(UroToday.com) Monday afternoon’s plenary session continued with a case series of penile fractures of different etiologies. A penile fracture is a rupture of the tunica albuginea, typically caused by blunt trauma to an erect penis, often during vigorous sexual intercourse or upon penetration. It typically presents with a characteristic “popping” sound, immediate detumescence, swelling, and bruising, and usually requires urgent surgical repair to prevent long-term complications like erectile dysfunction or penile curvature.
The session kicked off with the first of three case presentations by men’s health expert and session moderator Dr. Faysal Yafi from the University of California, Irvine, as shown below.
Dr. Lawrence Jenkins from Tulane University took the podium to provide his expert opinion and approach to this case. Dr. Jenkins first explains that given the mechanism of injury (penile trauma during intercourse, particularly with the partner on top), the classing popping sound, immediate pain, swelling, and detumescence warrant urgent evaluation and potential surgical intervention.
The incidence of penile fracture is about 1.02 per 100,000 male subjects per year and most commonly occurs in the 4th decade of life, especially during the summer months. Moreover, when the penis is flaccid, the tunica albuginea is 2mm thick, but around 0.25-0.5mm thick making it more susceptible to rupture after forceful impact.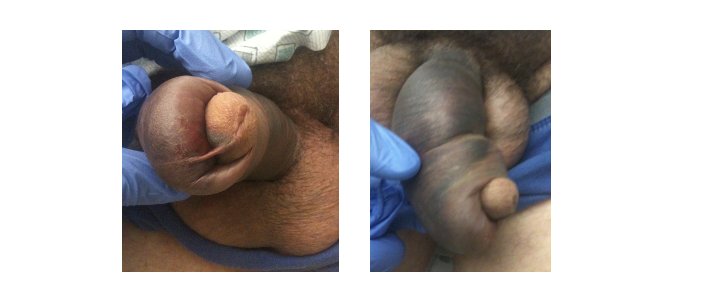
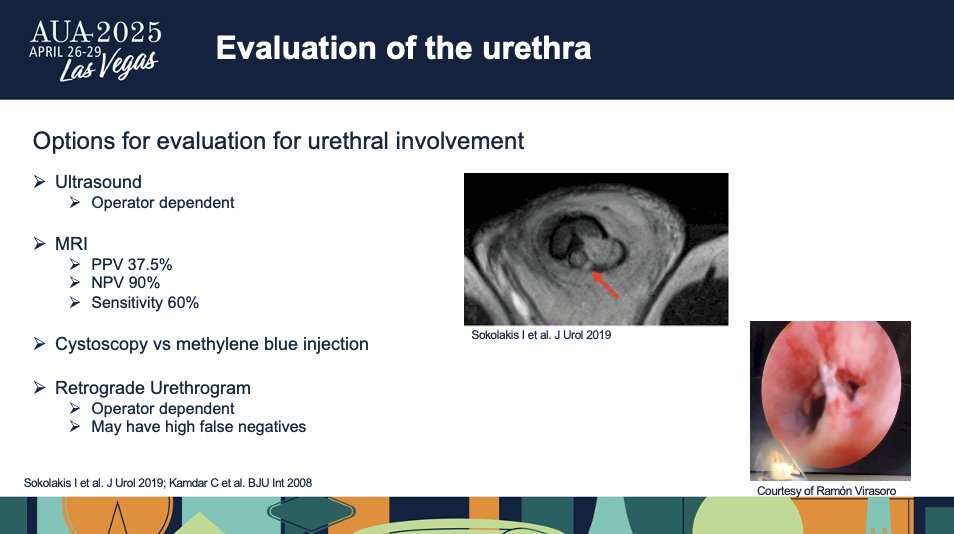
Dr. Jenkins goes on to share that the AUA Guidelines recommend prompt surgical exploration and repair for patients presenting with signs and symptoms of penile fracture. However, there is no specific guidance on a delayed presentation. Equivocal cases may benefit from the utilization of ultrasound or MRI to more definitively identify tunical rupture.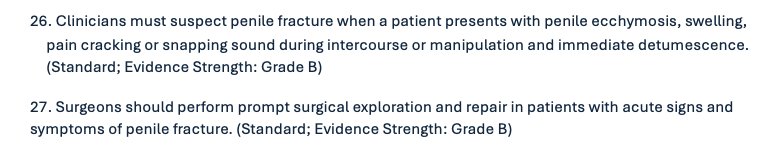
Literature has shown that when penile fractures are not surgically repaired, patients are at a higher risk for complications such as erectile dysfunction and penile curvature. Dr. Jenkins shared that in one study on penile fracture treatment, 96% of patients who had received surgical intervention versus 50% of patients who were treated conservatively were ultimately able to re-achieve an erection that was adequate for intercourse, with no voiding dysfunction and no penile curvature.
