(UroToday.com) The American Urologic Association (AUA) 2025 Annual Meeting held in Las Vegas, NV between April 26th and 29th, 2025 was host to a bladder cancer clinical trials in progress session. Mark Tyson, MD, MPH, presented BOND-003 Cohort P, a multinational, single arm study of intravesical Cretostimogene Grenadenorepvec for the treatment of BCG-unresponsive, high-risk, papillary-only non-muscle invasive bladder cancer (NMIBC).
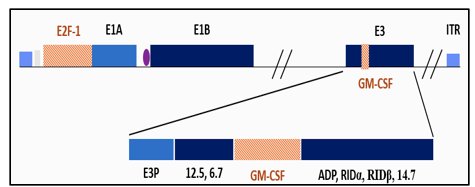
What is cretostimogene grenadenorepvec (CG)? It is an oncolytic immunotherapy with a dual mechanism of action. It binds to the Coxsackie Adenovirus Receptor (CAR) & integrin αvβ5, which is highly expressed in all stages of bladder cancer. It is a conditionally replicating, highly immunogenic adenovirus under the regulation of the human E2F-1 promoter, selective for RB-E2F pathway alterations, and encodes the GM-CSF transgene.
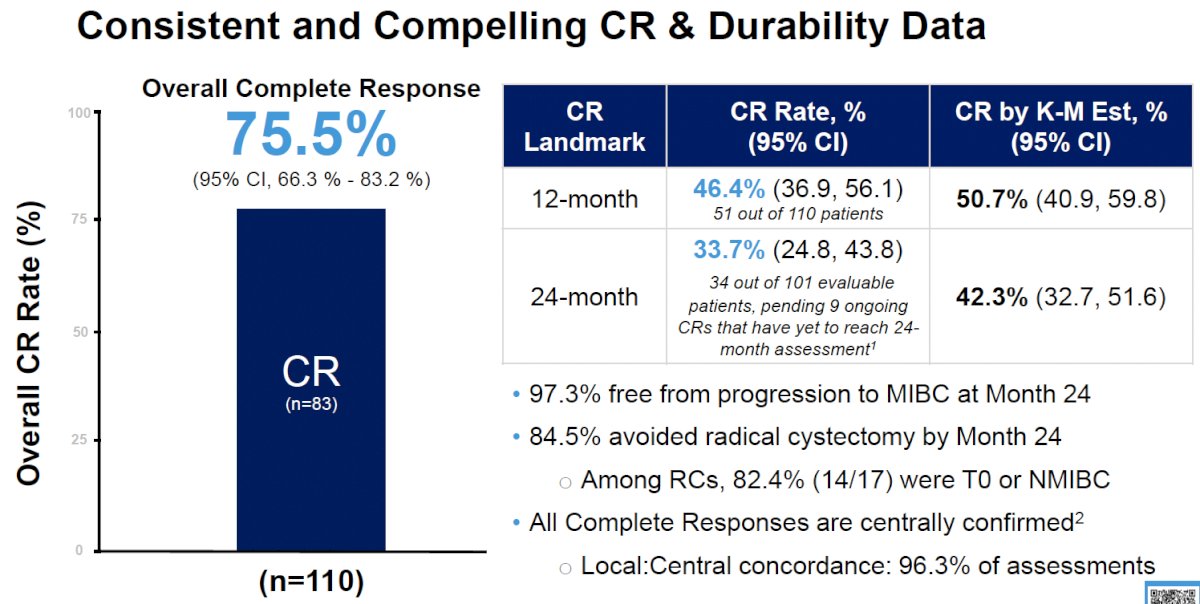
Existing data support the efficacy and durability of response with CG therapy. BOND-003 Cohort C evaluated CG in patients with high-risk, BCG-unresponsive NMIBC with CIS and demonstrated the following results:1
- Overall complete response: 75.5%
- 12-months complete response: 46.4%
- 24-months complete response: 33.7%
- 97.3% were free from progression to MIBC at 24 months
- 84.5% avoided radical cystectomy within 24 months
- Among radical cystectomy patients, 82.4% (14/17) were T0 or had NMIBC
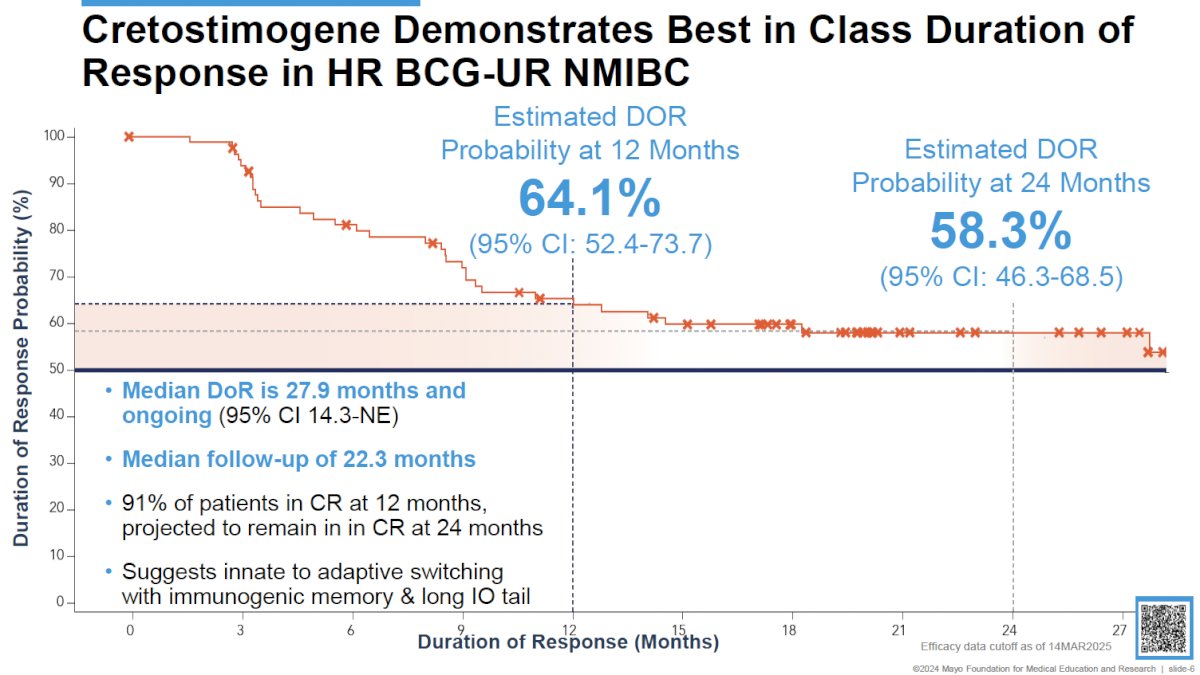
Among complete responders, 64.1% maintained their response by 12 months, with durable long-term responses, as reflected by the 24 months-maintained response rate of 58.3%. The median duration of response is 27.9 months and ongoing.
CG is well-tolerated with a favorable safety profile. No grade ≥3 treatment-related adverse events (TRAEs) or deaths were observed, and the median time to TRAE resolution was 1 day. No treatment-related discontinuations have been observed with CG, and 97.3% of eligible patients received all protocol-defined treatments.1
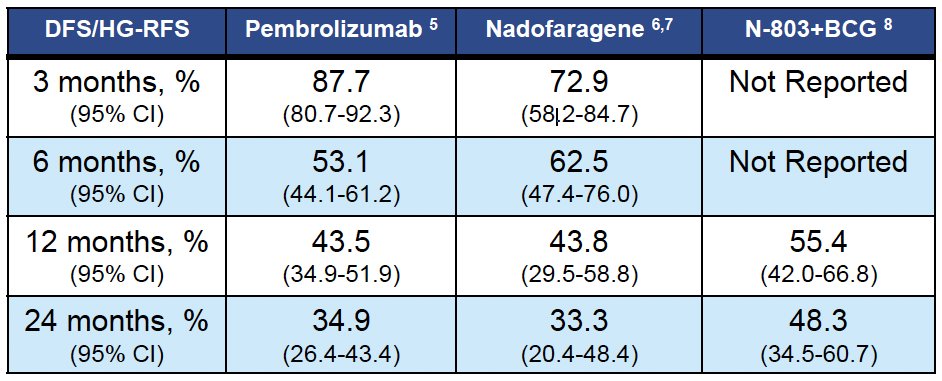
Dr. Tyson noted that there remains a significant unmet need for clinically effective and well-tolerated bladder-sparing treatment options for the BCG-unresponsive, papillary-only NMIBC population. Current FDA approved agents for patients with high-risk, BCG-unresponsive NMIBC are for those with CIS +/- Ta/T1 disease. There is a growing incidence of patients with papillary NMIBC, and current treatments offer modest improvements over the FDA benchmark.
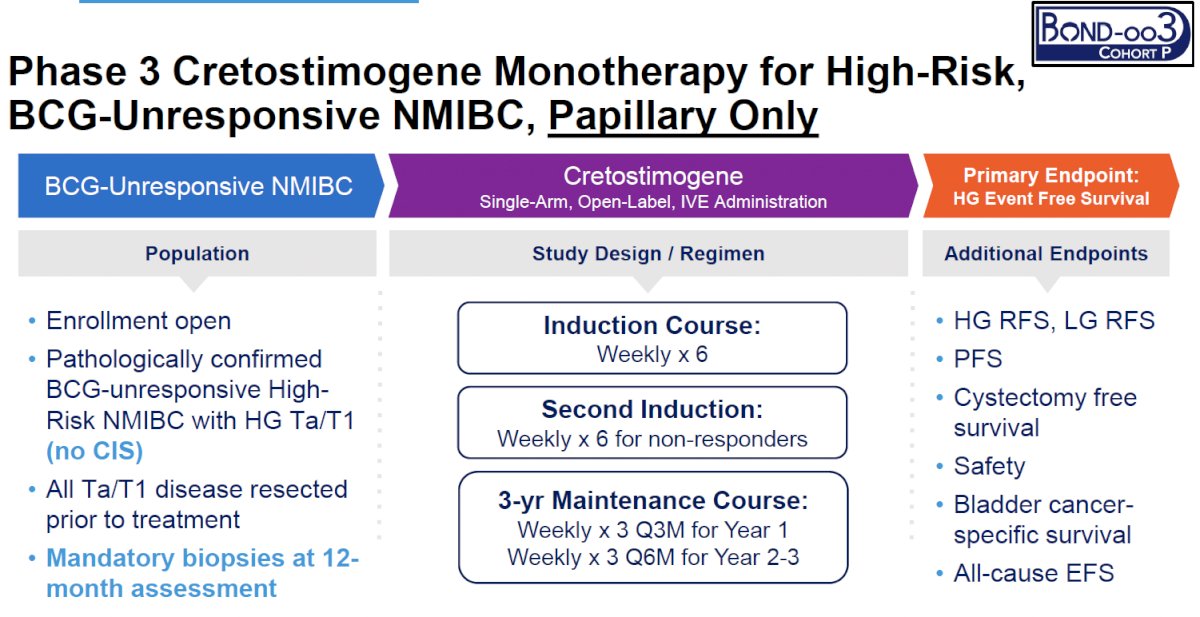
BOND-003 Cohort P will evaluate cretostimogene monotherapy for papillary-only, high-risk BCG-unresponsive NMIBC. The study inclusion criteria are as follows:
- Pathologically confirmed BCG-unresponsive, high-risk NMIBC with HG Ta/T1 (no CIS)
- All Ta/T1 disease resected prior to treatment
- Mandatory biopsies at 12-month assessment
Patients will receive a 6-week induction course, with a second induction course allowed for non-responders. A 3-year maintenance course is planned for responders. The primary endpoint is high-grade event-free survival, with key secondary endpoints including:
- High- and low-grade recurrence-free survivals
- Progression-free survival
- Cystectomy-free survival
- Safety
- Bladder cancer-specific survival
- All-cause event-free survival
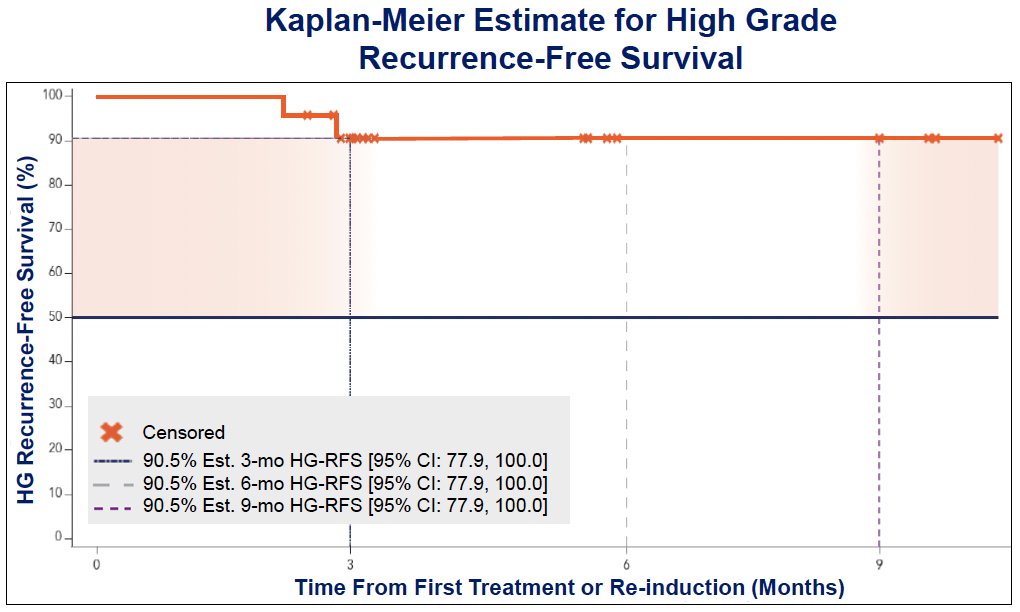
Dr. Tyson presented the initial results from the first 24 treated patients. The 3- and 9-months high-grade recurrence-free survival rates (primary endpoint) were 90.5%. This regimen was very well-tolerated with no treatment-related serious adverse events and no treatment discontinuations.
This trial is currently ongoing with the 1st sites opened and patients enrolled in March 2024. There are currently >35 sites across North America and Japan.

Presented by: Mark Tyson, MD, MPH, Associate Professor, Department of Urology, Mayo Clinic, Phoenix, AZ
Written by: Rashid K. Sayyid, MD, MSc – Robotic Urologic Oncology Fellow at The University of Southern California, @rksayyid on Twitter during the 2025 American Urological Association (AUA) annual meeting held in Las Vegas, NV, Saturday, April 26 - Tuesday, April 29, 2025
Related content: BOND-003 Cohort P Results for BCG-Unresponsive Papillary Bladder Tumors - Mark Tyson
References:
- Tyson MD, Bivalacqua TJ, Steinberg GD, et al. Final results of BOND-003 Cohort C: A phase 3, single-arm study of intravesical cretostimogene grenadenorepvec for high-risk BCG-unresponsive non-muscle invasive bladder cancer with carcinoma in situ. J Urol. 2025; 193(4): 1010–1018.