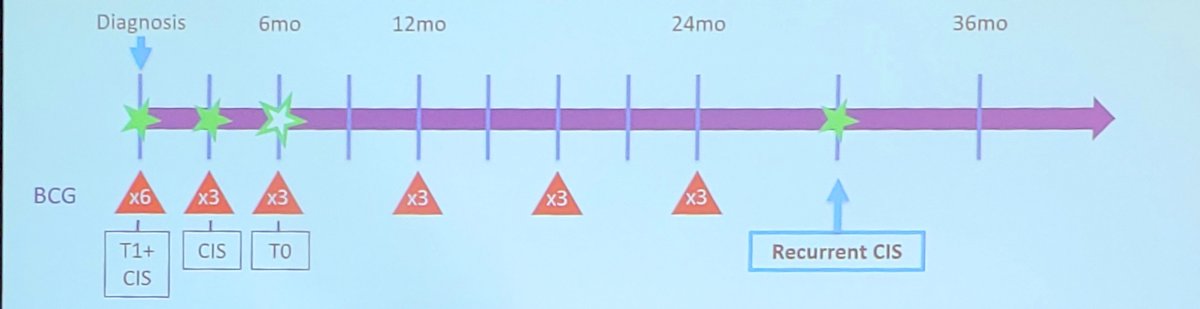
(UroToday.com) The 2025 AUA annual meeting featured the IBCG Bladder Cancer Forum evaluating common problems and controversies in bladder cancer, moderated by Dr. Peter Black, with a debate between Drs. Wes Kassouf and Michael O’Donnell discussing optimal treatment sequencing for patients with BCG unresponsive non muscle invasive bladder cancer who decline radical cystectomy. Dr. Black started the debate with a case presentation of a 67 year old male who presented with urinary urgency and frequency + microhematuria. A CT-IVP was normal, but cytology was suspicious for high grade urothelial carcinoma. Subsequent cystoscopy showed raised red areas on the posterior wall of the bladder, so the patient underwent a TURBT that demonstrated high grade T1 (focal invasion, no lymphovascular invasion, and no histologic subtypes). A re-TURBT showed no invasive cancer, however, there was CIS present. Given the above, the patient underwent treatment with 6 cycles of BCG induction therapy followed by re-evaluation at 3 months:
- Cytology was positive for high grade urothelial carcinoma
- Cystoscopy showed a red patch present at the prior location
- Office biopsy confirmed CIS
The decision was made to proceed with the first round of maintenance BCG, and at re-evaluation at 6 months, cytology, cystoscopy, and random biopsies were negative, so BCG maintenance was continued. As noted in the following figure, the patient eventually had an early relapse of CIS within 12 months of the last dose of BCG after a prior complete response:
Dr. Black then polled the audience based on the following question: “Assuming you have access to all treatment choices, what is your preferred second line treatment after BCG for patients with BCG unresponsive CIS?” The following were the options available:
- Radical cystectomy
- Intravesical gemcitabine + docetaxel
- A novel intravesical agent (ie. N-803 or nadofaragene firadenovec)
- Intravesical BCG
- Intravenous pembrolizumab
Dr. O’Donnell then discussed bladder sparing therapy with gemcitabine + docetaxel as an excellent first option for patients with BCG unresponsive CIS. To start, Dr. O’Donnell mentioned that among chemotherapies for BCG unresponsive CIS, by weighted means, gemcitabine + docetaxel has the most effective 12 month and 24 month disease free survival:

The 2006 AUA was the first time Dr. O’Donnell and his team reported sequencing of gemcitabine + mitomycin C, in which they concluded:
- Both treatment regimens were well tolerated
- There was occasional nausea attributed to gemcitabine
- There was moderate chemical cystitis attributed primarily to twice weekly gemcitabine and/or mitomycin C
- For gemcitabine + mitomycin C, the gemcitabine dose was reduced to 1 gm/50 cc once weekly x 6 + mitomycin C 40 mg/20cc
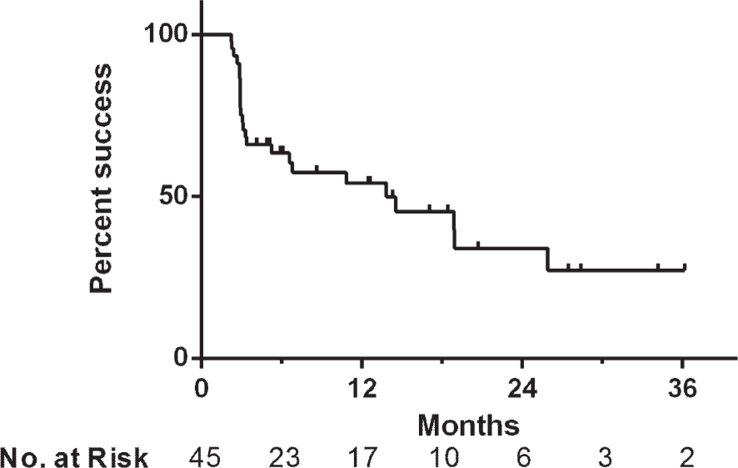
Ultimately, the first person was dosed with gemcitabine + docetaxel in July 2009 and the first series report was reported in 2015 based on the University of Iowa experience. Among 45 patients treated between June 2009 and May 2014, 9% were BCG naïve, 42% were BCG refractory, 40% were BCG relapsing, and 9% were BCG intolerant.1 The median follow-up was 15 months, with treatment success reported 66% at first surveillance, 54% at 1 year, and 34% at 2 years after initiating induction:
The Iowa experience was expanded to a multicenter analysis of 276 patients, including 38% of patients being BCG unresponsive.2 Over a median follow-up of 23 months, the 2 year outcomes:
- Recurrence free survival: 46%
- High grade recurrence free survival: 52%
- Cancer specific mortality: 4%
- Overall mortality: 13%
Looking at a regression analysis from the multi-institutional study, Dr. O’Donnell notes that only maintenance therapy significantly affected recurrence free survival, thus highlighting the importance of monthly maintenance therapy after induction gemcitabine + docetaxel.
Dr. O’Donnell then highlighted the external validation for gemcitabine + docetaxel in BCG failures at Brigham and Women’s hospital and Mass General Hospital.3 Among 102 patients with BCG-unresponsive disease, the 6-, 12-, and 24-month high-grade recurrence-free survival rates were 78%, 65%, and 49%, respectively. Overall, 20 patients underwent radical cystectomy (median 15.5 months from induction), and 6 patients progressed to muscle invasive disease. Patients with BCG refractory disease were more likely to develop high grade recurrence when compared to patients with BCG relapsing disease (HR 2.14; 95% CI 1.02-4.49).
Dr. O’Donnell’s group published their long term gemcitabine + docetaxel for BCG non muscle invasive bladder cancer in 2023.4 Among 97 patients with a median follow-up of 49 months, 71% of the cohort had CIS containing disease, and 35% of the cohort had BCG-unresponsive disease. They noted that complete response at 3-month surveillance was 74%, and the median duration of response was 25 months. At 1, 2, and 5 years, high grade recurrence free survival was 60%, 50%, and 30%, respectively. High grade recurrence free survival was similar among BCG-unresponsive patients and the overall cohort. During follow-up, 20 patients underwent cystectomy, and 15 patients experienced disease progression. Notably, the 5-year progression free survival rate was 82%.
For BCG treated high risk disease, Dr. O’Donnell discussed a multicenter experience of 299 patients with a median follow-up of 40 months.5 Of these patients, 95 were treated with gemcitabine + docetaxel, reporting a 1 year high grade recurrence free survival rate of 74%, and a 1 year progression free survival rate of 96%. Of note, receipt of further BCG was associated with a higher progression risk (HR 2.6):

Dr. O’Donnell concluded his portion of the debate by highlighting the comparative efficacy of new agents for BCG unresponsive CIS:

Dr. Kassouf then made the case for BCG unresponsive CIS in a patient with a good functioning bladder. The novel option he discussed was N-803 + BCG, which was FDA approved in 2024. In this combination, there is a synergistic mechanism of action of BCG (priming) + N-803 (boosting) to induce innate immune memory with a prolonged duration of response:

N-803 is an IL-15 super agonist that forms a mutant IL-15 based immunostimulatory fusion protein complex from IL-15 agonism. It promotes proliferation and activation of natural killer cells and CD8+ T cells, thereby increasing the efficacy of BCG and cancer cell death. N-803 is given intravesically with an additional BCG course (weekly for 6 weeks), augmenting the immune response to BCG.
QUILT-3.0326 is an ongoing, open label, multicenter, single arm trial that is evaluating intravesical N-803 + BCG or N-803 alone in patients with BCG-unresponsive, high-grade non muscle invasive bladder cancer. This study includes three patient cohorts:
- Cohort A (CIS +/- papillary disease): Intravesical N-803 (400 μg/instillation) + BCG (50 mg/instillation) given once weekly for 6 consecutive weeks (induction)
- Cohort B (High grade Ta/T1 papillary disease): N-803 + BCG
- Cohort C (CIS +/- papillary): N-803 alone
In Cohort A, a complete response was observed in 71% of patients (13/58 responders required a re-induction), with the following summary of clinically meaningful efficacy results:

The median duration of response in complete responders in Cohort A was 26.6 months (95% CI 9.9% to NR), and the duration of complete response >= 12 months was 61.6% (95% CI 47.3 to 73.1%)

Re-induction therapy in 24 (29%) patients had a complete response rate of 54%. Additionally, the 24 month disease free survival rate was 48.3%. The most common treatment-related adverse events with the combination of N-803 + BCG were lower genitourinary in nature (dysuria, pollakiuria, hematuria). The incidence of grade 3 or worse adverse events was 23%, most frequently hematuria and urinary tract infections (2% each). One patient experienced a grade 5 treatment-related adverse event (cardiac arrest with subsequent death), and 3 had evidence of immune-related adverse events:

Of note, updated data from QUILT-3.032 were presented by Dr. Sam Chang at AUA 2025.
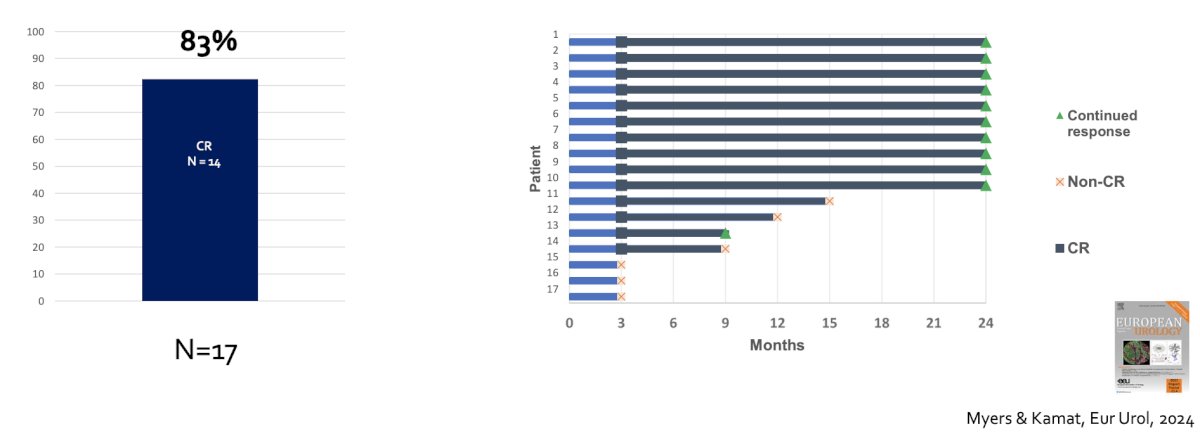
Dr. Kassouf then discussed work from Dr. Kamat’s group showing that a sub-population of patients that have BCG-unresponsive CIS +/- Ta/T1 may have a response to additional BCG.7 Among 17 patients receiving additional BCG, 14 (83%) had a complete response:
With regards to the counter argument of gemcitabine + docetaxel, in the multicenter validation study,2 Dr. Kassouf highlighted the following points:
- This was a retrospective study across 10 centers, thus, this is not prospective data
- The majority (62%) were not BCG unresponsive patients, and there was no mandatory biopsy
- 9.4% of patients were intolerant or had symptoms that impacted the treatment schedule
Additional points regarding gemcitabine + docetaxel provided by Dr. Kassouf include:
- This is a heterogeneous patient population: a mix of BCG naïve, BCG relapse, and BCG unresponsiveness, with various follow-up regimens and no mandatory biopsy
- The BCG unresponsive subset is low in these studies (<30-50 patients); thus, gemcitabine + docetaxel has been assessed in “lower risk” BCG unresponsive patients
- Maintenance is critical for efficacy: Tolerance decreases with maintenance therapy
Dr. Kassouf concluded his portion of the debate for alternative regimens, in particular N-803 + BCG with the following messages:
- There is a strong biological rationale for N-803 + BCG
- It maintains BCG as a backbone therapy
- It is well tolerated in patients with a good functioning bladder
- It has been tested in a prospective trial with a higher length of evaluation, showing efficacy and durability
The debate concluded by highlighting the pre- and post-debate answers to the polling question “Assuming you have access to all treatment choices, what is your preferred second line treatment after BCG for patient with BCG unresponsive CIS?”
- Radical cystectomy
- Pre-debate: 23%
- Post-debate: 11%
- Intravesical gemcitabine + docetaxel
- Pre-debate: 51%
- Post-debate: 73%
- A novel intravesical agent (ie. N-803 or nadofaragene firadenovec)
- Pre-debate: 22%
- Post-debate: 14%
- Intravesical BCG
- Pre-debate: 4%
- Post-debate: 2%
- Intravenous pembrolizumab
- Pre-debate: 0%
- Post-debate: 0%
Presented by:
- Wes Kassouf, McGill, MD, University Health Center, Montreal, Quebec, Canada
- Michael O’Donnell, MD, University of Iowa Hospitals and Clinics, Iowa City, IA
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2025 American Urological Association (AUA) annual meeting held in Las Vegas, NV, Saturday, April 26 - Tuesday, April 29, 2025
References:
- Steinberg RL, Thomas LJ, O’Donnell MA, et al. Sequential intravesical gemcitabine and docetaxel for the salvage treatment of non-muscle invasive bladder cancer. Bladder Cancer. 2015 Apr 30;1(1):65-72.
- Steinberg RL, Thomas LJ, Brooks N, et al. Multi-Institution Evaluation of Sequential Gemcitabine and Docetaxel as Rescue Therapy for Nonmuscle Invasive Bladder Cancer. J Urol. 2020 May;203(5):902-909.
- Yim, K, Melnick K, Mott SL, et al. Sequential intravesical gemcitabine + docetaxel provides a durable remission in recurrent high-risk non muscle invasive bladder cancer following BCG therapy. Urol Oncol. 2023 Nov;41(11):458.e1458.e7.
- Chevuru PT, McElree IM, Mott SM, et al. Long-term follow-up of a sequential intravesical gemcitabine and docetaxel salvage therapy for non-muscle invasive bladder cancer. Urol Oncol. 2023 Mar;41(3):148.e1-148.e7.
- Taylor J, Kamat AM, Annapureddy D, et al. Oncologic outcomes of sequential intravesical gemcitabine and docetaxel compared with Bacillus Calmette-Guerin in patients with Bacillus Calmette-Guerin-unresponsive non-muscle invasive bladder cancer. Eur Urol Oncol. 2025 Apr;8(2):469-476.
- Chamie K, Chang SS, Kramolowsky E, et al. IL-15 Superagonist NAI in BCG-Unresponsive Non-Muscle-Invasive Bladder Cancer. NEJM Evid 2022; 2(1)
- Myers AA, Tan WS, Grajales V, et al. Challenging the paradigm of “BCG-unresponsive” Bladder Cancer: Does Additional Bacillus Calmette-Guerin have an effect? Eur Urol. 2024 Oct;86(4):366-368.