(UroToday.com) The 2024 American Urological Association (AUA) Annual Meeting held in San Antonio, TX was host to the International Prostate Forum. Dr. Adam Weiner presented the latest advances in the prevention, diagnostic, and surgical applications of prostate-specific membrane antigen (PSMA) positron emission tomography (PET) in prostate cancer.
There have been numerous studies published demonstrating that MRI-guided biopsy pathways can increase the yield of Grade Group ≥2 prostate cancer and reduce Grade Group 1 detection, compared to a systematic biopsy approach. In the PRECISION trial, men with a clinical suspicion of prostate cancer who had not previously undergone a prostate biopsy were randomized to undergo MRI, with or without targeted biopsy, or standard transrectal ultrasonography–guided biopsy. Men in the MRI-targeted biopsy group underwent a targeted biopsy (without standard biopsy cores) if the MRI was suggestive of prostate cancer; men whose MRI results were not suggestive of prostate cancer were not offered biopsy. Standard biopsy was a 10-to-12–core, transrectal ultrasonography–guided biopsy.
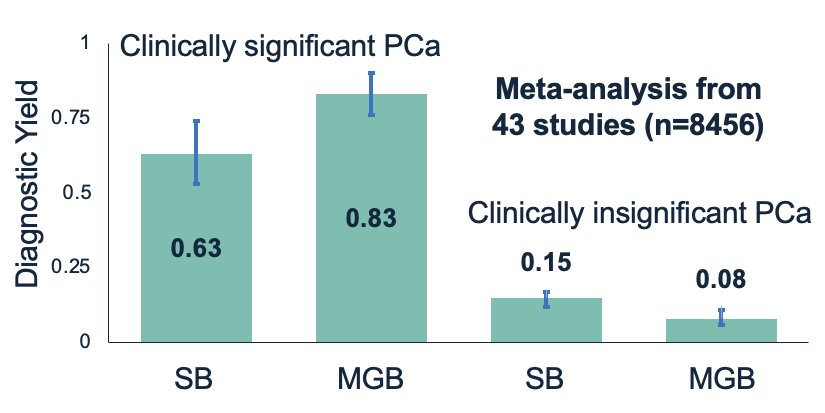
Men in the MRI group had increased detection of Grade Group ≥2 disease (38% versus 26%) with lower detection of Grade Group 1 disease (22% versus 9%). Notably, 28% of men avoided a biopsy with MRI, and a median of only 4 cores was obtained with such a targeted approach.1 These findings are supported by those from a 2022 meta-analysis of 43 studies that demonstrated that MRI-guided biopsy improves the yield for clinically significant prostate cancer by ~32% while decreasing the detection of clinically insignificant disease by 47%.2
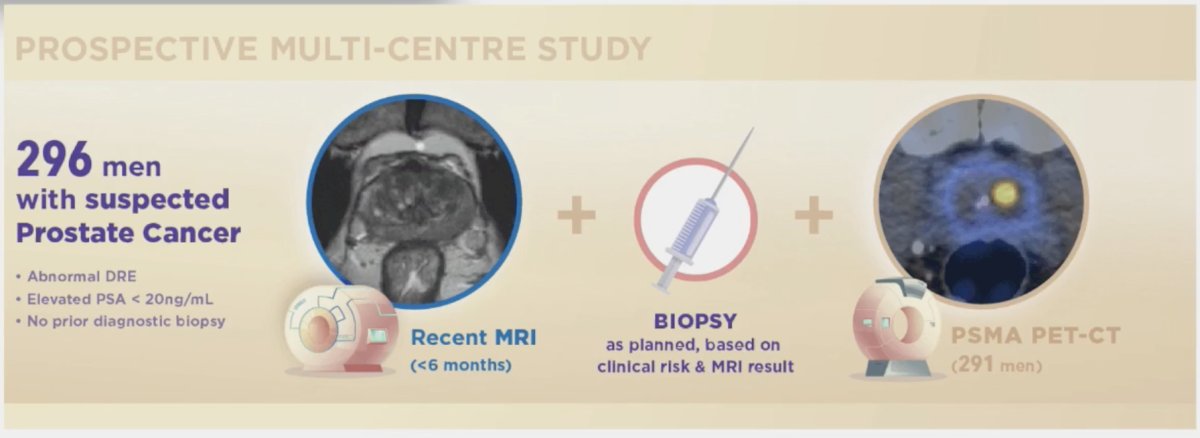
The utility of PSMA-PET/CT has recently been evaluated in the diagnostic (i.e., primary) setting in the Australian PRIMARY trial (NZCTRN12618001640291). This is a multicenter, phase II imaging trial that evaluated if a limited (i.e. pelvic-only) 68Ga-PSMA-11 PET/CT in combination with mpMRI can reliably discriminate men with clinically significant prostate cancer (i.e. Grade Group ≥2) from those without clinically significant disease. This trial included 296 men (291 eligible) with suspected prostate cancer (PSA<20), no previous biopsy, recent MRI within 6 months, and planned transperineal biopsy based on clinical risk and MRI. For analysis, the combination of PSMA and MRI was considered negative for those with PSMA negative findings with PI-RADS 2/3 findings and conversely positive for those with either PSMA positive or PI-RADS 4/5 lesions.
Of these 291 men, 162 (56%) had clinically significant prostate cancer. MRI, PSMA, and PSMA+MRI was positive in 67%, 73%, and 81% of patients, respectively. Combination PSMA and MRI, compared to MRI alone, improved the sensitivity (97% versus 83%, p<0.001) and NPV (91% versus 72%, p<0.001). However, this was at the cost of reduced specificity (40% versus 53%, p=0.001). Among all 291 patients, 56 (19%) were both PSMA and MRI negative and could have potentially avoided a biopsy at a risk of delayed clinically significant prostate cancer detection of 3.1%.3
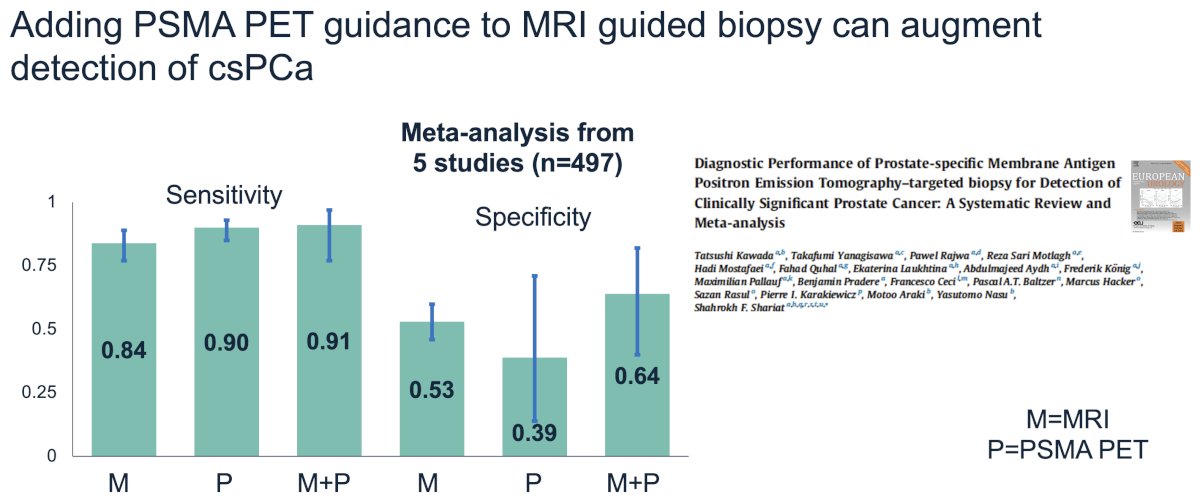
A 2022 systematic review and meta-analysis of 5 studies demonstrated that the addition of PSMA-PET to MRI can improve the sensitivity of MRI alone for the detection of clinically significant prostate cancer from 84% to 91% and the specificity from 53% to 64%.4
What about the utility of PSMA-PET in the biopsy negative setting? In 2017, Simopoulos et al. published a case report of a 71-year-old male with a PSA of 49 ng/ml who had six prior negative MRI-guided biopsies. PSMA-PET/US fusion-guided biopsy demonstrated Grade Group 2 prostate cancer, which was confirmed on the radical prostatectomy specimen.5 Since then, there have been numerous studies that have evaluated the utility of PSMA-PET in this setting. At AUA 2024, Brisbane et al. presented the results of an ongoing trial (NCT05160597) that demonstrated clinically significant disease in 10/25 (40%) patients with a prior negative/inconclusive biopsy.
What about PSMA-PET for the initial staging of intermediate/high-risk patients? Published in 2020, proPSMA is a multi-center, two-arm randomized controlled trial of men with histologically confirmed prostate cancer who were being considered for curative intent radical prostatectomy or radiotherapy. To be eligible for inclusion, men must have had ≥1 high-risk factor including PSA ≥ 20 ng/mL, ISUP grade group 3-5, or clinical stage T3 or greater. Following enrollment, patients were randomly assigned in a 1:1 ratio to either conventional imaging consisting of bone scan and CT, or 68Ga-PSMA-11 PET/CT. PSMA PET/CT had a 27% absolute greater area-under-the-curve (AUC) for accuracy compared to conventional imaging (92% versus 65%). Conventional imaging had both a lower sensitivity (38% vs. 85%) and specificity (91% vs. 98%). Subgroup analyses by site of metastasis demonstrated the superiority of PSMA PET/CT for pelvic nodal (AUC: 91% versus 59%) and distant metastases (AUC: 95% versus 74%).6

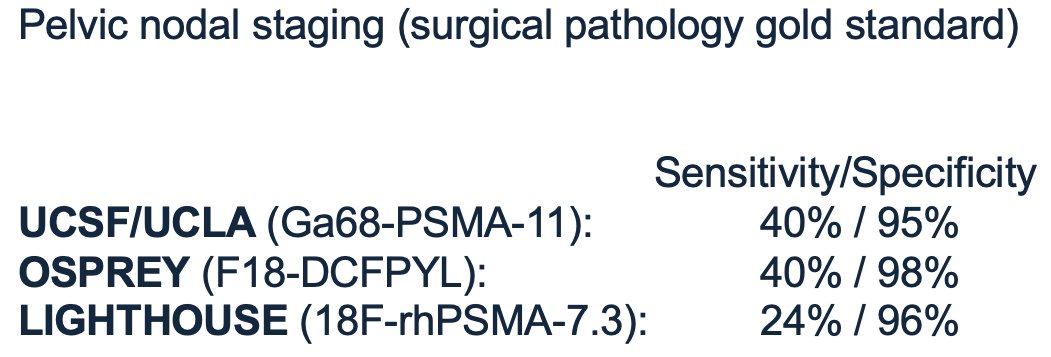
What is the performance of PSMA-PET for pelvic nodal staging? Ideally, this imaging test would help rule out patients with minimal risk of pelvic nodal disease, which in turn would spare them the morbidity of a pelvic lymph node dissection at the time of a radical prostatectomy. This test would thus require a high sensitivity (i.e., high negative predictive value) in this setting. It appears that the sensitivity of PSMA-PET/CT remains approximately 24–40%, although this value varies by the patient’s underlying disease risk status.
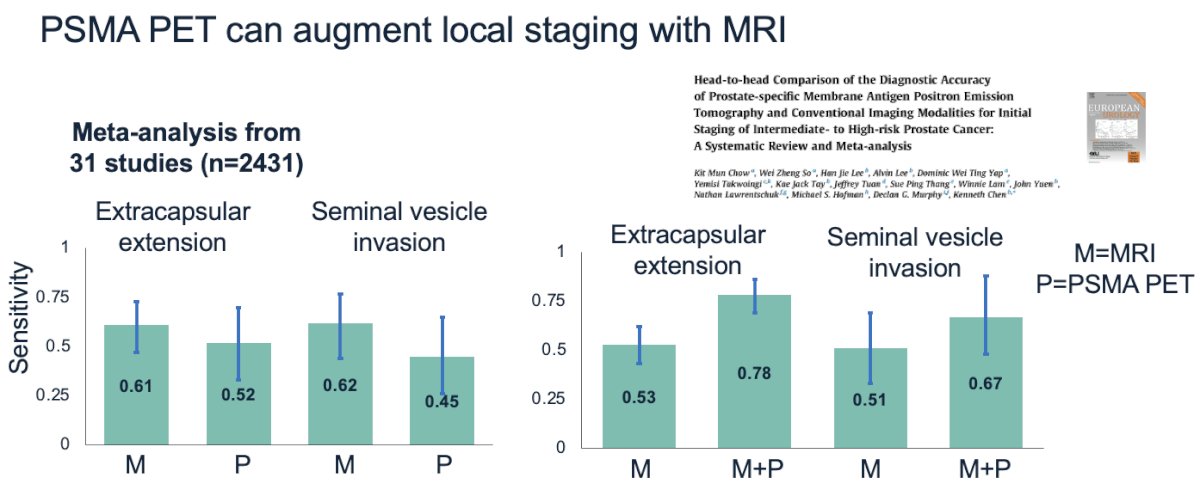
PSMA-PET may also have value for improving local staging accuracy when combined with MRI. A meta-analysis of 31 studies demonstrated that this combination approach, combined with MRI alone, improves the sensitivity for detecting extracapsular extension (78% versus 53%), seminal vesicle invasion (67% versus 51%), and pelvic nodal metastasis (74% versus 39%).7
What about PSMA-PET for surgical planning? A retrospective, multicenter cohort study of 3,978 men with N0/M0 disease who underwent a radical prostatectomy +/- pelvic nodal dissection was staged with PSMA PET (n=278) or conventional imaging (n=3,518). On multivariable logistic regression analysis, patients staged with PSMA-PET, compared to conventional imaging, had decreased odds of biochemical recurrence (OR: 0.61, p=0.004). This likely reflects a stage migration phenomenon owing to the improved sensitivity of PSMA-PET for staging of locally advanced/metastatic disease (i.e., some N0/M0 patients on conventional imaging likely would have been upstaged to N+/M+ on PSMA-PET).
Currently, a single center (Indiana University) phase 2/3 randomized controlled trial is evaluating the use of PSMA-PET to guide prostatectomy in prostate cancer patients (MRI +/- PSMA PET), with a primary outcome of erectile function and secondary outcomes of change in treatment, surgical pathology, and incontinence.
What about PSMA as a biomarker? Localized prostate cancer remains both biologically and clinically heterogeneous, with management approaches ranging from surveillance to multimodal therapies. Efforts to better characterize prostate cancer have resulted in improved imaging with PSMA PET. However, not all prostate cancer is seen on PSMA PET. As demonstrated below, this is a case of a 76-year-old male with a PSA of 10.2. Pre-biopsy MRI showed a PI-RADS 5 lesion in the left base with invasion into the left seminal vesicle, as well as an enlarged left iliac node.
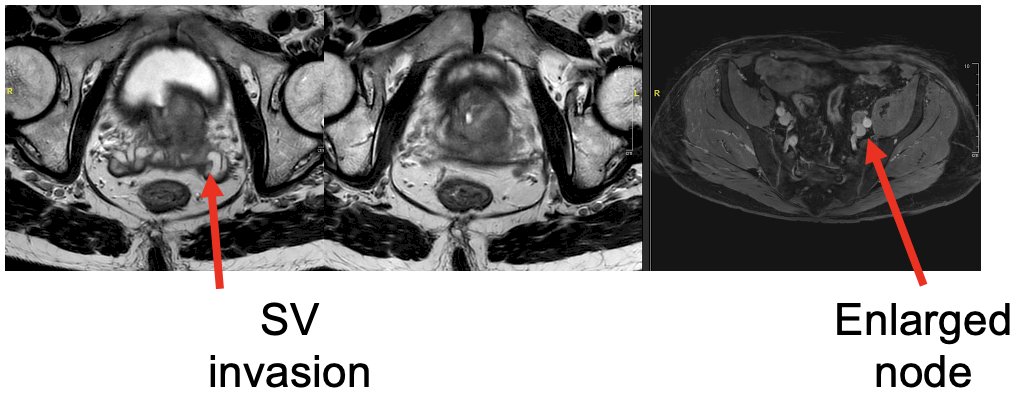
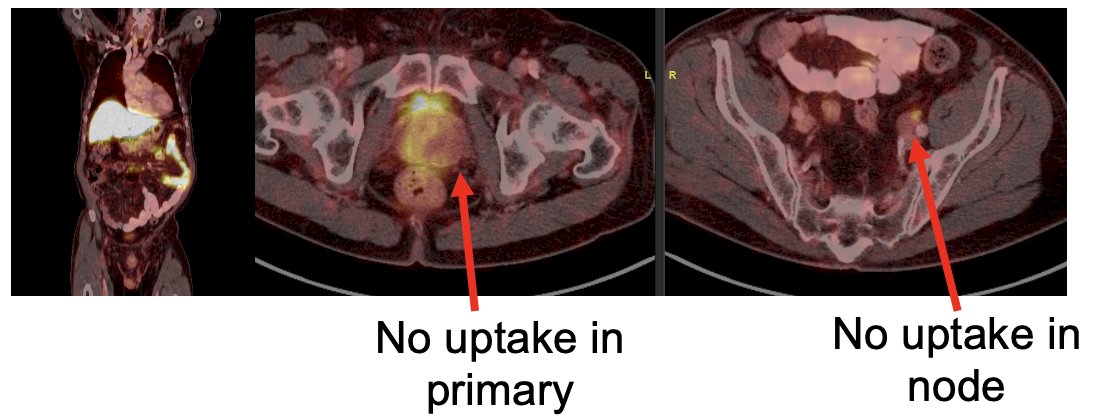
Biopsy confirmed Grade Group 5 prostate cancer only in the left base. However, PSMA-PET showed no PET avidity in the left base or the left iliac node.
As such, we clearly need a better understanding of the biology underlying differential PSMA expression that can help individualize cancer care, particularly with regards to treatment susceptibilities/prognostics and the need for further molecular testing. PSMA PET could be leveraged as one of the most commonly obtained biomarkers for early-stage prostate cancer.
Presented by: Adam Weiner, MD, Society of Urologic Oncology (SUO) fellow, Department of Urology, University of California, Los Angeles, CA
Written by: Rashid Sayyid, MD, MSc – Society of Urologic Oncology (SUO) Clinical Fellow at The University of Toronto, @rksayyid on Twitter during the 2024 American Urological Association (AUA) Annual Meeting, San Antonio, TX, Fri, May 3 – Mon, May 6, 2024.
References:
- Kasivisvanathan V, Rannikko AS, Borghi M, et al. MRI-Targeted or Standard Biopsy for Prostate-Cancer Diagnosis. N Engl J Med. 2018;378(19): 1767-77.
- Bass EJ, Pantovic A, Connor MJ, et al. Diagnostic accuracy of magnetic resonance imaging targeted biopsy techniques compared to transrectal ultrasound guided biopsy of the prostate: a systematic review and meta-analysis. Prostate Cancer Prostatic Dis. 2022;25(2): 174-9.
- Emmett L, Buteau J, Papa N, et al. The Additive Diagnostic Value of Prostate-specific Membrane Antigen Positron Emission Tomography Computed Tomography to Multiparametric Magnetic Resonance Imaging Triage in the Diagnosis of Prostate Cancer (PRIMARY): A Prospective Multicentre Study. Eur Urol. 2021;80(6):682-9.
- Kawada T, Yanagisawa T, Rajwa P, et al. Diagnostic Performance of Prostate-specific Membrane Antigen Positron Emission Tomography-targeted biopsy for Detection of Clinically Significant Prostate Cancer: A Systematic Review and Meta-analysis. Eur Urol Oncol. 2022;5(4): 390-400.
- Simopoulos DN, Natarajan S, Jones TA, et al. Targeted Prostate Biopsy Using 68Gallium PSMA-PET/CT for Image Guidance. Urol Case Rep. 2017;14: 11-4.
- Hofman MS, Lawrentschuk N, Francis RJ, et al. Prostate-specific membrane antigen PET-CT in patients with high-risk prostate cancer before curative-intent surgery or radiotherapy (proPSMA): a prospective, randomised, multicentre study. Lancet. 2020;395(10231):1208-1216.
- Chow KM, So WZ, Lee HJ, et al. Head-to-head Comparison of the Diagnostic Accuracy of Prostate-specific Membrane Antigen Positron Emission Tomography and Conventional Imaging Modalities for Initial Staging of Intermediate- to High-risk Prostate Cancer: A Systematic Review and Meta-analysis. Eur Urol. 2023;84(1): 36-48.