EMBARK is a randomized phase III trial of biochemically recurrent prostate cancer patients who had evidence of high-risk disease, defined as PSADT ≤9 months and a PSA of ≥2 ng/mL above nadir following radiation therapy or ≥1 ng/mL after radical prostatectomy, with or without postoperative radiation therapy. Eligible patients had no evidence of metastasis on conventional imaging and baseline eugonadal testosterone levels ≥150 ng/dL. Patients underwent 1:1:1 randomization as follows:
- Enzalutamide 160 mg + leuprolide acetate
- Placebo + leuprolide acetate
- Enzalutamide monotherapy
- PSA <0.2 ng/mL: Treatment was suspended at week 37 and PSA was monitored with treatment reinitiated if PSA rose again
- PSA >0.2 ng/mL: Treatment was continued

EMBARK included 1,068 patients, with a median serum PSA level at study entry of 5–5.5 ng/ml. The median PSADT was 4.6–5 months, with approximately 20% of patients having a PSADT ≤3 months. Half of the cohort had undergone both radical prostatectomy and radiation therapy, and 30% of patients had received prior hormonal therapy.
At a median follow-up of 60.7 months, patients in the combination arm of enzalutamide + leuprolide had significantly superior 5-year metastasis-free survival rates (87.3% versus 71.4%; HR 0.42, 95% CI 0.30–0.61, p < 0.001). Subgroup analyses demonstrated consistent benefits for this combination, irrespective of PSADT, baseline age, PSA, geographic region, receipt of prior hormonal therapy, or prior radical prostatectomy:

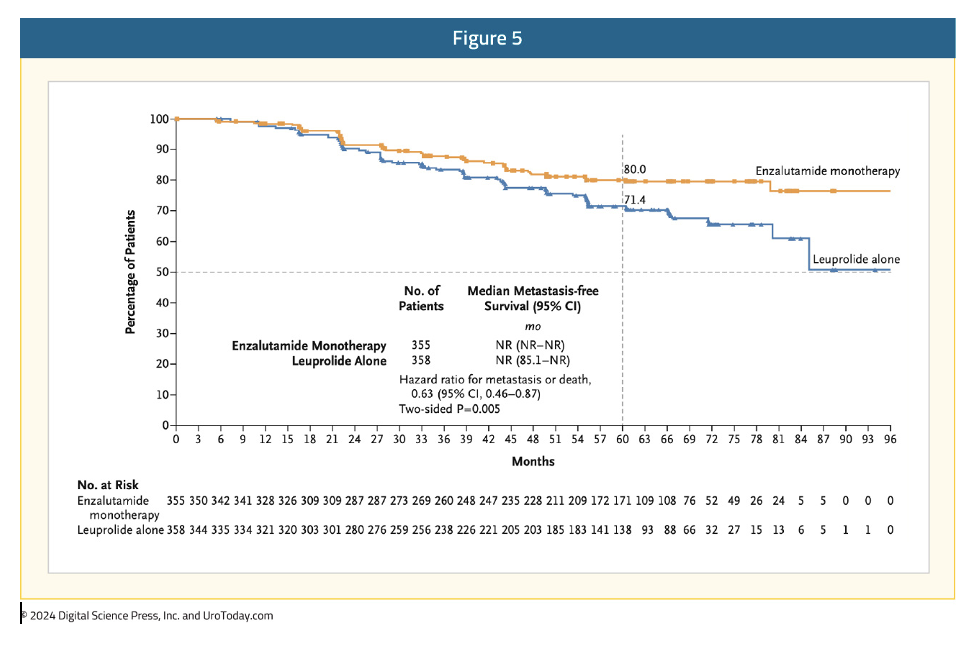
For the comparison of enzalutamide monotherapy to leuprolide monotherapy, patients in the enzalutamide monotherapy arm had superior 5-year metastasis-free survival (80% versus 71.4%; HR: 0.63, 95% CI: 0.46–0.87, p=0.005):1
The objective of this ad hoc analysis of the EMBARK trial was to assess testosterone recovery in patients treated with enzalutamide combination therapy and leuprolide alone, following treatment suspension. This is particularly relevant given that low testosterone levels induced by androgen deprivation correlate with poorer health outcomes, and testosterone recovery while off treatment has been associated with improved quality of life. Furthermore, given that older age correlates with slower time to testosterone recovery, subgroup analyses by patient age were performed.
Testosterone recovery in this analysis was defined as recovery to a level >175 ng/dL. While normal testosterone levels are typically defined as ≥250 ng/dL, the EMARK study entry criterion was a testosterone level ≥150 ng/dL. Dr. Freedland argued that a testosterone level of 175 ng/dL provides a clinically meaningful threshold for patients with lower-than-normal testosterone levels at baseline.
Among patients who had their treatment suspended by week 37, the median time to testosterone recovery was 8.3 months (range: 0–36) in the enzalutamide combination arm and 5.9 months (range: 0–47.1) in the leuprolide alone arm. Overall, 84% of patients in the enzalutamide combination arm and 88% of patients in the leuprolide arm had recovery of testosterone levels to >175 ng/dL. Additionally, 15% and 11% of patients in the two arms, respectively, had partial recovery of testosterone levels to 50–175 ng/dL. Thus, >98% of patients in the trial had at least partial testosterone recovery.
When stratified by patient age (<70 versus ≥70 years), there was a significantly higher proportion of testosterone recovery in the <70 years of age group:
- Enzalutamide combination: 89% versus 78%
- Leuprolide monotherapy: 92% versus 84%
Longitudinal testosterone recovery following treatment suspension is summarized below. Overall, recovery of testosterone levels was observed to start ~12 weeks following treatment suspension, which correlates with the observed improvements in quality-of-life outcomes following treatment suspension previously reported from this trial.1
Dr. Freedland concluded as follows:
- In this post hoc analysis of EMBARK assessing testosterone recovery following treatment suspension, most patients recovered their T levels during treatment suspension in both the enzalutamide combination and leuprolide alone arms.
- This recovery of testosterone levels was observed regardless of age group.
- As expected, a slightly higher percentage of patients <70 years of age recovered their testosterone levels in both the enzalutamide combination and leuprolide groups, compared with those ≥70 years of age.
- These findings may help explain the improvement in hormonal treatment-related quality of life following treatment suspension in the EMBARK trial.
Written by: Rashid K. Sayyid, MD, MSc – Robotic Urologic Oncology Fellow at The University of Southern California, @rksayyid on Twitter during the 2025 American Urological Association (AUA) annual meeting held in Las Vegas, NV, Saturday, April 26 - Tuesday, April 29, 2025
Related content: EMBARK Analysis: Testosterone Recovery Post-ADT in High-Risk Prostate Cancer Patients - Stephen Freedland
References:
- Freedland SJ, de Almeida Luz M, De Giorgi U, et al. Improved Outcomes with Enzalutamide in Biochemically Recurrent Prostate Cancer. N Engl J Med. 2023; 389(17):1453-1465.