and patient perspective. Papillary tumors constitute the majority of non-muscle invasive bladder cancer diagnoses, and their prognosis depends on disease stage and grade. With standard of care BCG (induction + maintenance), poor outcomes are observed for patients with papillary stage T1 and high-grade tumors. In POTOMAC, the addition of 1 year of durvalumab to BCG (induction + maintenance) therapy demonstrated:1
- Statistically significant and clinically meaningful improvement in disease-free survival: HR 0.68 (95% CI, 0.50–0.93); p = 0.0154
- Early and sustained disease-free survival benefit (starting at <4 months)
- No detriment to overall survival: HR 0.80 (95% CI, 0.53–1.20), with a median follow-up of >5 years (66 months)
- A manageable safety profile, consistent with the known safety profiles of the individual therapies
At the 2026 AUA annual meeting, Dr. Shore and colleagues presented expanded efficacy and subgroup analyses, as well as additional safety outcomes from the POTOMAC trial.
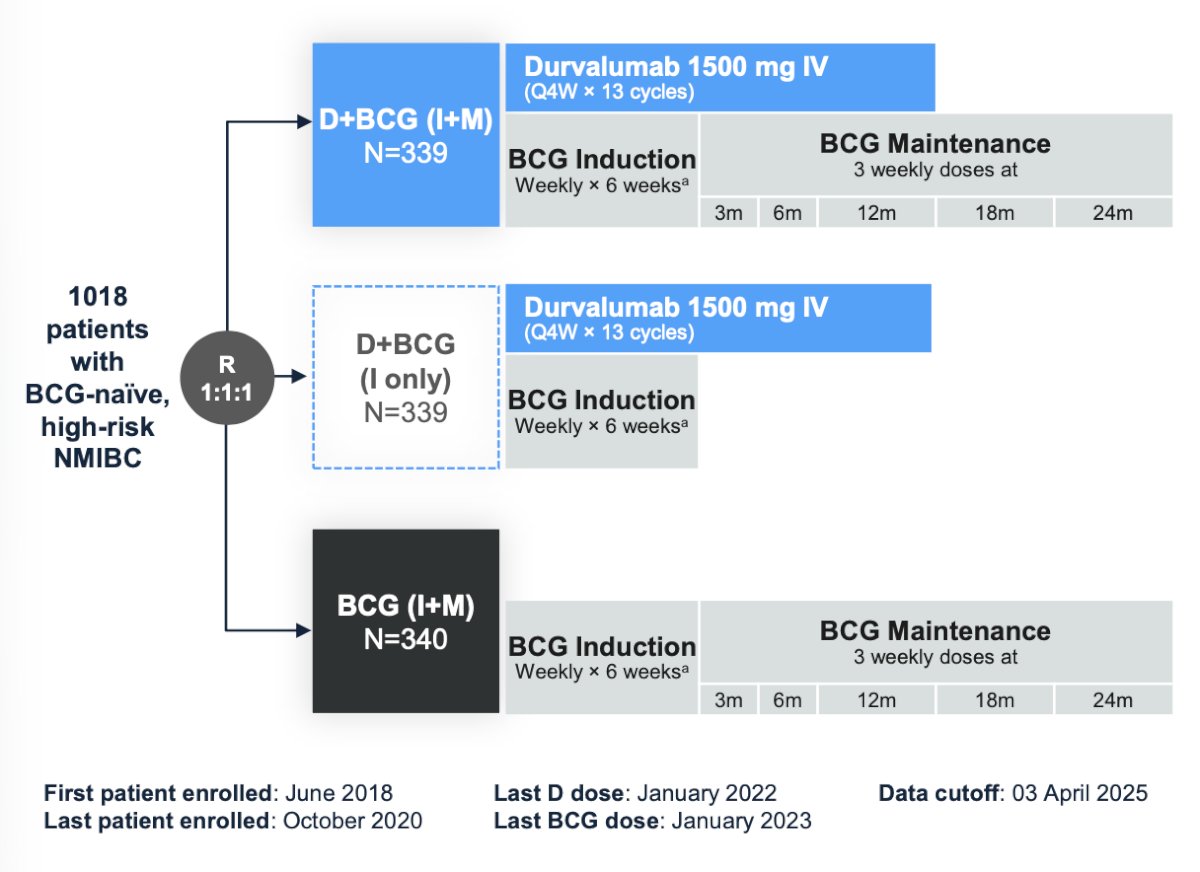
Eligible adult patients with BCG-naïve, local histologically confirmed high-risk non-muscle invasive bladder cancer who had TURBT (complete resection, including patients with residual CIS) were randomized 1:1:1 to receive durvalumab + BCG (induction + maintenance), durvalumab + BCG induction only, or BCG (induction + maintenance). Durvalumab was administered intravenously (1,500 mg every 4 weeks for 13 cycles), and intravesical BCG was given weekly × 6 weeks (induction only) and as 3 weekly doses at 3, 6, 12, 18, and 24 months. Patients were stratified by higher-risk papillary disease and CIS. The primary endpoint was investigator-assessed disease-free survival with durvalumab + BCG (induction + maintenance) versus BCG (induction + maintenance). The trial design for POTOMAC is as follows:
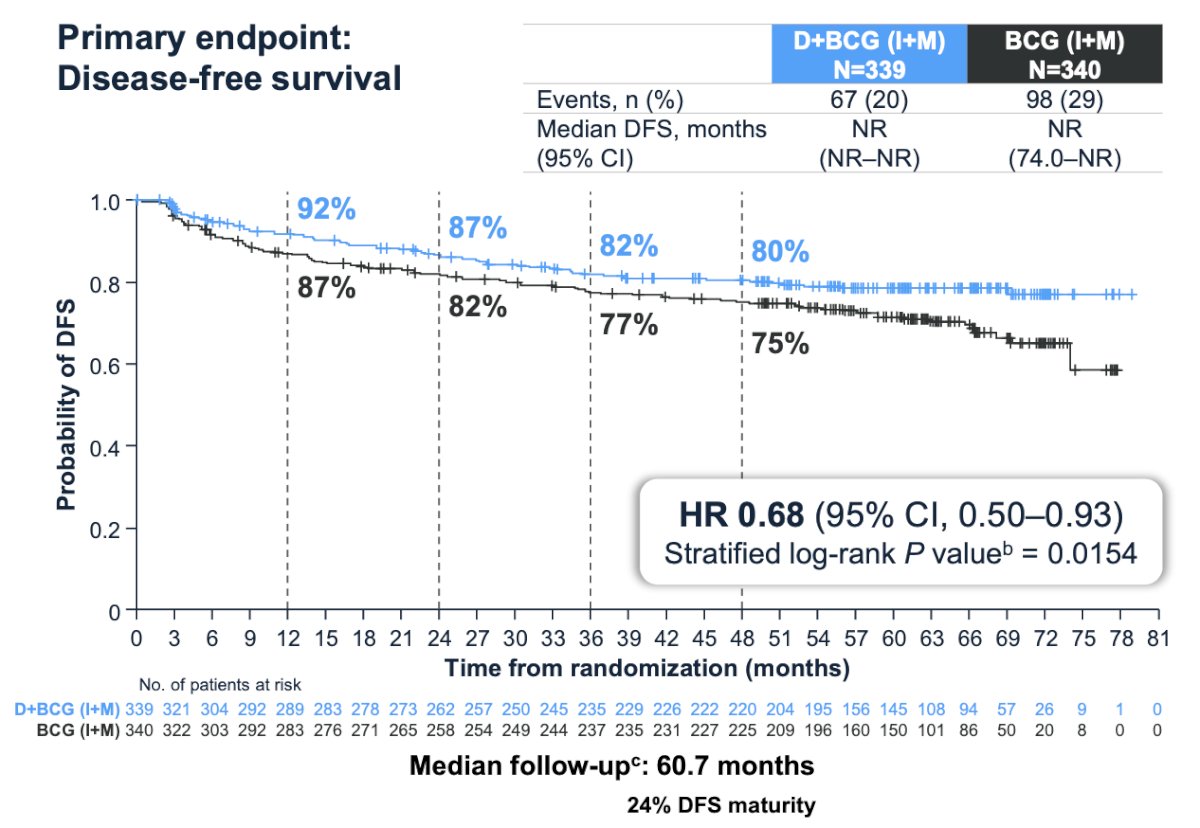