Multiple case reports have discussed late repairs from 7 to 42 days with low rates of erectile dysfunction or penile curvature, albeit with short follow-up. Due ot the nature of the disease, there is a lack of large clinical trials or longitudinal studies to assess outcomes.
Surgically, this is typically approached in one of two ways, through a degloving incision or direct incision over the rupture. Degloving allows for optimal exposure but may add extra complications for those who are uncircumcised. After the incision, the hematoma clot is removed, and the extent of the tear can be evaluated. With the delay in presentation, the hematoma may be more organized, and the presence of early fibrosis may make dissection and repair more technically challenging. The tunica is repaired using an absorbable suture of adequate strength, such as 2-0 or 3-0 monofilament or braided suture.
Lastly, Dr. Jenkins shares that postoperatively, the patient should abstain from all sexual activity for at least 6 weeks. Low-dose phosphodiesterase type 5 inhibitors may be used early postoperatively to optimize tissue oxygenation and prevent fibrosis. Given the patient’s presentation, surgical exploration and repair should still be pursued to optimize long-term outcomes.
At the conclusion, Dr. Yafi takes the podium to share the second case of a penile fracture that presents more acutely.
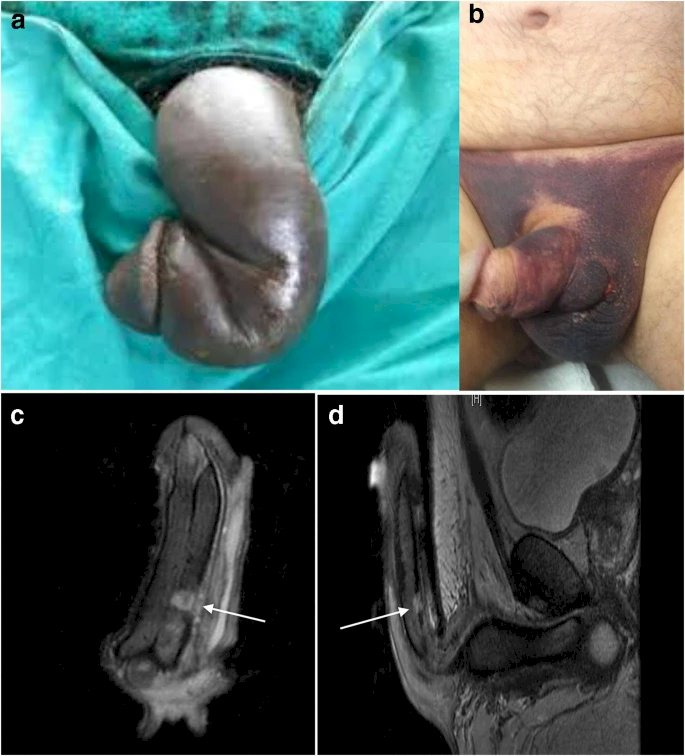
Dr. Maria Francesca Monn takes the stage to discuss her expertise in approaching this case. She begins by sharing that concomitant urethral involvement is estimated at 3.9% based on a recent systematic review, although this likely varies regionally and by etiology of the injury with some studies reporting up to urethral involvement in up to 27%. The most common presenting symptoms are blood at the meatus or hematuria, which should trigger a workup and discussion of potential injury with the patient. The proximal and mid shaft are the most common sites of tunical rupture associated with urethral injury, and it is more common to have a partial than complete rupture of the urethra.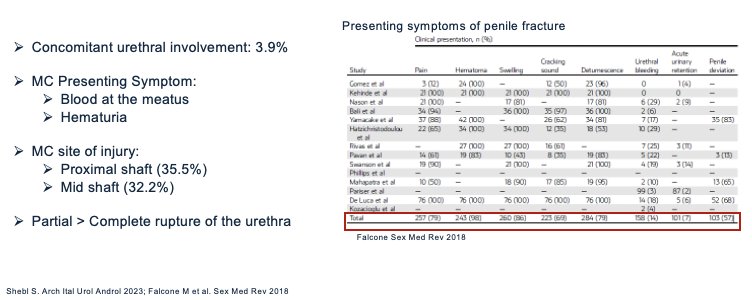
Moreover, Dr. Monn shares that one of the greatest risk factors for a urethral injury is a bilateral fracture, which you can see in this image. In a European multi-institutional study, 33% of patients with a bilateral fracture had urethral involvement compared with less than 12% of the unilateral patients. Of note, this study was not included in the prior systematic review and had a much higher rate of urethral involvement at around 11.6%.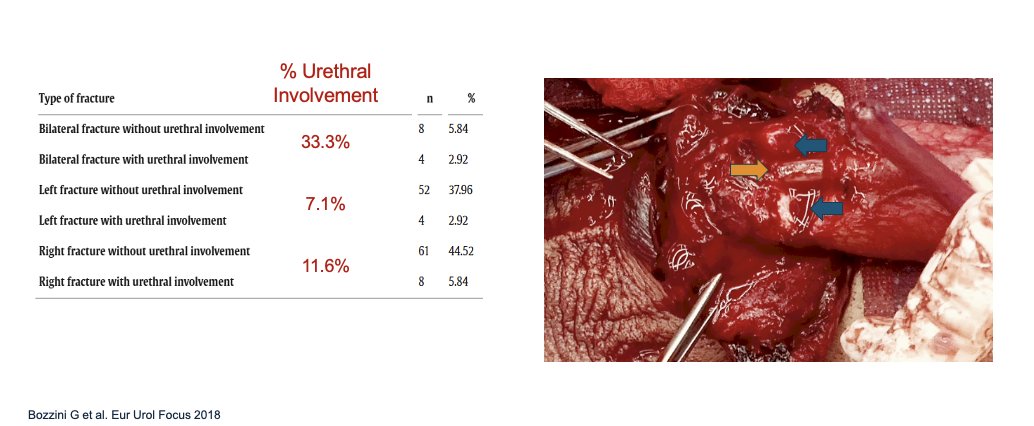
Dr. Monn shares her own appraoch to intraoperative repair of such a case:
“When repairing, I perform a degloving incision unless the injury is proximal in which I use a peno-scrotal incision. Urethral injuries are repaired with either 4-0 Vicryl or PDS with a 14fr catheter placed. The corpus is repaired with PDS. A dartos flap may be used to cover the incision. Depending on severity and swelling, a closed suction drain may be placed. Of note, if there is any concern for a urethral injury, I perform intraoperative flexible cystoscopy to evaluate.”
