(UroToday.com) The American Urologic Association (AUA) 2025 Annual Meeting held in Las Vegas, NV between April 26th and 29th, 2025 was host to an advanced prostate cancer podium session. Dr. Neal Shore presented the results of a real-world study evaluating time-to-next treatment and castration-resistance in metastatic castration-sensitive prostate cancer (mCSPC) patients treated with androgen receptor pathway inhibitors (ARPIs).
The treatment of mCSPC is challenged by the molecular heterogeneity of the disease. Patients harboring homologous recombination repair (HRR) mutations, particularly BRCA1 and BRCA2, have more aggressive disease courses and are less responsive to traditional treatments.1,2 Novel treatments such as poly ADP-ribose polymerase (PARP) inhibitors are currently being investigated for the treatment of HRR positive mCSPC.3,4 While ARPIs are a common treatment for patients with mCSPC, real-world evidence of clinical outcomes among patients treated with ARPIs with HRR mutations remains limited.
This was a descriptive analysis using retrospective data of real-world clinical outcomes among patients with mCSPC treated with ARPIs, with and without HRR mutations. The study outcomes were real-world time-to-next-treatment (TTNT) and time-to-castration resistance (TTCR).
The study design was as follows:
- Retrospective, longitudinal cohort analysis
- Patients were classified into cohorts (HRR positive [HRR+]1, including BRCA1/2 positive [BRCA+] subgroup, or HRR negative [HRR-]) based on testing results observed any time prior to progression to castration resistance, if observed
- The observation period spanned from the ARPI initiation (index date) to the end of clinical activity or data availability (12/31/2022)
- Data was obtained from the US-based Flatiron Health-Foundation Medicine, Inc. Metastatic PC Clinico-Genomic Database.
Patients with mCSPC who initiated an ARPI on/after 1/1/2018 and were tested for an HRR mutation were included. Patients were excluded if they had evidence of:
- Progression to castration resistance prior to/on the index date
- Use of clinical trial medication as initial mCSPC treatment
- Diagnosis of another primary cancer prior to metastasis
TTNT and TTCR were analyzed using Kaplan-Meier analyses.
The study flow chart is illustrated below. Overall, there were 125 HRR+ patients, of whom 88 were BRCA+, and 620 HRR- patients.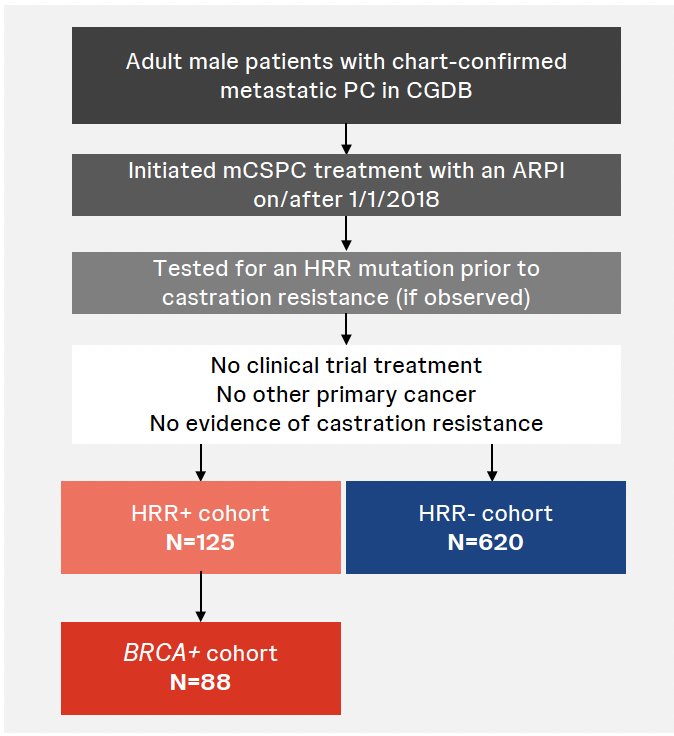
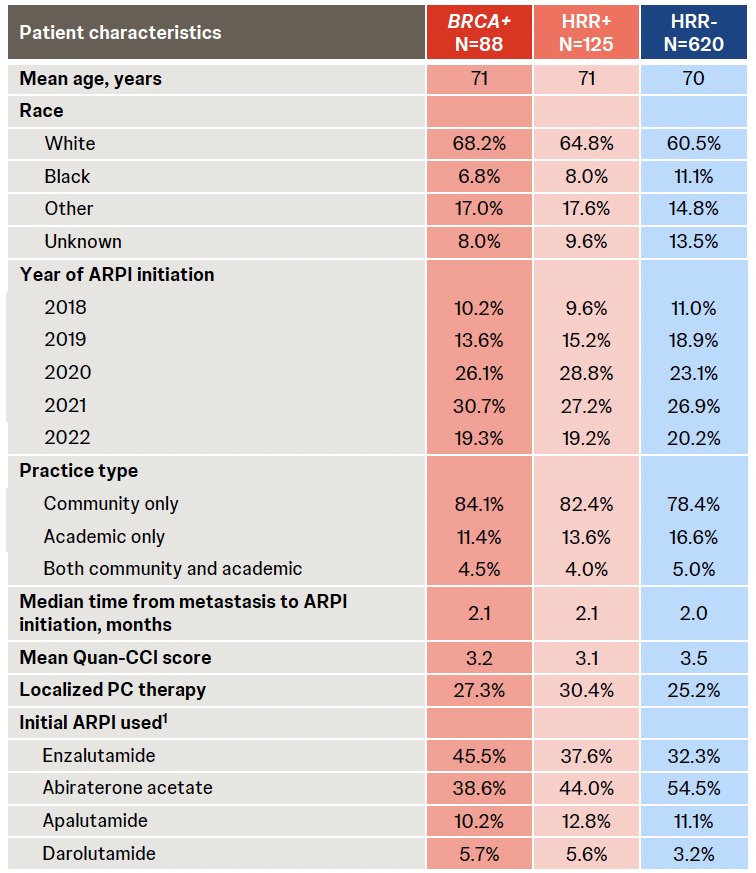
The baseline patient characteristics are summarized below. The mean age was similar across cohorts (71 years HRR+ and BRCA+, 70 years HRR-). Approximately two-thirds of patients in each cohort were White. Most patients were treated in community-based oncology practices. Across all cohorts, enzalutamide and abiraterone acetate were the most frequently used ARPIs. Overall, 5.5% of patients received ≥2 HRR tests.
By 24 months, 60% of BRCA+ patients had received a next treatment, which was a higher proportion relative to 48% of HRR+ and 48.1% of HRR- patients. BRCA+ patients had a median TTNT of 19.6 months, which was shorter relative to 24.9 months among HRR+ and 27.2 months among HRR- patients.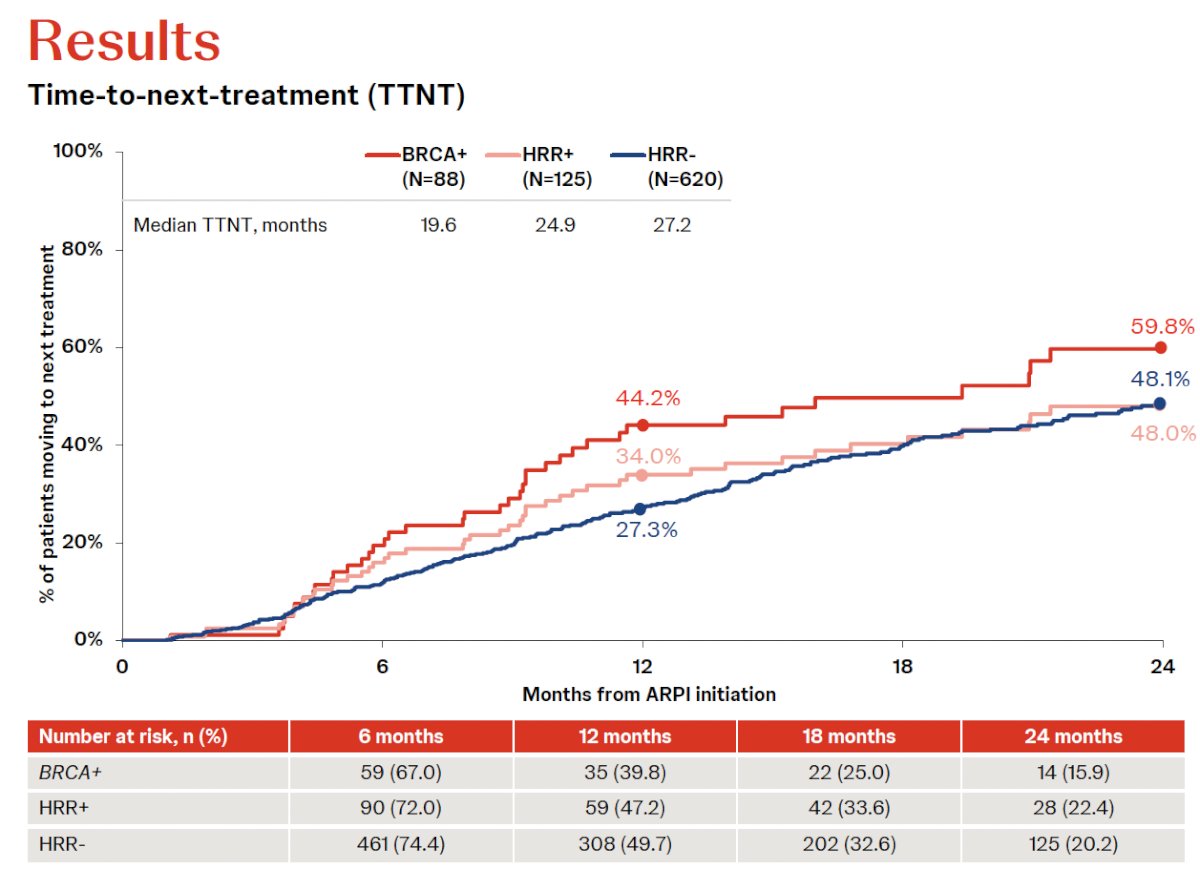
For TTCR, by 24 months, 56.4% of BRCA+ patients had progressed to castration resistance, which was a higher proportion relative to 49.7% of HRR+ patients and 46.7% of HRR- patients. BRCA+ patients had a median TTCR of 20.1 months, shorter relative to 24.7 months among HRR+ patients and 28.1 months among HRR- patients.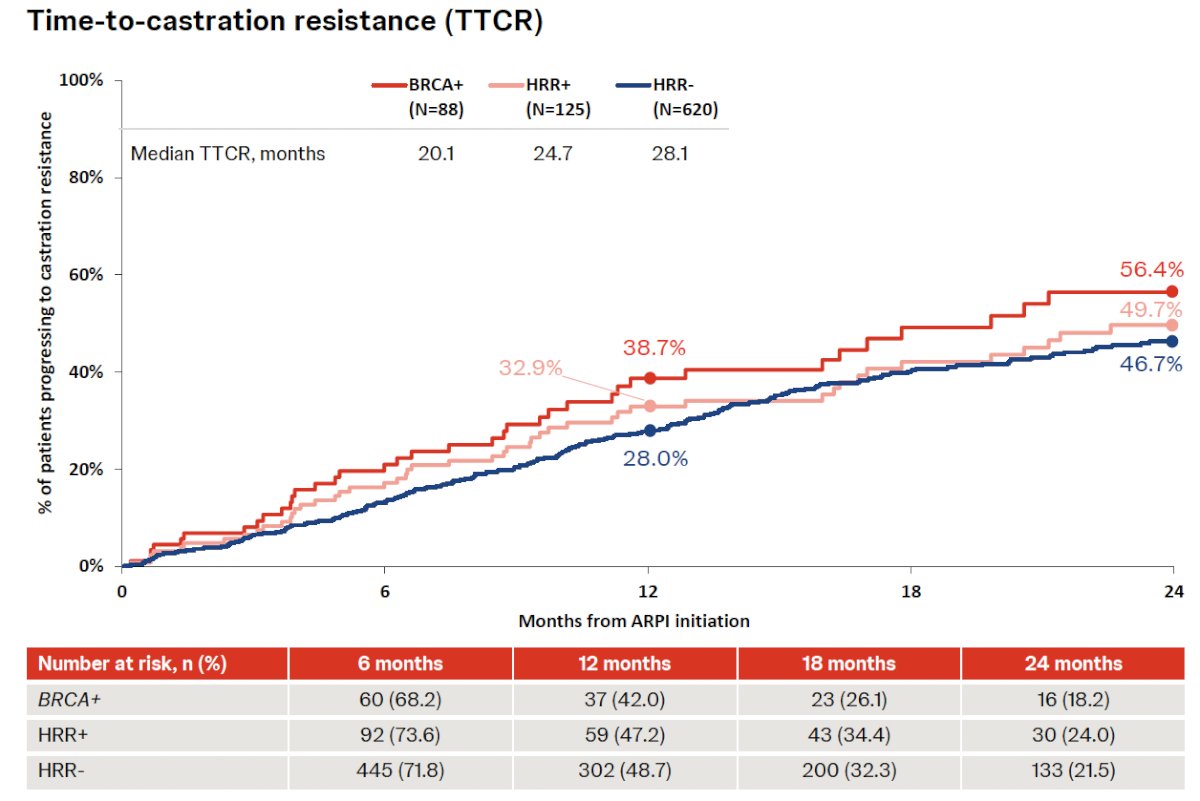
Dr. Shore concluded as follows:
- This retrospective study utilized real-world genomic data from a major oncology network in the US to evaluate clinical outcomes among patients with mCSPC tested for HRR mutations
- Among patients treated with an ARPI, those with BRCA1/2 mutations experienced faster progression to next treatment, and higher rates of progression to castration resistance
- These findings suggest that currently available treatments for mCSPC may be suboptimal for patients with BRCA mutations and highlight the need for novel therapies such as PARP inhibitors in the mCSPC setting
- These results support the need for ongoing clinical trials such as AMPLITUDE and TALAPRO-3 investigating the use of PARP inhibitors in HRR-positive mCSPC