Previously reported, the primary endpoint of disease free survival was met with a 32% reduction in risk of recurrence of high risk disease or death by any cause for durvalumab + BCG (induction + maintenance) versus BCG (induction + maintenance) (HR 0.68, 95% CI 0.50–0.93; log-rank p = 0.0154), and 24-month disease free survival rates were 86.5% (95% CI 82.2–89.8) for durvalumab + BCG (induction + maintenance) and 81.6% (95% CI 76.9–85.3) for BCG (induction + maintenance):
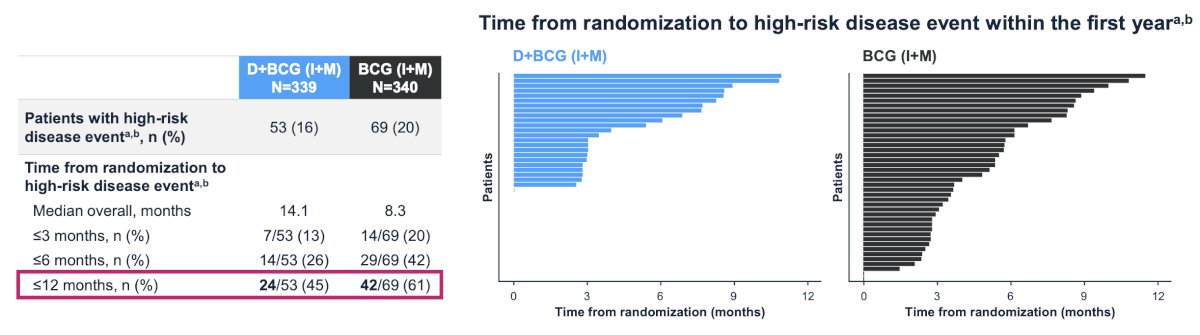
Durvalumab + BCG (induction + maintenance) also prevented early recurrences compared with BCG (induction + maintenance) alone. A high-risk disease event was defined as high-risk non-muscle invasive bladder cancer recurrence (HG Ta, T1, or CIS), persistent CIS at 6 months, muscle invasive bladder cancer, and/or metastatic disease:
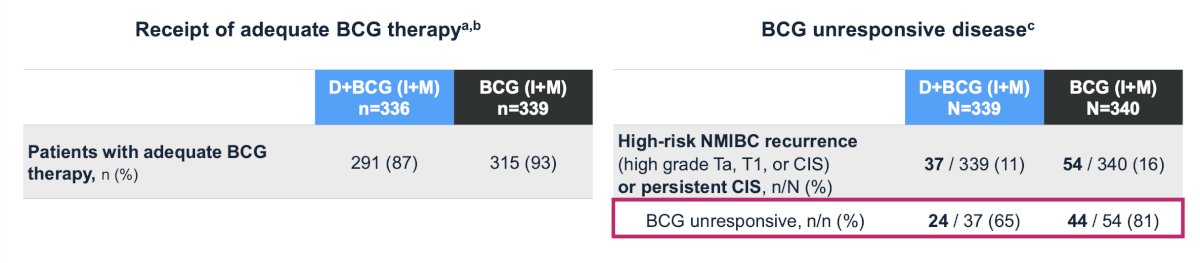
The majority of patients received adequate BCG therapy. Most patients with high-risk non-muscle invasive bladder cancer recurrence or persistence CIS met BCG unresponsive criteria, with fewer BCG unresponsive recurrences in the durvalumab + BCG (induction + maintenance) arm versus the BCG (induction + maintenance) arm alone:
