(UroToday.com) The 2026 American Urological Association annual meeting featured a non-invasive bladder cancer session and a presentation by Dr. Daniel Joyce discussing a cost-effectiveness analysis from CREST assessing sasanlimab + BCG for high-risk non-muscle invasive bladder cancer. The phase 3 CREST trial demonstrated that combining sasanlimab, a subcutaneous checkpoint inhibitor, with BCG improved event-free survival compared to BCG alone for patients with BCG-naïve high-risk non-muscle invasive bladder cancer.1
However, patients treated with sasanlimab + BCG experienced higher rates of ≥ grade 3 treatment-related adverse events, including 15.7% with ≥ grade 3 immune adverse events, and the cost of checkpoint inhibitors is substantial. At the AUA 2026 annual meeting, Dr. Joyce and colleagues used a Markov model to weigh the costs, toxicities, and efficacy of sasanlimab + BCG to further investigate its utility.
Dr. Joyce and colleagues used a decision-analytic Markov model to compare sasanlimab + BCG to BCG alone for BCG-naïve high-risk non-muscle invasive bladder cancer. Efficacy and toxicity model probabilities were extracted from the CREST trial. Cost data for sasanlimab were extrapolated from subcutaneous nivolumab pricing ($24,225/dose), as sasanlimab is not currently FDA-approved. The model used a U. S. Medicare payer perspective with a lifetime time horizon. One-way and probabilistic sensitivity analyses were performed to vary all model inputs across biologically plausible ranges. Incremental cost-effectiveness ratios were compared using a willingness to pay threshold of $100,000/quality-adjusted life year.
Over a patient’s lifetime, the combination of sasanlimab + BCG resulted in 0.03 additional quality-adjusted life years (6.11 versus 6.08) at an additional cost of $191,666 relative to BCG alone. Combination therapy was found not to be cost-effective over a lifetime horizon (incremental cost-effectiveness ratio = $6,440,594). On one-way sensitivity analysis, the combination of sasanlimab + BCG became cost-effective only if the per-dosing price of sasanlimab was reduced by > 90% (to $1244/dose) from the existing pricing of a currently available subcutaneous checkpoint inhibitor: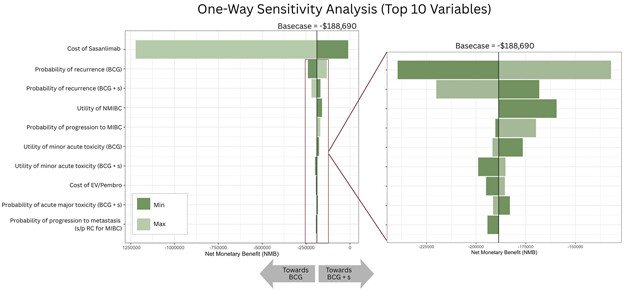
Dr. Joyce concluded his presentation discussing a cost-effectiveness analysis from CREST with the following take-home points:
- Sasanlimab + BCG is not cost-effective relative to BCG alone
- The overall improvement in effectiveness is marginal (11 days of perfect health), given the incidence of treatment toxicity with immune checkpoint inhibitors and the already high effectiveness of BCG alone
- Further efforts are needed to improve the efficacy/toxicity profile of novel therapies
- Continued scrutiny of the healthcare system cost implications of new agents remains warranted
- To help address the exponential rise in bladder cancer treatment costs, the investigators created a publicly available cost-effectiveness tool based on these findings to facilitate the incorporation of value assessments in clinical trial development, as well as healthcare policy and reimbursements
Presented by: Daniel Joyce, MD, MS, Assistant Professor of Urology, Division of Urologic Oncology, Vanderbilt University Medical Center, Nashville, TN
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the American Urological Association (AUA) 2026 Annual Meeting, Washington, DC, Fri, May 15 – Mon, May 18, 2026.
Reference: