(UroToday.com) A panel of specialists convened to discuss contemporary strategies in the management of Fournier’s gangrene, a life-threatening urological emergency requiring rapid intervention, multidisciplinary care, and long-term reconstruction planning. Moderated by Dr. Steven Hudak, the panel featured Dr. Alex Skokan, Dr. Krishnan Venkatesan, and Dr. Lindsey Hartsell, who shared staged approaches across the phases of Fournier’s disease—from acute infection control to delayed reconstruction.

Dr. Skokan began by emphasizing the importance of infection control during the acute phase, particularly within the first 24–48 hours. He stressed the need for aggressive intervention involving wide exposure and drainage of necrotic tissue, balanced with the goal of preserving as much viable skin as possible to facilitate future wound closure. For high-quality skin-sparing debridement, he advised a comprehensive strategy. Surgeons should identify the location that is obviously most infected or discolored before placing longitudinal incisions on extremities that avoid skin creases or sulci. That will allow wide elevation of flaps that can be lengthened with further longitudinal incising. Then all necrotic tissue can be excised, as well as overlying skin, and the infection can be drained, ensuring that viable tissue is maintained. Dr. Skokan highlighted skin-sparing debridement as a critical advancement, with evidence suggesting improved survival and wound closure outcomes compared to traditional wide excision approaches.


Early recognition of prodromal cases—especially in patients with morbid obesity or recurrent urinary tract infections—was emphasized as crucial for timely surgical intervention. Dr. Skokan also discussed the use of serologic markers such as the LRINEC score, noting its utility not just in diagnosis but in serial monitoring across successive debridement. He shared data showing a consistent decline in LRINEC scores during treatment, supporting its value in tracking disease resolution and guiding intraoperative decision-making.