Thus, the addition of durvalumab to BCG (induction + maintenance) did not impact patients’ ability to receive adequate BCG therapy. Time to cystectomy showed a trend in favor of the durvalumab + BCG (induction + maintenance) arm versus the BCG (induction + maintenance) arm alone, with fewer patients undergoing cystectomy, and a longer median time to cystectomy, compared with the BCG (induction + maintenance) arm alone:
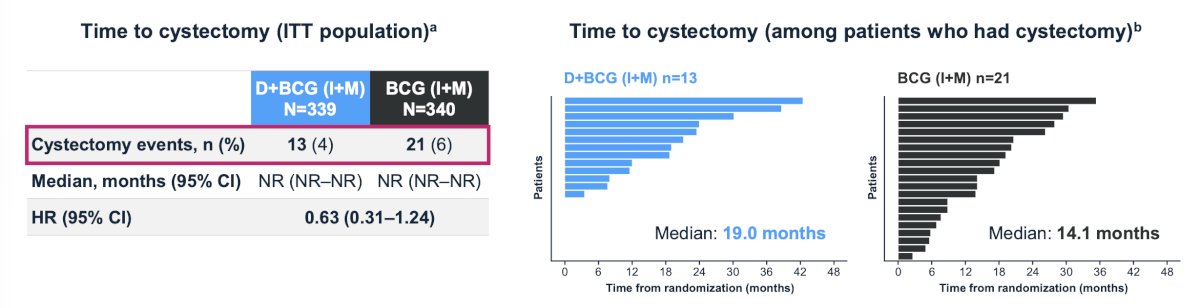
Further, fewer cystectomies were performed in the durvalumab + BCG (induction + maintenance) arm compared to the BCG (induction + maintenance) arm, which was also observed in patients with BCG-unresponsive disease:
- In the durvalumab + BCG (induction + maintenance) arm, 2/24 (8%) patients underwent cystectomy
- In the BCG (induction + maintenance) arm, 11/44 (25%) patients underwent cystectomy
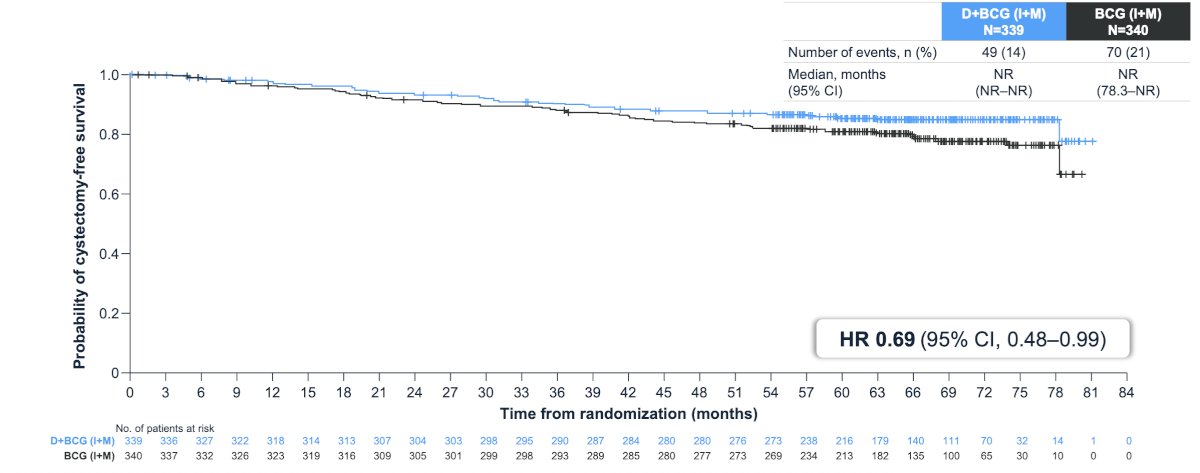
