(UroToday.com) Dr. Lynn Stothers introduced a novel, transcutaneous optical monitoring system designed to track bladder volume and pressure in patients with neurogenic lower urinary tract dysfunction (NLUTD) secondary to spinal cord injury (SCI). This wearable system, developed in collaboration with Dr. Andrew Macnab (Vancouver, Canada), aims to improve symptoms by reducing incontinence and lowering the risk of autonomic dysreflexia (AD), related to bladder distention.
Dr. Stothers' group has previously demonstrated through 24-hour home bladder pressure monitoring that bladder-related events, such as overdistention and incontinence, are the leading triggers for both symptomatic and silent autonomic dysreflexia (AD) in SCI patients. They also found that bladder oximetry, utilizing near-infrared light, correlates with changes in detrusor pressure during urodynamic studies (UDS). In this continued investigation, they hypothesized that a wearable device incorporating near-infrared light-emitting diodes (LEDs) could be engineered to non-invasively monitor both bladder volume and detrusor pressure.
Two major study objectives were outlined: 1) primary outcomes related to engineering a functional device and 2) surveying the SCI community to assess their preferences for hardware and software features of a home bladder monitoring system.
The newly developed optical interface, based on near-infrared spectroscopy (NIRS), offers a self-contained, wireless, and suprapubically applied sensor. Light absorption was measured at three wavelengths: 950 nm for water detection and 760/850 nm for oxygenated and deoxygenated hemoglobin, capturing dynamic changes in bladder content and detrusor perfusion (Figure 1)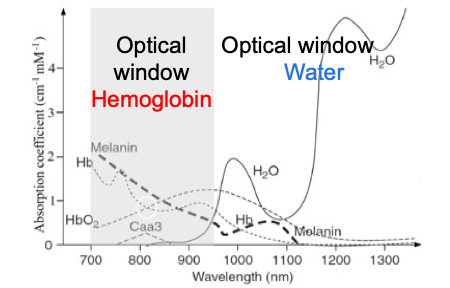
Figure 1: Infrared light absorption detecting water and oxygenated/deoxygenated hemoglobin on the wearable device.
The device is embedded in a soft, latex-free silicone sheet with a 10 x 10 cm optical grid. It contains paired emitter-detector arrays spaced 4 cm apart to track changes at two vertical levels of the bladder wall (Figure 2). LEDs operate between 750-950 nm and allow for both superficial (short) and deep (long) channel measurements at a sampling rate of 50 Hz. Wireless data collection is supported with a battery life of 8-24 hours, and the flexible housing is designed to contour comfortably to the skin surface.
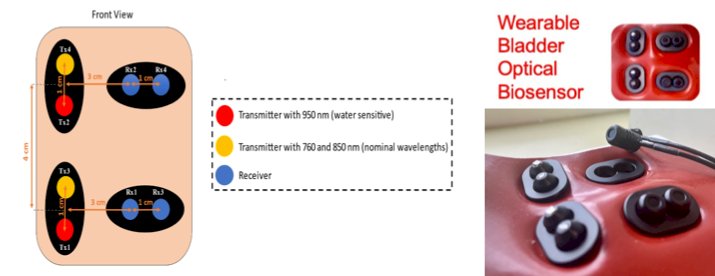
Figure 2: Technical design and prototype of the wearable device.
Among a cohort of 66 individuals with SCI >1 year post injury (41% ASIA A males; 33% ASIA A females) undergoing UDS, 26 were managed with clean intermittent catheterization (CIC) and spontaneous voiding, 20 via spontaneous voiding or Credé technique, 15 CIC-only, and 5 with condom drainage. The control group included 15 patients. During the clinical evaluation, the team monitored natural bladder filling across various postures and performed simultaneous UDS in SCI patients to validate the NIRS data. Optical density and chromophore concentration changes were compared between the two arrays at two levels (low and mid-point) during bladder filling.
Optical density changes from baseline were successfully tracked across bladder filling stages. At lower volumes (<250 mL), water signal attenuation was first detected by the lower array, while at higher volumes (>300 mL), the upper sensor reflected greater attenuation, clearly distinguishing between stages of bladder filling (Figure 3). With respect to bladder pressure, oximetry of hemoglobin (of the anterior bladder wall) and the configuration of the arterial wave were analyzed (Figure 4).

Figure 3: Water signal optical densities at low volume (left) and higher bladder volume (right) at capacity, with changes now detected by upper array.

Figure 4: Hemoglobin concentration changes detected by near-infrared spectroscopy during natural bladder filling.
Derived from hemoglobin signals, three algorithms were developed to correlate with detrusor pressure: Chromophore Total (blood volume), Oxygenated Hemoglobin (O₂Hb), and Hemoglobin Difference (Hb Diff). Ultimately, Hb Diff was the best-fit algorithm for UDS detrusor pressure, demonstrating predictive accuracy for detrusor pressure (Pdet) in 74% of subjects (Figure 5). Additionally, in 20% of SCI patients, autonomic dysreflexia occurred during UDS, further emphasizing the need for continuous, preventative monitoring.

Figure 5: Overlaid dataset of a T10 ASIA B male of the wearable bladder optical biosensor and simultaneous UDS output, with noted neurogenic detrusor overactivity (NDO), with resultant relationship to Pdet.
An end-user survey was conducted among participants, revealing that 90% were willing to wear a bladder monitor even if it slightly restricted movement. Participants showed a split preference between securing the device with medical adhesive or a strap and tolerated up to 15 minutes of daily preparation time. There was strong interest in device tethering to a cellphone or smartwatch, with a preference for haptic (vibrational) alerts over auditory signals.
In conclusion, Dr. Stothers stated that this wearable, transcutaneous system demonstrates feasibility for monitoring bladder function in SCI populations. Future directions include evaluating whether home monitoring with the optical device can improve quality of life and possibly reduce the frequency of events triggering AD.
During the discussion, Dr. Margot Damaser raised two important questions regarding the resolution and accuracy of the wearable optical device. First, she noted that arterial pulse waveforms, commonly detected by wearable devices like smartwatches, are difficult to measure in SCI patients due to their lower baseline blood pressure. In response, Dr. Stothers explained that although arterial signals are currently challenging to detect, the team now has a functioning prototype, and future iterations of the device may expand to address this limitation. Second, Dr. Damaser inquired whether the device measures abdominal pressure. Dr. Stothers clarified that the current focus is on detecting neurovascular responses rather than direct abdominal pressure, but acknowledged that future advancements combining multiple technologies may allow for broader physiological monitoring, including vascular responses.
Lastly, another audience member remarked that the "holy grail" of UDS is achieving simultaneous, non-invasive measurement of both bladder volume and pressure. Dr. Stothers responded that while volume is comparatively easier to detect using light absorption, as bladder filling results in sequential, measurable changes in optical signals, accurately measuring pressure remains more complex. She likened the optical detection of bladder filling to a "fuel gauge," where absorbed light signals gradually change as volume increases. In conclusion, she emphasized that detecting bladder volume is currently more straightforward than pressure with this system.
Presented by: Lynn Stothers, University of California, Los Angeles, during the 2025 American Urological Association (AUA) Annual Meeting, April 26-29, 2025, Las Vegas, Nevada
Co-Authors: Andrew Macnab
Moderated by: E. Ann Gormley (Dartmouth Hitchcock Clinic), Jang Hwan Kim (Yonsei University), Patrick Shenot (Thomas Jefferson University)
Written by: Seyed Amiryaghoub M. Lavasani, B.A., University of California, Irvine, @amirlavasani_ on Twitter during the American Urological Association's 2025 Annual Meeting, between April 26 – 29, 2025 in Las Vegas, NV.