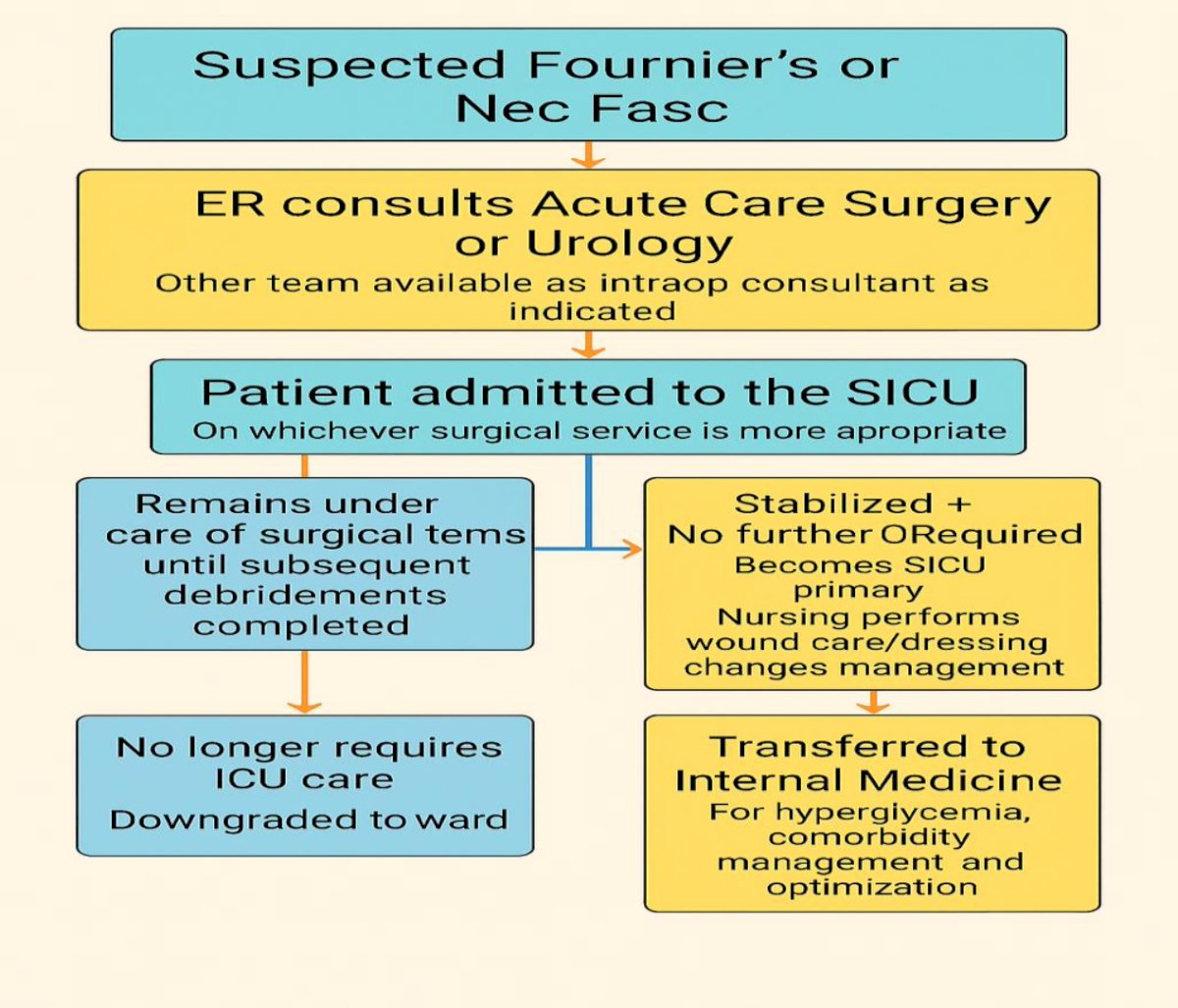
As the patient progresses to the subacute phase, Dr. Venkatesan highlighted the need for multidisciplinary stabilization with involvement from the ICU, general surgery, urology, plastic surgery, infectious disease, and palliative care teams. He described the intensive care support required, including fluid resuscitation, broad-spectrum antibiotic coverage, and tight glycemic control. The surgical management at this stage involves scheduled second-look operations—typically within 24 to 48 hours—to reassess the wound and perform any additional debridement. Dr. Venkatesan noted that patients often undergo an average of three operative interventions before the infection is sufficiently controlled to allow for reconstructive planning. He underscored the relevance of prognostic tools like Fournier’s Gangrene Severity Index (FGSI), which aid in assessing surgical risk, optimizing the timing of interventions, and guiding the broader plan of care.
Going through images, he outlined the common repair and recovery processes of a common patient who has gone through several debridements. However, cases can be more complex and require support from other specialties, such as plastic surgery, which can assist by placing thigh pouches for testicular support. Once the patient is stable, management is typically deferred to the medical team for optimization and treatment of any other underlying disorders.
Dr. Hartsell addressed the delayed phase of care, focusing on the reconstructive strategies employed once the infection has resolved and the patient has been stabilized. She noted that delayed reconstruction is typically necessary when wounds are not yet granulating or when systemic comorbidities remain poorly optimized. Wound management options at this stage range from extended inpatient care to outpatient management with negative pressure wound therapy (NPWT) or referral to rehabilitation facilities. While the role of hyperbaric oxygen therapy remains somewhat controversial, Dr. Hartsell acknowledged its potential benefits for survival, even though access and cost remain limiting factors. It can have increased oxygen delivery to tissues, bactericidal effects against anaerobic infections, and increased angiogenesis. However, there has been no comparative data demonstrating a difference in the number of debridements or the length of hospital stay required by Fournier patients.
She then outlined reconstructive strategies tailored to the size and depth of the defect. Small wounds may heal by secondary intention, while moderate defects may be amenable to delayed primary closure with local advancement flaps. For more extensive or deeper wounds, split-thickness skin grafts, preferably non-meshed for better cosmetic outcomes, are often used. In terms of choosing between meshed or non-meshed skin grafts, reasons for non-meshed include less risk of contracture, improved cosmetic outcomes, maintenance of sexual function in cases with penile involvement, and pie-crusting for prevention of seromas or hematomas. Conversely, meshed grafts allow for increased coverage area and graft take, but also an increased risk of contracture. In a similar vein, there is a decision that can be made between local fasciocutaneous flaps and myocutaneous flaps in cases requiring substantial volume restoration. Local flaps can be sourced from the medial and pudendal thighs. Myocutaneous flaps are useful if there is dead space to fill in addition to skin coverage, with the most common ones being gracilis, anterolateral thigh, gluteal, VRAM (vertical rectus abdominis myocutaneous), and deep inferior epigastric perforator flaps.
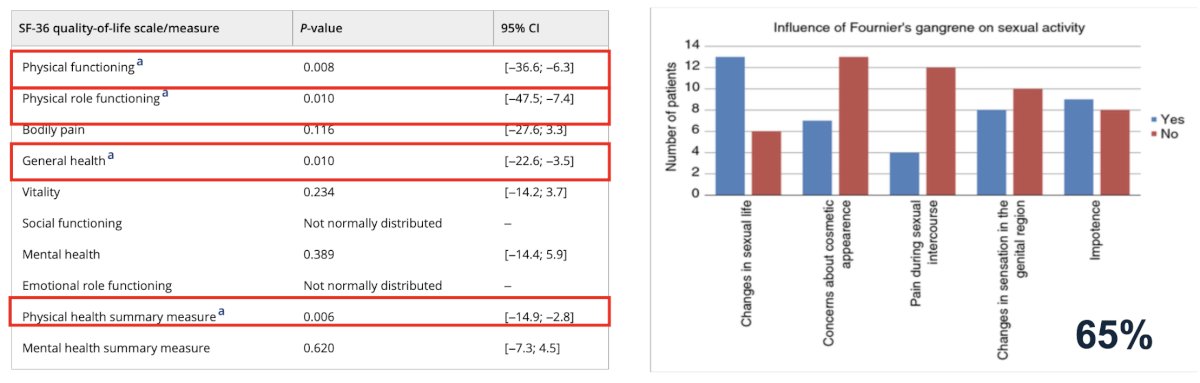
Dr. Hartsell then cited a quality-of-life study in patients using data from SF-36 questionnaires. The findings underscored the significant physical impairments experienced by patients with Fournier’s gangrene, highlighting the long-term impact this condition can have even after successful treatment.
Overall, the session reinforced that successful management of Fournier’s gangrene requires not only technical surgical expertise and critical care acumen but also long-term, patient-centered planning aimed at optimizing functional outcomes and quality of life.
Moderated by: Steven J. Hudak, MD, FACS, Distinguished Chair in Urology for Urologic Reconstruction, UT Southwestern Medical Center.
Expert Panel:- Alex J. Skokan, MD, Assistant Professor of Urology, Adjunct Assistant Professor of Plastic Surgery, University of Washington.
- Krishnan Venkatesan, MD, FACS, Associate Professor of Urology at Georgetown University, Director of Urologic Reconstruction, MedStar Health.
- Lindsey Hartsell, MD, Director of Reconstructive Urology, Emory University.
Written by: Yezan Hadidi, BS, Department of Urology, University of California Irvine. @yezanhadidi on X during the 2025 American Urological Association (AUA) annual meeting held in Las Vegas, NV, Saturday, April 26 - Tuesday, April 29, 2025