(UroToday.com) Dr. Colton K. Leavitt presented important findings addressing a long-standing procedural question in percutaneous nephrolithotomy (PCNL): is it safe to use water for irrigation instead of sterile saline? Current AUA guidelines mandate the use of sterile saline as opposed to water due to the risk of hyponatremia; however, surgeons have speculated that water might offer superior intraoperative visibility. This study aimed to determine whether using water during PCNL impacts patient outcomes, specifically regarding risks of hyponatremia and associated complications.
The research team conducted a retrospective cohort study analyzing adult patients undergoing PCNL, comparing outcomes between those who had procedures performed with water (n=82) and those with saline (n=18) as the irrigation fluid. The primary endpoint was the change in serum sodium levels from preoperative to postoperative measurements. Secondary outcomes included rates of hyponatremic events, hospital admission duration, ICU admissions, and emergency department (ED) visits within 14 days post-procedure.
The two groups were demographically similar. Preoperative sodium levels differed slightly (140 mEq/L in the water group vs. 138 mEq/L in the saline group), but postoperative sodium levels were identical (137 for the water group vs. 137.5 mEq/L for the saline group) (Figure 1).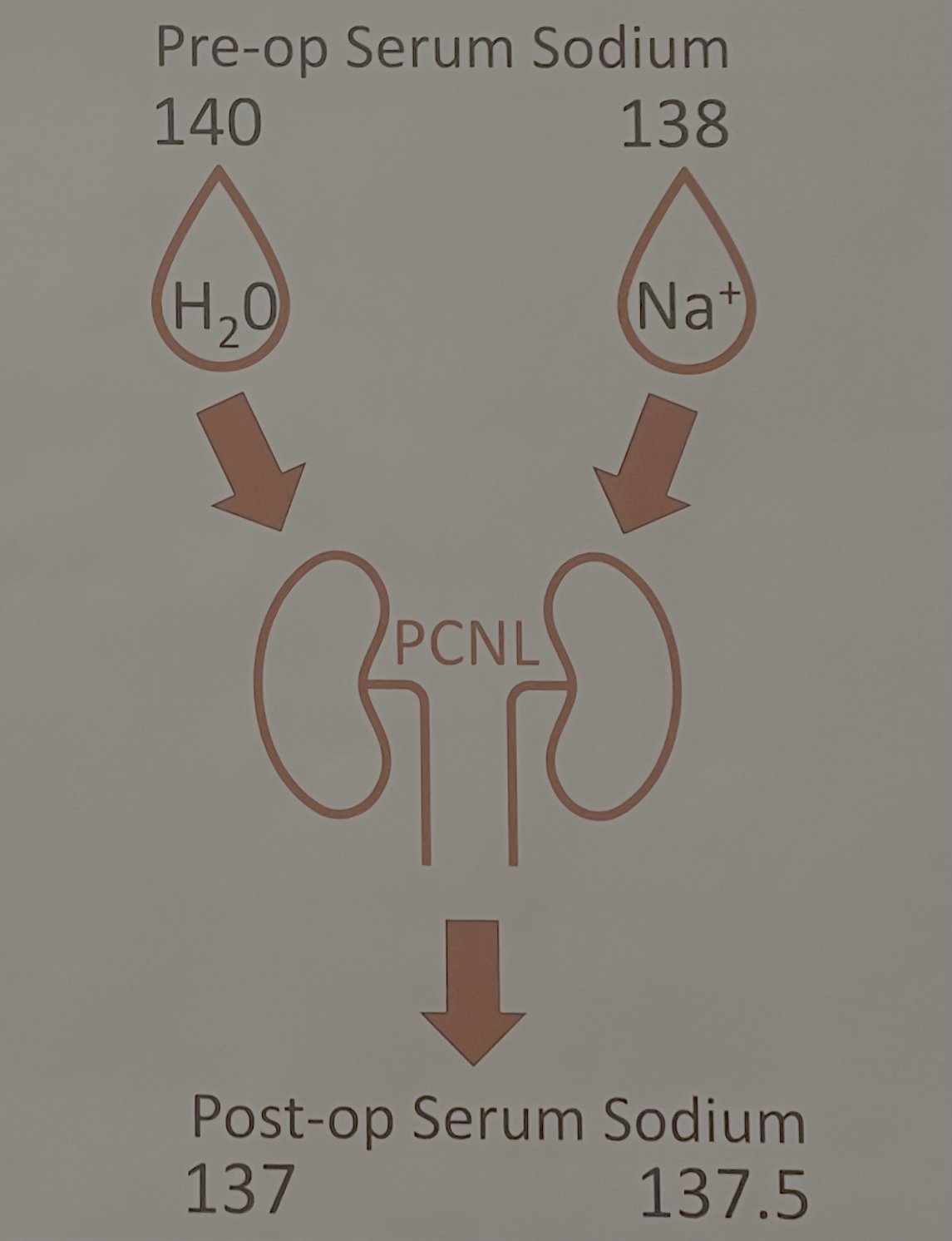
Figure 1: Comparison of preoperative and postoperative serum sodium levels.
Notably, no hyponatremic events were observed in either group. Similarly, no statistically significant differences were seen in hospitalization duration (25 vs. 27 hours), ICU admission rates (1.2% vs. 5.6%), or ED visits (15.9% vs. 11.1%) between the groups (Table 1)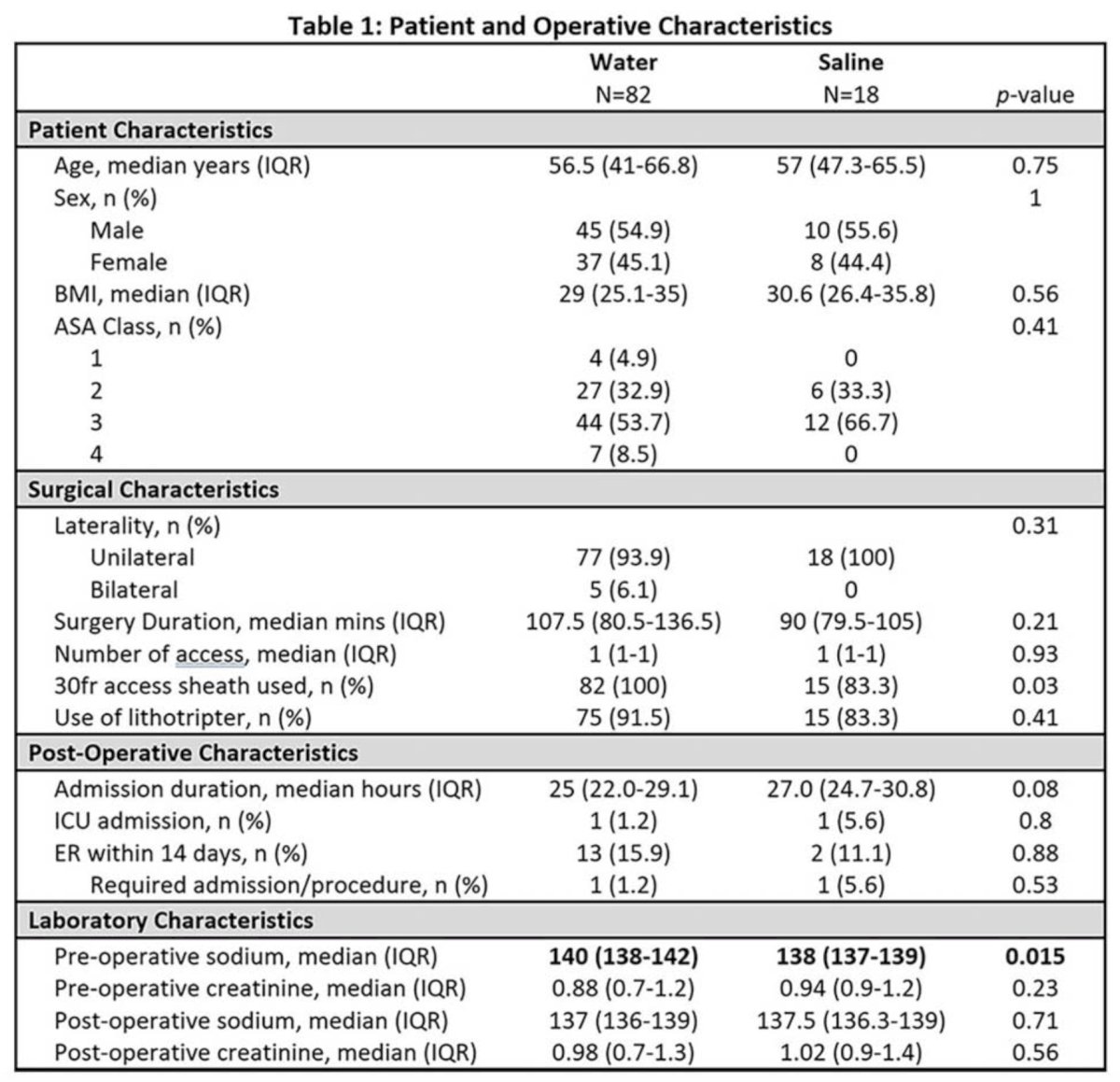
Using a multivariable linear regression model controlling for age, ASA score, surgical duration, and preoperative creatinine, the team found that irrigation with water resulted in a statistically significant decrease in serum sodium by 1.8 mEq/L compared to saline (p=0.006). However, this change was not deemed clinically meaningful. Additionally, surgery duration was associated with a minor decrease in sodium concentration (0.016 mEq/L per minute of operative time, p=0.014). There were no equity treatments events, no difference in admission duration, ICU admissions, or post-op ED visits (Table 2).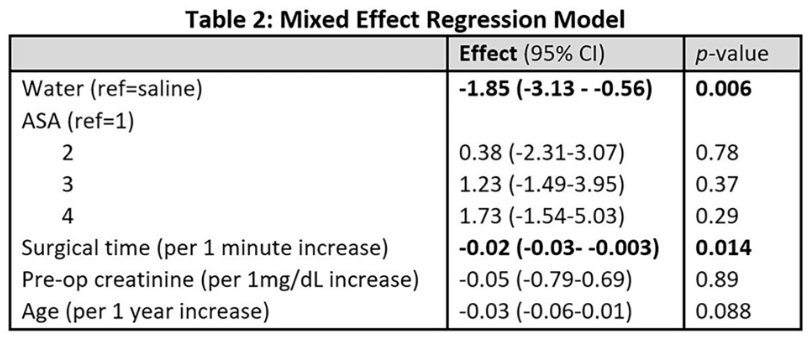
Dr. Leavitt concluded that water was H2-Okay! Indeed, while water irrigation results in a minor, statistically significant drop in serum sodium compared to saline, it does not lead to clinically meaningful hyponatremia or increased complication rates. These findings suggest that water can be considered a safe alternative to saline for irrigation during PCNL, potentially offering advantages such as improved visibility without compromising patient safety.
During the discussion session, several important questions were raised regarding the study.
Dr. Dendsted from the audience asked whether the study's conclusions might be affected by operative time, suggesting that longer surgeries could lead to greater fluid absorption. Dr. Leavitt responded that their multivariable model did show that longer operative times were associated with a slight decrease in serum sodium (approximately 0.0016 mEq/L per minute), but emphasized that while statistically measurable, the clinical relevance of this finding was minimal.
Dr. Molina then asked whether water irrigation offered any advantage with respect to stone-free rates (SFR). Dr. Leavitt clarified that the focus of this study was not on stone outcomes, but solely on the safety profile of using water versus saline. Another audience member asked if the study was prompted by the national fluid shortage. Dr. Leavitt explained that although water had already been used off-guideline at his institution, the saline shortage caused by flooding from Hurricane Helene and the subsequent closure of a major IV fluid production facility, prompted hospitals to impose stricter restrictions, providing an opportunity to formally evaluate and advocate for the safety of water in PCNL.
Finally, Dr. Bultitude from the moderator table questioned whether a cohort of 82 patients was sufficiently large. Dr. Leavitt stated that their team had calculated the study’s power based on the standard variance in sodium levels and determined that the sample size was adequate to detect even a five-point difference in serum sodium, supporting the robustness of their findings.
Presented by: Colton K. Leavitt, University of Utah during the 2025 American Urological Association (AUA) Annual Meeting, April 26-29, 2025, Las Vegas, Nevada
Co-Authors: Mira L. Reynolds, Joshua Horns, Stephen J. Summers, and Blake D. Hamilton
Moderated by: Matthew Bultitude (Guy's and St. Thomas' Hospital, London), Karthik Tanneru (Medical University of South Carolina (MUSC)), Mohamed Omar (Menoufia University)
Written by: Seyed Amiryaghoub M. Lavasani, B.A., University of California, Irvine, @amirlavasani_ on Twitter during the American Urological Association's 2025 Annual Meeting, between April 26 – 29, 2025 in Las Vegas, NV.