(UroToday.com) The 2023 American Urological Association (AUA) annual meeting held in Chicago, IL between April 28 and May 1st, 2023, was host to the International Prostate Forum, with Dr. E. David Crawford discussing the history of the Prostate Cancer Radiographic Assessments for Detection of Advanced Recurrence (RADAR) group.
The initial report from RADAR (i.e., RADAR 1) was published in 2014.1 Based on the available evidence to that point, the RADAR group concluded that:
- There is inconsistency in the literature and current practice guidelines in terms of eligibility criteria, type of imaging modality, and the frequency of scanning for advanced prostate cancer patients
- As a result, there us underdiagnosis of metastatic disease and costs
- Consensus and recommendations to promote early identification of metastatic disease were developed by the RADAR 1 groups
- The objective was to improve patient management and facilitate appropriate treatment practices
- Early detection of metastases in prostate cancer is important for optimal patient management
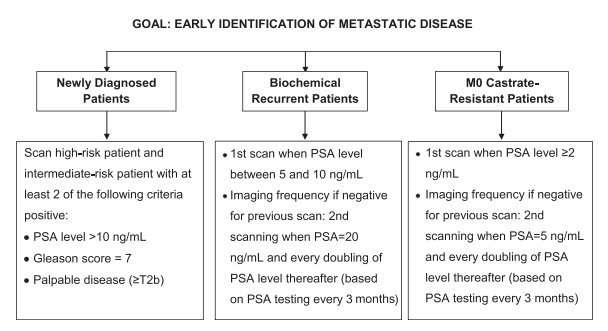
Based on the available evidence at that time, the RADAR group made the following recommendations for the following 3 disease states:
- Newly diagnosed patients
- Biochemical recurrent patients
- M0 castrate-resistant patients
The RADAR II recommendations were next published in 2017. The goal of RADAR II was to provide a consensus on sequencing, combination, and “therapeutic” layering. The group concluded at that time that: “In the absence of large-scale clinical trials, the Working Group recommends that patients may best be managed with a layered approach of approved therapies with unique or complimentary mechanisms of action.”

In 2019, the RADAR III recommendations were published. The goal of this update was to:
- Understand the potential use of next generation imaging in the initial staging of prostate cancer and in patients with biochemically recurrent, non-metastatic or metastatic prostate cancer, and castration-resistant prostate cancer
- Understand the rationale for obtaining these scans, the frequency of ordering them, and especially understanding the integration of the results obtained into clinical decision-making treatment algorithms
- Gauge the rapidity and ease of uptake of these novel imaging modalities among medical oncologists and urologic oncologists who practice in different settings around the country
- Redefine the existing terminology that does not accurately represent the changing landscape in biochemically recurrent, nonmetastatic or metastatic prostate cancer
- Update the existing RADAR I and II recommendations based on the availability of recent data
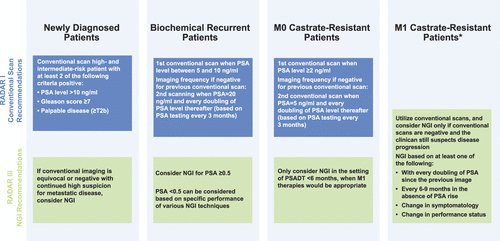
This was the first update to make imaging recommendations for patients with M1 CRPC (blue panels: RADAR I recommendations; green panels: RADAR III recommendations).
The RADAR IV and V updates focused on transitional disease states, including the castrate sensitive and resistant oligometastatic disease states as illustrated below:

The latest update of the RADAR group, RADAR VI, was recently published in The Journal of Urology Open Plus. This update focused on molecular targeted imaging (e.g., PSMA PET/CT). Summarized below are the RADAR VI recommendations for molecular targeted imaging in patients with newly diagnosed prostate cancer. Dr. Crawford highlighted that negative conventional imaging should not be considered a prerequisite for targeted precision imaging.
Targeted precision imaging is recommended for:
- Patients with unfavorable intermediate, high, or very high-risk prostate cancer
- Inconclusive prior conventional imaging in which there is a high clinical suspicion of metastatic or locoregional disease or risk of nodal metastases
- Patients who have an elevated molecular marker (Decipher®/Oncotype DX®/Prolaris®) scores
- Genomically diverse, high-risk patient populations