Presented by: Neal Shore, MD, FACS, Director, CPI (Certified Principal Investigator by the Association of Clinical Research Professionals), Medical Director for the Carolina Urologic Research Center, AUC Urology Specialists, Myrtle Beach, South Carolina
Written by: Rashid K. Sayyid, MD, MSc – Robotic Urologic Oncology Fellow at The University of Southern California, @rksayyid on Twitter during the 2025 American Urological Association (AUA) annual meeting held in Las Vegas, NV, Saturday, April 26 - Tuesday, April 29, 2025
References:- Huang X, Chau CH, Figg WD. Challenges to improved therapeutics for metastatic castrate resistant prostate cancer: from recent successes and failures. J Hematol Oncol. 2012; 5:35.
- Leith A, et al. Real-world homologous recombination repair mutation testing in metastatic castration-resistant prostate cancer in the USA, Europe and Japan. Future Oncol. 2022; 18(8): 937-51.
- Rathkopf DE, et al. Final results from ACIS, a randomized, placebo-controlled, double-blind phase 3 study of apalutamide and abiraterone acetate plus prednisone versus abiraterone acetate plus prednisone in patients with chemotherapy-naive metastatic castration-resistant prostate cancer. J Clin Oncol. 2021; 39(6_suppl): Abstract 11.
- Agarwal N, et al. Emerging treatment strategies for metastatic prostate cancer: current perspectives and future directions. Future Oncology. 2024; 20(9): 493–505.