While surgical interventions can restore penile shape, adequate erection, and regular voiding, there are many potential complications following penile fracture with urethral involvement. An important note is the role of time to surgery in long term erectile function preservation. While erectile dysfunction is not specifically dependent on urethral involvement, urethral involvement is often associated with a more severe fracture.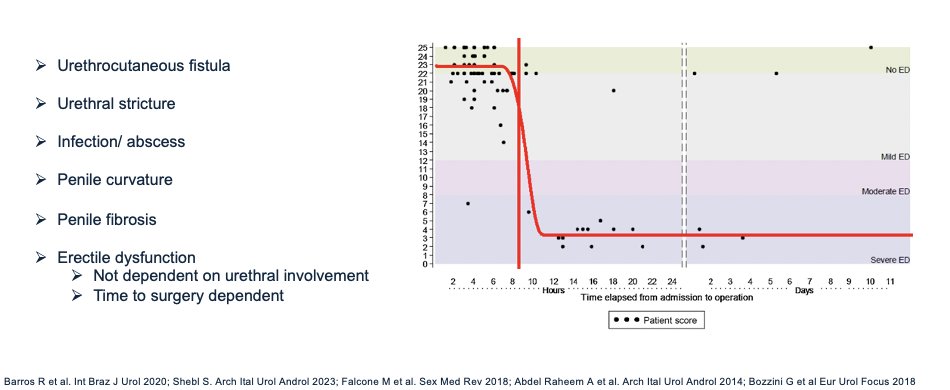
Dr. Monn ends her explanation of her approach with key points:
- Have a high index of suspicion if there is blood present at the meatus or hematuria
- Intraoperative cystoscopy is indicated if there is a concern for injury.
- Repair can be done with a primary urethroplasty.
- Time to repair matters for long-term erectile function.
Finally, Dr. Yafi takes the podium briefly to share the third and final case, inviting Dr. Jesse Mills from UCLA Urology in Santa Monica to share his expertise in his approach to the following case:

Dr. Mills takes the stage and begins by discussing intralesional Collagenase Clostridium Histolyticum therapy (CCH). CCH is the only FDA-approved medication for Peyronie’s Disease (PD). IMPRESS Trials demonstrated CCH efficacy in up to 34% curvature reduction. A rare but severe adverse event can occur, which is corporal rupture in 0 to 4.9% of cases.

Dr. Mills goes on to explain the crucial differences between traumatic versus CCH-associated fractures, and identifying and treating them. Traumatic penile fractures result from blunt force trauma, and immediate surgical repair improves erectile function and long-term outcomes compared to observation. CCH-associated fractures can occur at the site of injection or, at the weakest point of tunica at the ventrolateral aspect, and not necessarily at the site of injection. This is thought to result from applied force and ongoing transmural degradation of the tunica. Most cases occur spontaneously during erection or intercourse.
Dr. Mills mentions that in his own practice, in over 1000 men, no rupture has occurred during intercourse, 2 have occurred with nocturnal erection, and 2 with erect modeling.
Understanding the mechanism of rupture guides our decision-making in treatment plans. Traumatic penile fractures require ultrasound or immediate surgical intervention according to AUA guidelines. CCH-associated fractures require conservative management. More recent literature states that suspected penile fractures due to CCH have shown greater curvature improvement and similar erectile function with conservative treatment.
Recommendations and future guidelines for CCH patients include an increase in the post-injection abstinence period from 2 to 4 weeks. There is also a need for further research to optimize management. If a suspected CCH rupture occurs, the best take home practices are to evaluate immediately, ultrasound to measure tunical disruption, a tight coban wrap that must be changed daily, hot baths, and instructions on how to wrap at home. Moreover, it is crucial to ensure that a patient is still getting erections and that there is no formation of any expansive hematoma.
Dr. Mills leaves the audience with one final message before the conclusion of this session: “Mechanism Matters!” … Penile fractures are not all the same and must not be treated as such.
Moderated by: Faysal Yafi, Associate Professor of Urology, Director of Newport Beach Urology, Director of Men's Health, Chief, Division of Men's Health and Reconstructive Urology, University of California, Irvine, CA, USA
Expert Panel:- Lawrence Jenkins, Associate Chair, Associate Professor, Director of Men’s Health, Tulane University School of Medicine, New Orleans, LA, USA
- Maria Francesca Monn, Assistant Professor of Urology, Southern Illinois University, Springfield, IL, USA
- Jesse Mills, Director of the Men’s Clinic at UCLA, Fellowship Director of the Male Reproductive Medicine and Surgery program, Director of UCLA Urology, Santa Monica, CA, USA
Written by: Eman N. Chaudhri, MD, Department of Urology, University of California, Irvine, @EmanChaudhri on Twitter during the American Urological Association's 2025 Annual Meeting, between April 26 – 29, 2025, in Las Vegas, NV.