Conversely, targeted precision imaging may be considered in biochemical relapse in the following settings:
- For the patient for whom metastasis-directed therapy may be considered, targeted precision imaging is preferred over conventional imaging
- Early and accurate identification of sites of disease can lead to more anatomically directed therapy
- Optimizing outcomes can be facilitated by early detection of the site(s) of recurrent disease

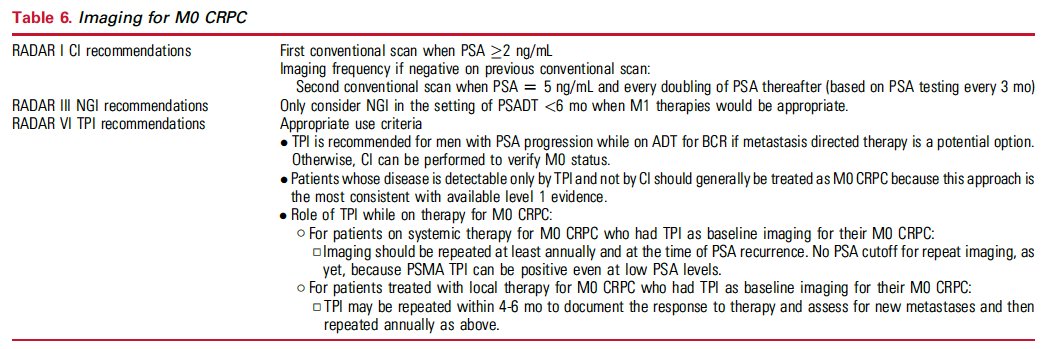
The RADAR VI recommendations for imaging of patients with M0 CRPC are as follows:
- TPI is recommended for men with PSA progression while on ADT for BCR if metastasis directed therapy is a potential option. Otherwise, CI can be performed to verify M0 status.
- Patients whose disease is detectable only by TPI and not by CI should generally be treated as M0 CRPC because this approach is the most consistent with available level 1 evidence.
- Role of TPI while on therapy for M0 CRPC:
- For patients on systemic therapy for M0 CRPC who had TPI as baseline imaging for their M0 CRPC:
- Imaging should be repeated at least annually and at the time of PSA recurrence. No PSA cutoff for repeat imaging, as yet, because PSMA TPI can be positive even at low PSA levels.
- For patients treated with local therapy for M0 CRPC who had TPI as baseline imaging for their M0 CRPC:
- TPI may be repeated within 4-6 months to document the response to therapy and assess for new metastases and then repeated annually as above.
- For patients on systemic therapy for M0 CRPC who had TPI as baseline imaging for their M0 CRPC:
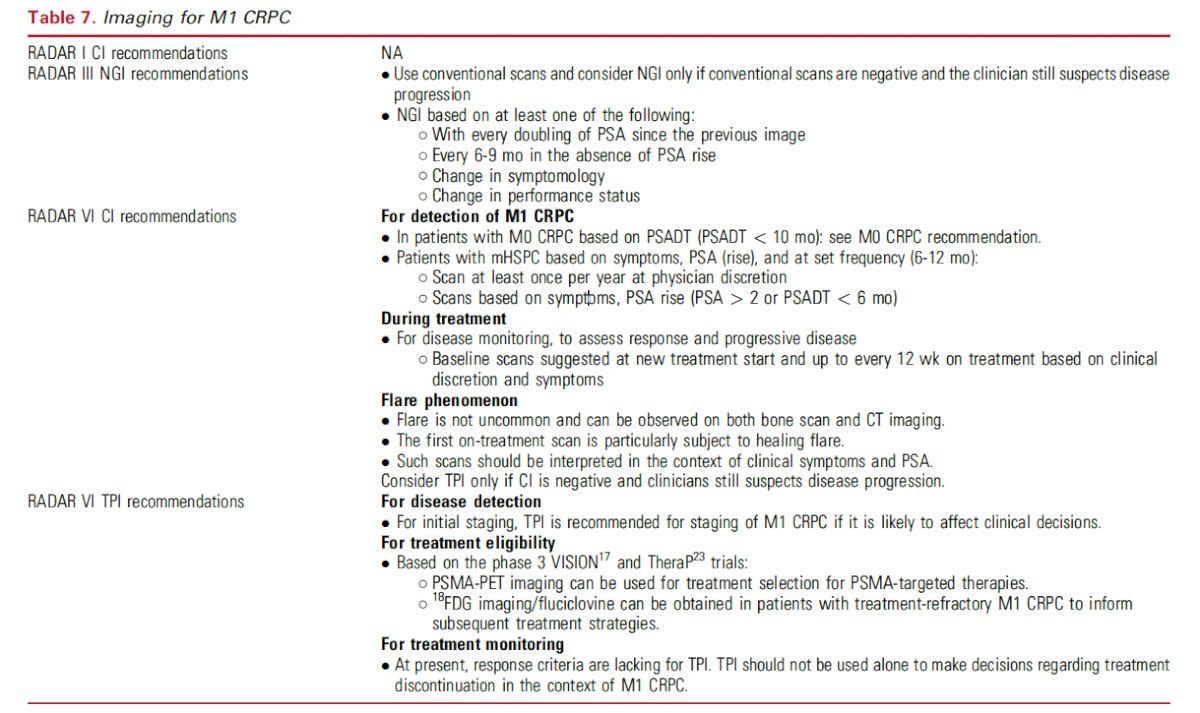
For patients with M1 CRPC, RADAR VI included the following recommendations:
For disease detection
- For initial staging, TPI is recommended for staging of M1 CRPC if it is likely to affect clinical decisions.
For treatment eligibility
- Based on the phase 3 VISION and TheraP trials:
- PSMA-PET imaging can be used for treatment selection for PSMA-targeted therapies.
- 18FDG imaging/fluciclovine can be obtained in patients with treatment-refractory M1 CRPC to inform subsequent treatment strategies.
For treatment monitoring
- At present, response criteria are lacking for TPI. TPI should not be used alone to make decisions regarding treatment discontinuation in the context of M1 CRPC.
What about conventional imaging-negative, molecular targeted imaging-positive (i.e., imaging-discordant) newly diagnosed metastatic prostate cancer:
- TPI is redefining advanced/metastatic prostate cancer.
- Men with positive TPI represent a wide spectrum of disease and heterogeneity.
- Clinicians have a number of therapeutic agents/interventions available in their armamentarium; most approvals are based on CI.
- Earlier therapeutic approaches tend to improve survival and outcomes.
- TPI offers an opportunity to implement MDT.


Written by: Rashid K. Sayyid, MD, MSc – Society of Urologic Oncology (SUO) Clinical Fellow at The University of Toronto, @rksayyid on Twitter during the 2023 American Urological Association (AUA) Annual Meeting, Chicago, IL, April 27 – May 1, 2023
References:
- Crawford ED, et al. Challenges and Recommendations for Early Identification of Metastatic Disease in Prostate Cancer. Urology, 2014.
- Crawford ED, et al. The Role of Therapeutic Layering in Optimizing Treatment for Patients With Castration-resistant Prostate Cancer (Prostate Cancer Radiographic Assessments for Detection of Advanced Recurrence II). Urology, 2017.
- Crawford ED, et al. A Clinician’s Guide to Next Generation Imaging in Patients With Advanced Prostate Cancer (RADAR III). J Urol, 2019.
- Crawford ED, et al. Evolving understanding and categorization of prostate cancer: preventing progression to metastatic castration-resistant prostate cancer: RADAR IV. Can J Urol, 2020.
- Crawford ED, et al. A Clinician’s Guide to Targeted Precision Imaging in Patients With Prostate Cancer (RADAR VI). J Urol Open Plus, 2023.
Improving Appropriate Utilization of Imaging in Prostate Cancer Patients: A Discussion on the RADAR Articles - E. David Crawford