Cystectomy free survival showed a favorable trend for durvalumab + BCG (induction + maintenance) arm versus BCG (induction + maintenance) arm alone (HR 0.69, 95% CI 0.48-0.99):
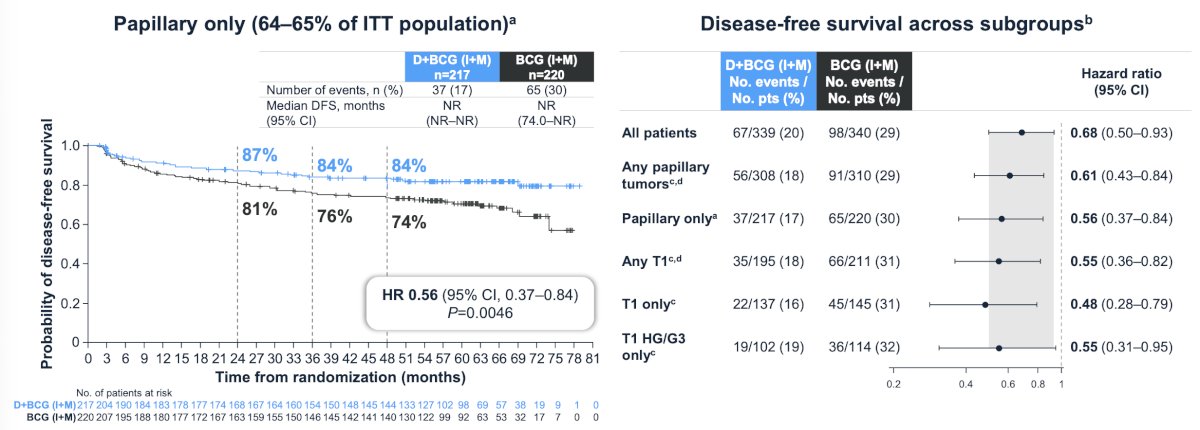
There was a 39% to 52% reduction in the risk of high-risk disease recurrence or death across papillary tumor subgroups with durvalumab + BCG (induction + maintenance) versus BCG (induction + maintenance):
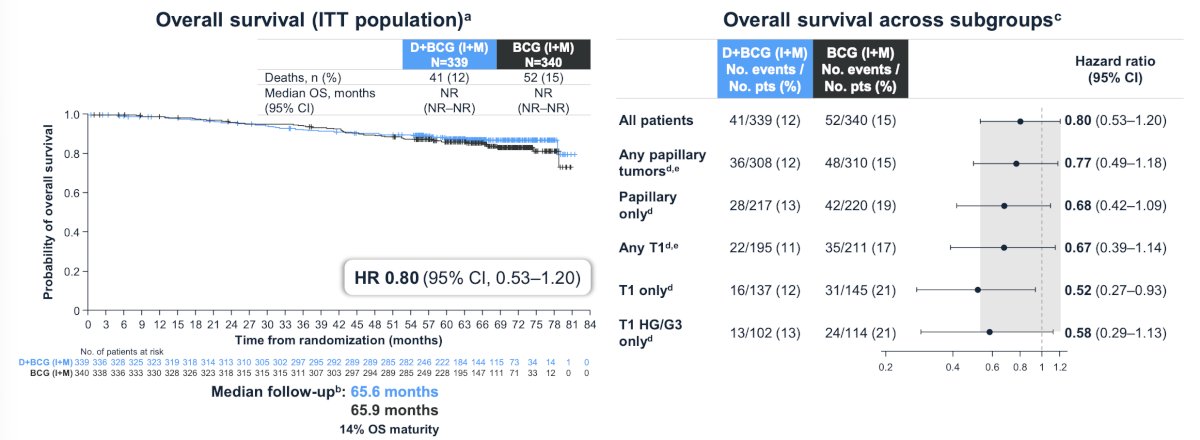
No detriment to overall survival (HR 0.80, 95% CI 0.53-1.20) was observed with the addition of durvalumab to BCG (induction + maintenance) across papillary subgroups:
The safety profile of durvalumab + BCG (induction + maintenance) in patients with papillary-only tumors was consistent with the overall safety population:
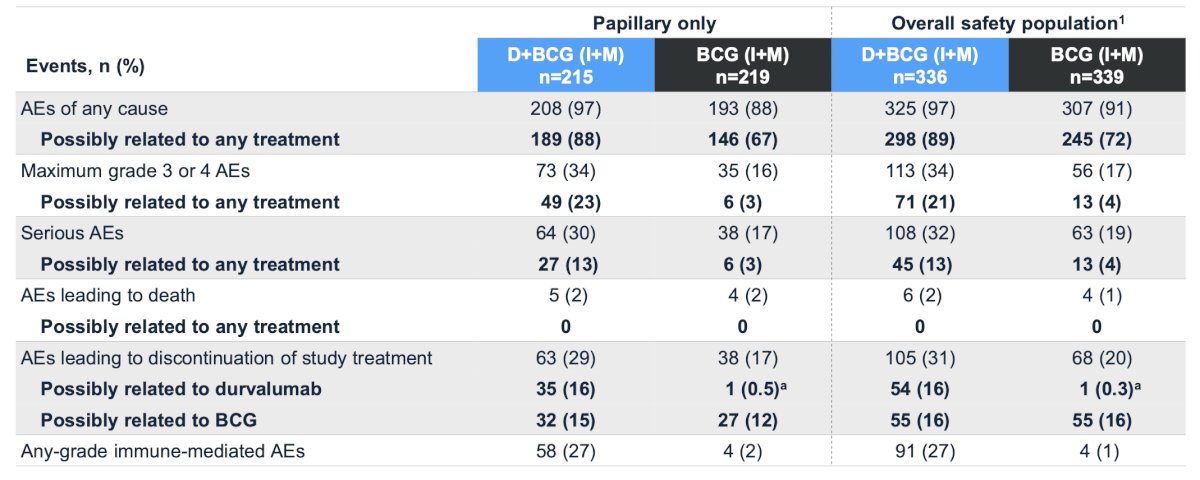
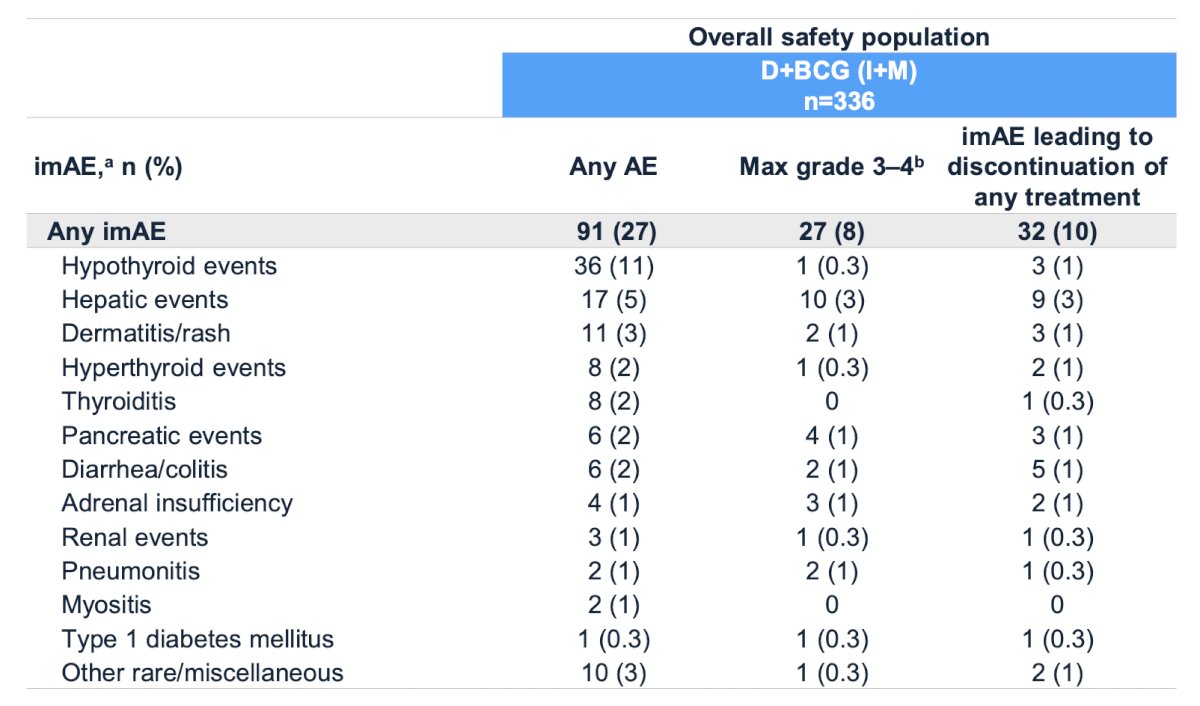
The majority of immune adverse events in the overall survival population were low-grade and manageable, and consistent with the mechanism of durvalumab:
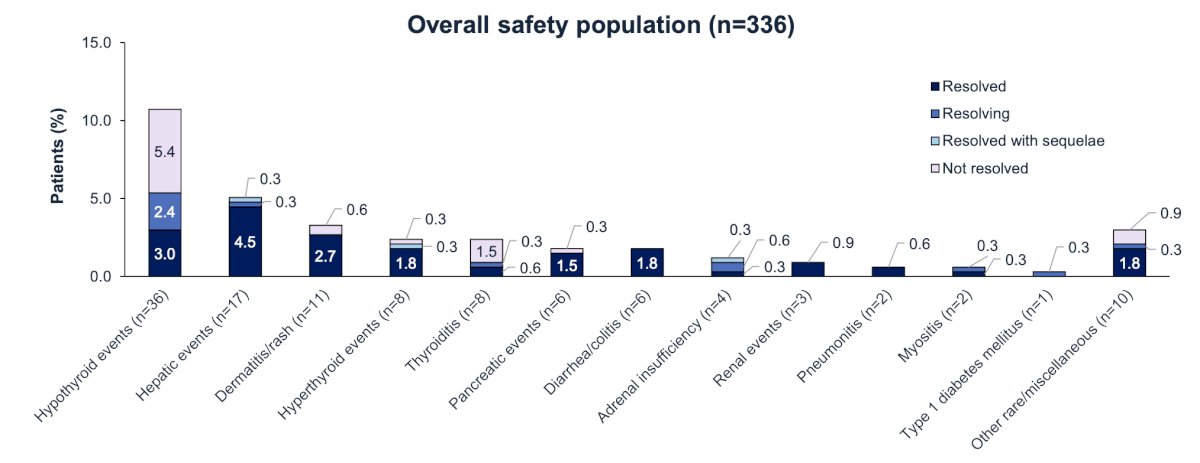
Of patients who experienced immune adverse events in the overall safety population, 67% had these events resolved (with or without sequelae) or were resolving at the time of data cutoff:
Dr. Shore concluded his presentation discussing expanded efficacy and safety analyses from POTOMAC with the following take-home points:
- The phase 3 POTOMAC study met its primary endpoint, demonstrating that durvalumab plus BCG (induction + maintenance) reduced the risk of high-risk disease recurrence or death by 32% compared with BCG (induction + maintenance) alone (HR 0.68; 95% CI, 0.50–0.93)
- The addition of durvalumab to BCG (induction + maintenance) therapy led to:
- Fewer early high-risk disease recurrences
- Delayed time to high-risk events
- Fewer BCG unresponsive recurrences
- Fewer cystectomies were observed, with favorable trends for time to cystectomy and cystectomy-free survival
- Notable disease-free survival benefit across subgroups of patients with papillary tumors
- Safety of durvalumab + BCG (induction + maintenance) in the overall safety population and across papillary subgroups was consistent with the known safety profiles of the individual therapies, and the immune adverse events were mostly low grade and manageable
- These data further support 1 year of durvalumab in combination with BCG (induction + maintenance) as a potential new treatment for patients with BCG-naïve, high-risk non-muscle invasive bladder cancer
Presented by: Neal D. Shore, MD, FACS, Director, CPI (Certified Principal Investigator by the Association of Clinical Research Professionals), START Carolinas/Carolina Urologic Research Center, Head of GU Oncology and Radiopharm, START Center for Cancer Research Institute, AUC Urology Specialists, Myrtle Beach, SC
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the American Urological Association (AUA) 2026 Annual Meeting, Washington, DC, Fri, May 15 – Mon, May 18, 2026.
Reference: