(UroToday.com) The 2023 American Urological Association (AUA) annual meeting held in Chicago, IL between April 28 and May 1st, 2023, was host to a plenary session that included a panel discussion for the management of upper tract urothelial carcinoma (UTUC). This discussion was moderated by Dr. Surena Matin, and included Drs. Jay Raman, Tomonori Habuchi, and Sima Porten as panelists.
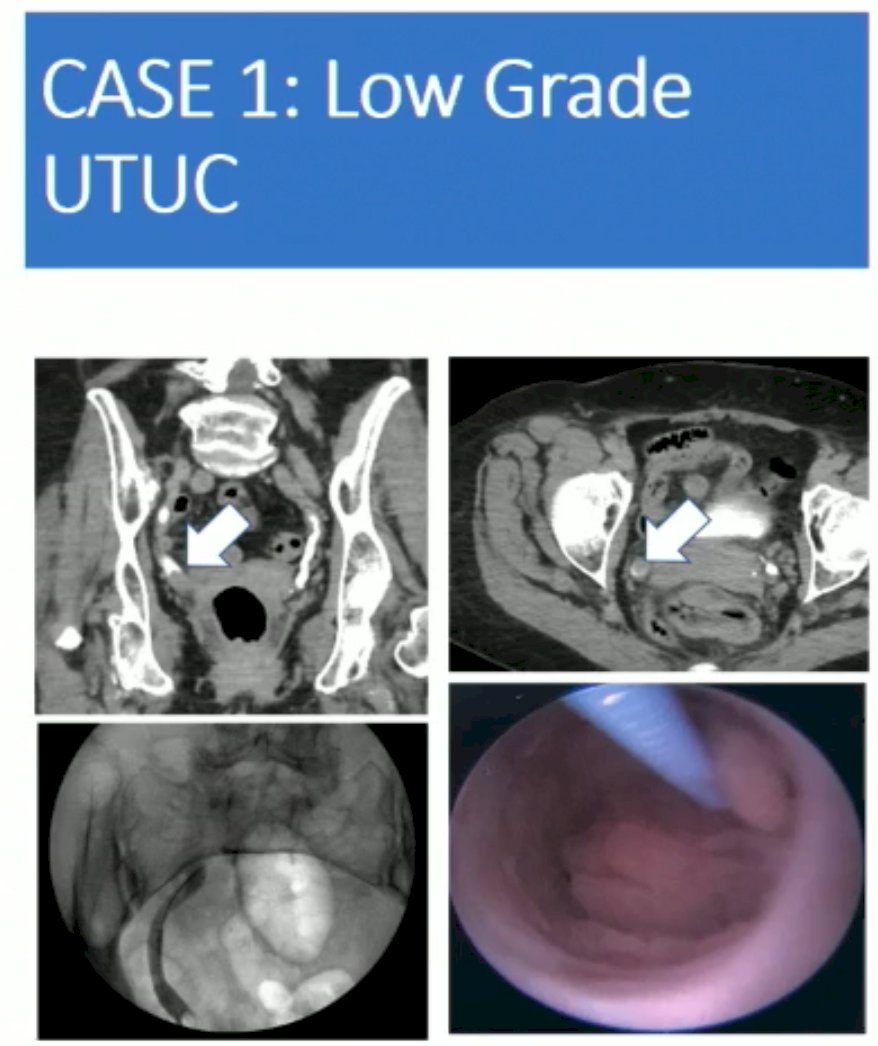
Dr. Matin began with a case presentation of an 85-year-old female with painless gross hematuria for 6 months. This patient was found to have a 3 cm right distal ureteral tumor with hydronephrosis. This patient underwent a biopsy with total laser ablation, with no other tumors seen. Biopsy demonstrated a low-grade, non-invasive tumor. At this point, the patient opted for surveillance.
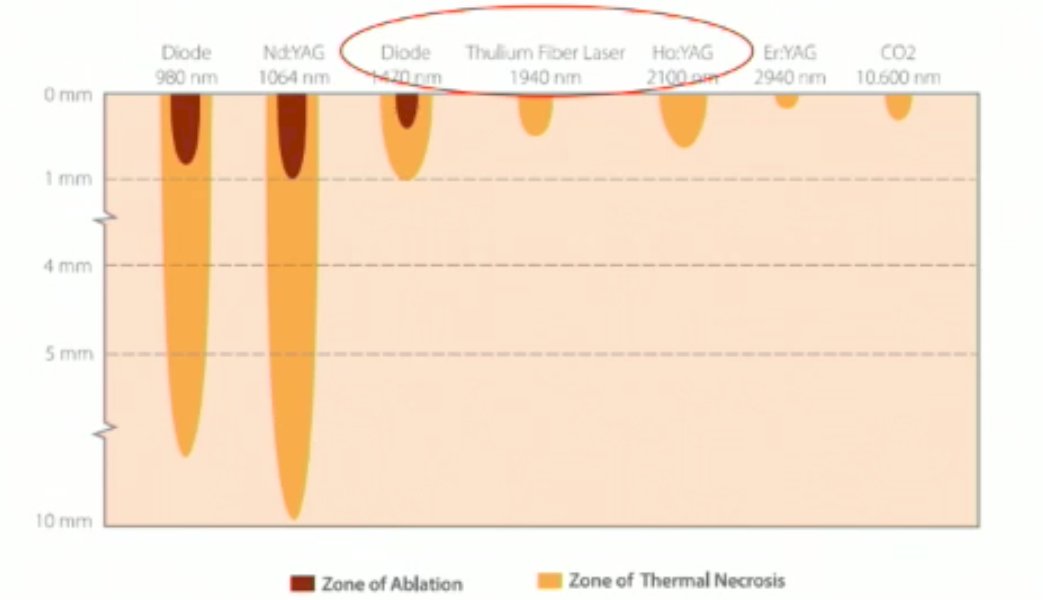
Dr. Matin queried the panelists regarding what laser energy sources they use for endoscopic ablation of UTUC. All four panelists indicated that they use Holmium: YAG laser in the majority of their cases. Commonly cited reasons included practical ones of laser type availability at their center, with holmium: YAG laser commonly used for stone procedures as well. Dr. Matin acknowledged the increased utilization of Thulium laser fibers in practice, however, as demonstrated below, the limited tissue penetration of the Thullium fiber laser remains an issue to consider.
Returning to the case presentation, 3 months later a cystoscopy and right ureteroscopy showed a 1 cm bladder tumor, which was resected, and multiple 5-8 mm tumors in the renal pelvis and lower calyces, some villous in appearance. All were biopsied (LG Ta) and were lasered. The patient received a single dose of intravesical gemcitabine post-operatively and was presented with the following options:
1. Repeat ureteroscopy in 3 months
2. Place a stent and give 6 weeks induction with intravesical chemotherapy
3. Instill mitomycin hydrogel (UGN-101) for 6 weeks retrograde or antegrade
The panelists and the voting crowd indicated that options 1 and 3 would be the most highly favored in this setting.

At this point, Dr. Matin addressed the question of routine intravesical chemotherapy use after ureteroscopy for UTUC. A 2021 study from the Mayo Clinic of 834 patients with UTUC demonstrated that 28.3% had intravesical recurrence. Significantly, ureteroscopy plus a biopsy was associated with an increased risk of intravesical recurrence compared to no ureteroscopy, percutaneous biopsy, or ureteroscopy alone (HR 1.40, p=0.04). Further analysis from the 2021 ROBUUST collaboration study of 485 patients demonstrated that 23% had intravesical recurrence at an average of 15.2 months. This study also demonstrated that ureteroscopic biopsy was a risk factor for intravesical recurrence.
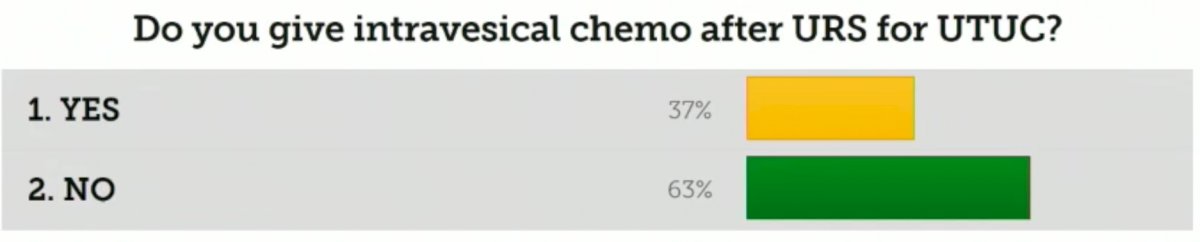
When queried, almost two-thirds of the attendees indicated that they do not give routine intravesical chemotherapy in this setting.
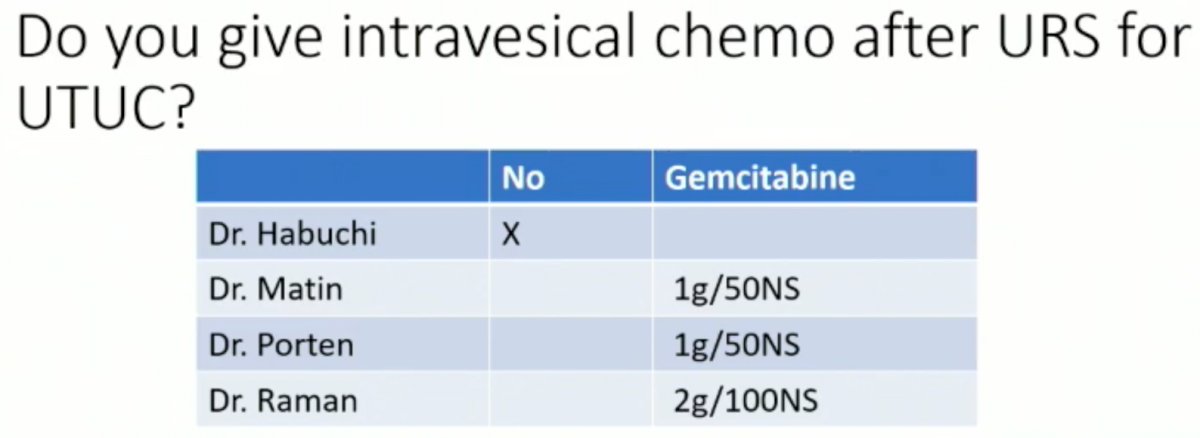
Although ureteroscopic manipulation is associated with higher risk of bladder recurrence, use of an access sheath and intravesical chemotherapy may reduce this risk. As such, 3/4 of panelists indicated that they were routinely given intravesical chemotherapy in this setting.
Next, Dr. Matin addressed the topic of mitomycin hydrogel (JELMYTO). Dr. Habuchi indicated that he does not use it as it is not yet approved in Japan. Dr. Porten also indicated that she does not currently use it in her practice for numerous reasons, which include no fluoroscopy in her clinics to allow for retrograde instillation, having to use the operating room regularly to gain access to fluoroscopy, and inability to give chemotherapy outside of infusion centers. To circumvent these issues, antegrade administration of JELMYTO via a nephrostomy tube has been advocated. This allows for safe, easier administration with no fluoroscopy needed, and may lead to fewer strictures due to the decreased instrumentation requirements. Dr. Matin then addressed the question of whether this drug should be used for chemoablation or in the adjuvant setting only. The data suggest that a better response is seen in the adjuvant setting, which may reflect a bias secondary to smaller residual tumor and thus a better response:
- Use in adjuvant setting (all tumor mechanically ablated first): 69% tumor-free at ureteroscopy
- Chemoablation (residual tumor as per clinical trial): 38% tumor-free at ureteroscopy
Dr. Matin noted that currently in his practice, he performs a maximal mechanical (laser) ablation at the time of ureteroscopy prior to JELMYTO instillation via a nephrostomy tube.
Going back to the case presentation, this patient had a negative ureteroscopy performed 8 weeks after induction JELMYTO. The patient experienced temporary ureteral narrowing that improved with a treatment holiday and steroids. One year later, the patient was found to have left (contralateral) multifocal low-grade UTUC, with the right side remaining without evidence of disease. The patient was treated with induction JELMYTO via a nephrostomy tube for 6 weekly treatments without difficulty. A bilateral ureteroscopy 6 weeks later was negative. The patient was given bilateral maintenance every two. Six months later the patient remained without evidence of recurrence bilaterally.

Dr. Matin next went on to present the second case of a patient with high grade UTUC with good baseline glomerular filtration rate (GFR). This was a 71-year-old female with a 2 cm left upper pole tumor that was incidentally found during surveillance for a remote history of lymphoma. The patient had no evidence of nodal involvement or pulmonary lesions. The lesion was biopsied and found to be T1 high grade. The patient had an eGFR of 62, Hgb of 11.5, and good split renal function with a performance status of 1.
Options for this patient include:
1. Nephroureterectomy +/- lymph node dissection, adjuvant chemotherapy based on pathology (POUT: gemcitabine + cisplatin or carboplatin)
2. Neoadjuvant chemotherapy followed by a nephroureterectomy +/- LND
3. Endoscopic management (unfavored)
While the majority of the audience (60%) indicated that they would proceed with surgery followed by adjuvant chemotherapy, Dr. Matin argued that a radical nephroureterectomy might be insufficient treatment for high-risk disease and comes at a cost of significant loss of kidney function that may preclude cisplatin chemotherapy. Indeed, a study by Lane et al. demonstrated that cisplatin eligibility decreases significantly in the post-radical nephroureterectomy setting:

Numerous nomograms have emerged to predict new baseline GFR post-surgery, based on pre-operative factors as demonstrated below:
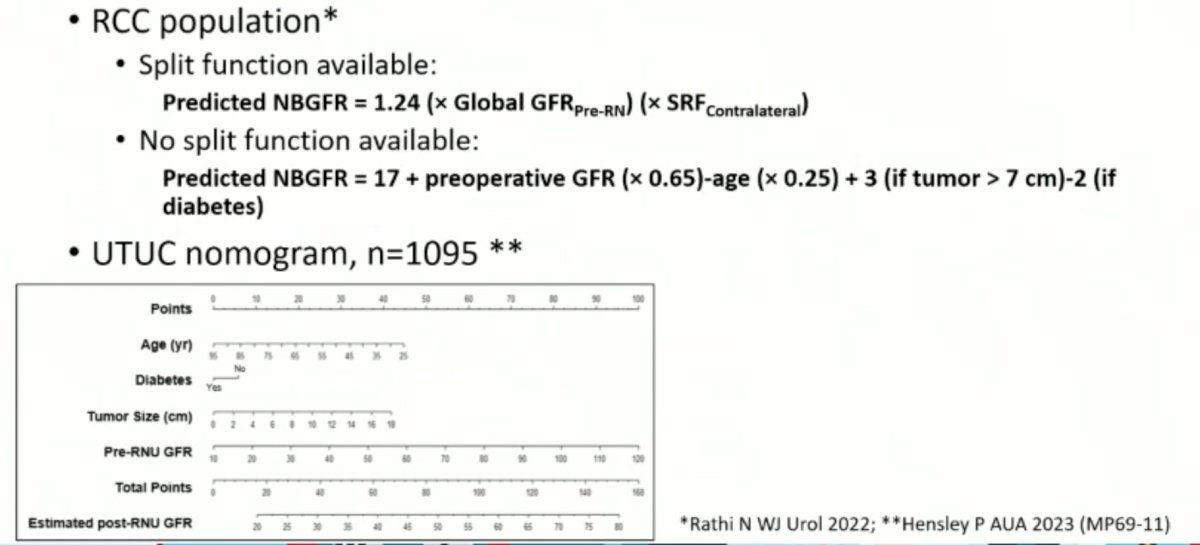
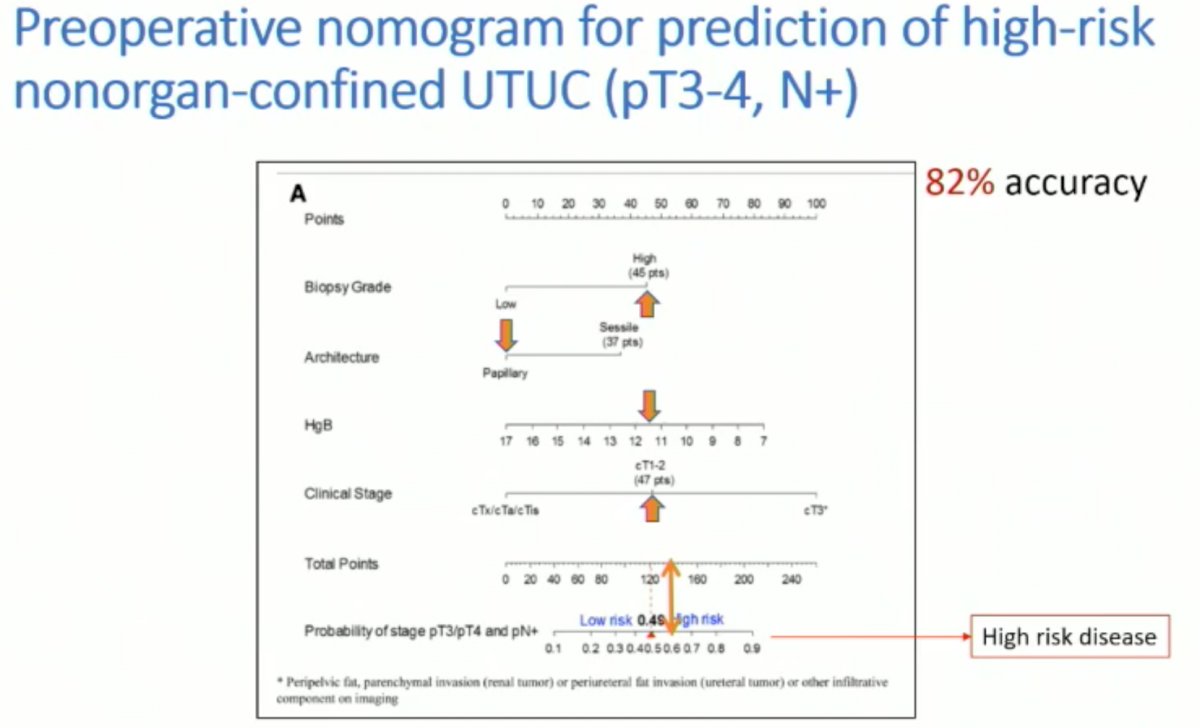
Based on the available data, the presented patient had an expected post-nephroureterectomy GFR of 42, which would significantly impair her ability to receive adjuvant chemotherapy. As such, the question becomes whether this patient needs neoadjuvant chemotherapy given the concerns for disease understaging. Current imaging modalities underestimate invasion (i.e., can rule-in, but not rule out). As such, risk stratification tools can help parse out those patients at higher risk. As demonstrated below, pre-operative nomograms exist for the prediction of pathologic muscle invasive UTUC and pathologic nodal disease:

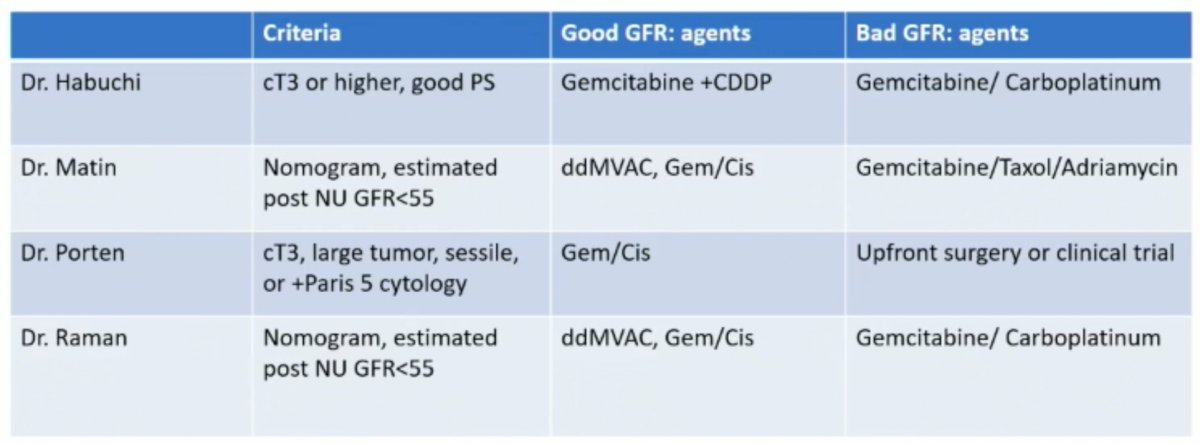
As such, it becomes clear that the decision for neoadjuvant chemotherapy for such patients is complicated. In the absence of clear level one evidence, the panelists’ criteria for recommending neoadjuvant chemotherapy are summarized below:
The phase II EA8141 trial of accelerated MVAC demonstrated pathologic complete response rates of 14%, with pT1 or less disease observed in 62% of patients.1 Similar results were observed in the recent phase II study published by Coleman et al . that demonstrated ypT0N0 rates of 19% with downstaging observed in 63% of patients.2

The patient went on to receive 4 cycles of neoadjuvant gemcitabine/cisplatin without difficulty with re-staging CT after 2 cycles showing a good partial response. At this point, the patient was planned for a radical nephroureterectomy. Similar to the post-ureteroscopic setting, Dr. Matin next queried the panel regarding the routine use of intravesical chemotherapy in the peri-nephroureterectomy setting. Three of the four panelists indicated that they routinely administer intravesical gemcitabine post-operatively, with the fourth, Dr. Habuchi highlighting his team’s ongoing clinical trial that is aiming to investigate the efficacy of this approach. This study will build on the available evidence in this setting, which includes two RCTs by O’Brien (UK) and Ito (Japan) that demonstrated an improvement in bladder recurrence-free survival as highlighted below:

With regards to surgical technique, excision of the bladder cuff is a critical component of this oncologic, extirpative procedure. The panelists indicated that they use an extravesical approach, although Dr. Matin argued that this is not strictly an extravesical approach, with a limited cystotomy often required as well to allow for adequate excision of the intramural ureter:

Other approaches to bladder cuff excision such as transurethral resection of the ureteral orifice and extravesical stapling have fallen out of favor due to retrospective data demonstrating that such approaches are associated with higher intravesical recurrence rates.

Finally, Dr. Matin discussed the role of lymphadenectomy for UTUC. The panel summarized their criteria for performing a lymphadenectomy as below:

Current dissection templates are based on laterality and the most likely landing zones for nodal tumor metastases:

Dr. Matin argued that we cannot rely on conventional imaging to rule out nodal metastases, and, as such, a lymph node dissection should be the reference standard for these patients. A recent multicenter, retrospective study of 815 patients demonstrated that the sensitivity and specificity of CT for cN-staging were 25% and 91%, respectively. The corresponding AUC was only 0.58, thus showing limited predictive ability to rule out the presence of pathologic nodal disease.
Dr. Matin concluded with the following take home messages:
- Consider mitomycin hydrogel for recurrent low-grade disease
- Intravesical chemotherapy with nephroureterectomy is supported by level 1 data
- Intravesical chemotherapy after ureteroscopic biopsy is supported by a preponderance of circumstantial data
- For high-risk disease patients:
- Use risk stratification
- Estimate post-nephroureterectomy kidney function to counsel between upfront nephroureterectomy versus neoadjuvant chemotherapy
- Do not shortchange distal ureter/bladder cuff dissection
- Consider lymphadenectomy for high-risk cases
Dr. Surena Matin, MD, Professor, Department of Urology, Division of Surgery, The University of Texas MD Anderson Cancer Center, Houston, TX
Panelists:- Jay D. Raman, MD, FACS, Professor and Chair, Department of Urology, Penn State Health Milton S. Hershey Medical Center, Hershey, PA
- Tomonori Habuchi, MD, Professor and Chairmen, Department of Urology, Akita University, Akita, Japan
- Sima P. Porten, MD, MPH, FACS, Associate Professor, Department of Urology, University of California in San Francisco, San Francisco, CA
References:
- Margulis V, et al. Phase II Trial of Neoadjuvant Systemic Chemotherapy Followed by Extirpative Surgery in Patients with High Grade Upper Tract Urothelial Carcinoma. J Urol, 2020.
- Coleman JA, et al. Multicenter phase II clinical trial of gemcitabine and cisplatin as neoadjuvant chemotherapy for patients with high-grade upper tract urothelial carcinoma. J Clin Oncol, 2023.
- Pallauf M, et al. Diagnostic Accuracy of Clinical Lymph Node Staging for Upper Tract Urothelial Cancer Patients: A Multicenter, Retrospective, Observational Study. J Urol, 2023.