(UroToday.com) The 2023 American Urological Association (AUA) annual meeting held in Chicago, IL between April 28 and May 1st, 2023, was host to the International Prostate Forum, with Dr. Fred Saad discussing the role of combination therapy for metastatic castrate-resistant prostate cancer (mCRPC).
mCRPC patients have poor survival outcomes, with an estimated median overall survival (OS) of approximately three years with currently approved 1st line agents within the context of a clinical trial.1 In the real-world setting, median OS for such patients is significantly worse, with a median OS of less than 2 years. This is due to the fact that most patients in the real-world receive only 1st line treatment regimens, whereas clinical trial mCRPC patients often receive 2 or 3 treatment regimens.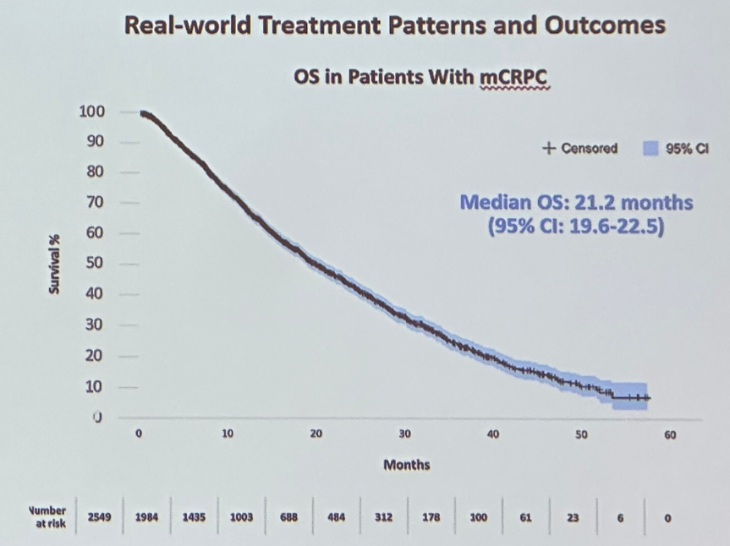
One of the major issues in the mCRPC disease space is that management remains monotherapeutic with a sequential treatment approach used in this setting. Furthermore, phase III trials in this disease space have only demonstrated OS benefits in trials with a non-life prolonging control arm as summarized below: 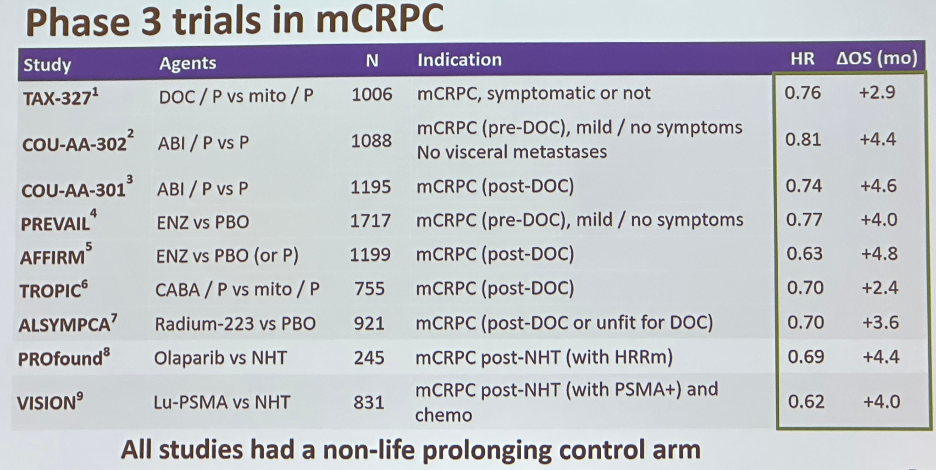
Numerous trials have evaluated docetaxel combinations for mCRPC patients and none, to date, have demonstrated any OS benefits.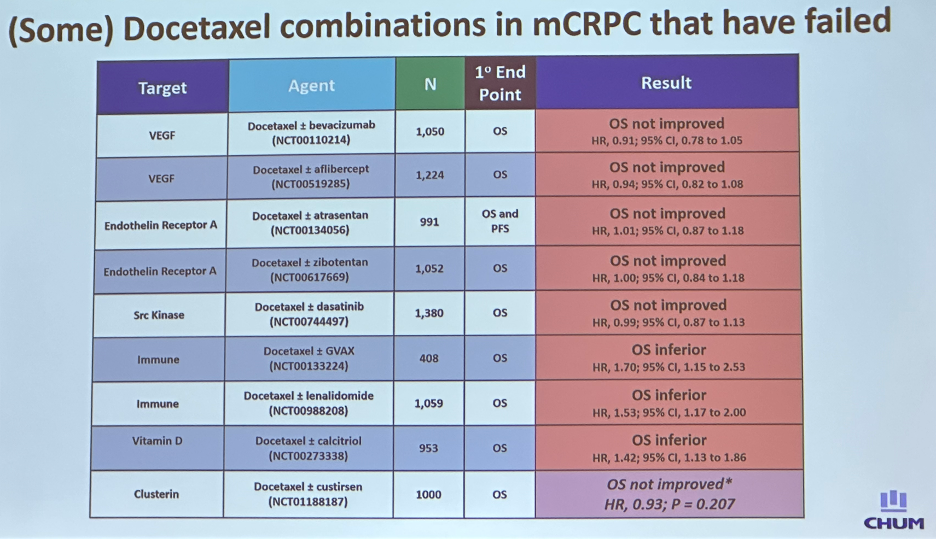
Furthermore, trials evaluating androgen receptor signaling inhibitor (ARSI) combinations in this setting have failed to demonstrate survival benefits for mCRPC patients. The ACIS trial evaluated the combination of apalutamide + abiraterone acetate/prednisone versus abiraterone/prednisone with rPFS, but no OS benefits.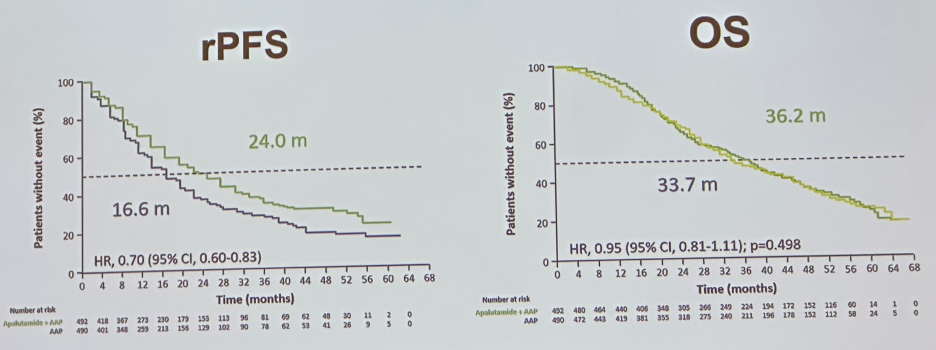
IPATential150 evaluated the combination of ipatasertib (an AKT inhibitor) plus abiraterone acetate/prednisone versus placebo + abiraterone acetate/prednisone. This trial included 1,101 previously untreated, asymptomatic, or minimally symptomatic mCRPC patients with progressive disease. The median follow up was 19 months. In the group of patients with PTEN loss (47% of total cohort), median rPFS was superior in the ipatasertib arm (18.5 versus 16.5 months; HR: 0.77, 95% CI: 0.61 – 0.98), with median PFS improvements also observed in the intent-to-treat population. However, such rPFS benefits were modest, and no OS improvements have yet to be demonstrated.2
Over the last few years, we have seen the emergence of PARP inhibitors in the mCRPC disease space. PROfound was a randomized, open-label, phase 3 trial that evaluated olaparib (PARPi) in men with mCRPC progression with a prior ARSI. All men had a qualifying alteration in prespecified genes with a direct or indirect role in homologous recombination repair. Cohort A (245 patients) had at least one alteration in BRCA1, BRCA2, or ATM; cohort B (142 patients) had alterations in any of 12 other prespecified genes, prospectively and centrally determined from tumor tissue. Patients were randomly assigned (in a 2:1 ratio) to receive olaparib or the physician’s choice of enzalutamide or abiraterone (control). The primary endpoint was imaging-based progression-free survival in cohort A according to blinded independent central review. As demonstrated in the Kaplan Meier plots below, olaparib monotherapy in this setting was associated with significant improvement in both rPFS and OS in these patients.3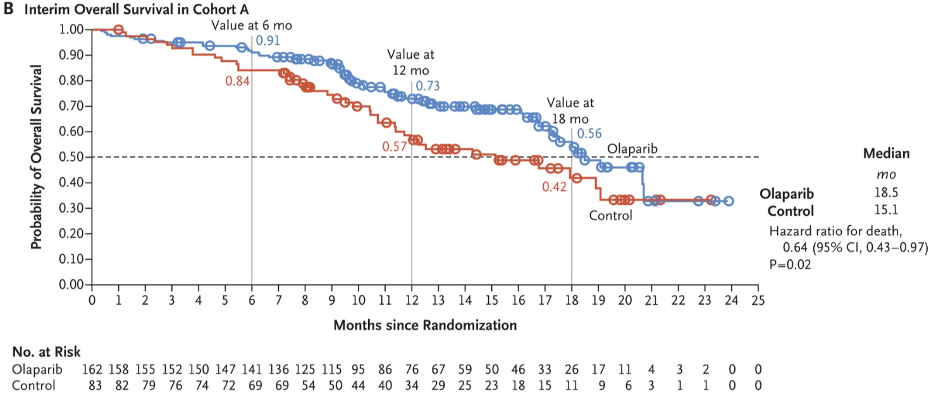
Preclinical studies suggest that PARPi and ARSIs may have synergistic mechanisms of action. PARPi upregulate androgen receptor signaling, enhancing ARSI activity. Conversely, ARSIs inhibit the transcription of some HRR genes, inducing an HRR deficiency-like state and potentiating PARPi activity. These findings suggest that this combination may demonstrate efficacy in patients irrespective of HRR mutational status. This hypothesis was supported by the results of a phase II trial that demonstrated that the combination of olaparib/abiraterone prolonged radiographic progression-free survival (rPFS) in docetaxel pre-treated, HRR biomarker unselected mCRPC patients.4
Over the past year, the results of three phase 3 clinical trials evaluating the combination of a PARPi + an ARSI have been reported: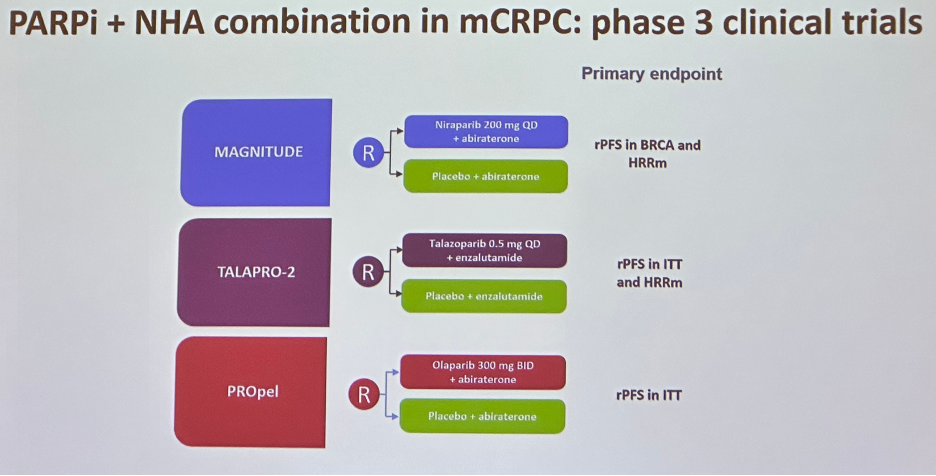
MAGNITUDE is a phase III, randomized, double-blinded study that evaluated the combination of niraparib and abiraterone acetate plus prednisone in patients with (n=423) or without (n=247) HRR-associated gene alterations. These patients were prospectively selected via tissue/plasma-based assays. Patients were assigned 1:1 to receive niraparib/abiraterone versus placebo/abiraterone. We note that a reduced dose of niraparib (200 mg) was used to due to drug-limiting toxicities with the full dose of 400 mg. The primary endpoint of radiographic progression-free survival (rPFS) was assessed by central review and was evaluated first in the BRCA1/2 subgroup, and then subsequently in the full HRR cohort. A futility analysis was pre-planned for the HRR- cohort.5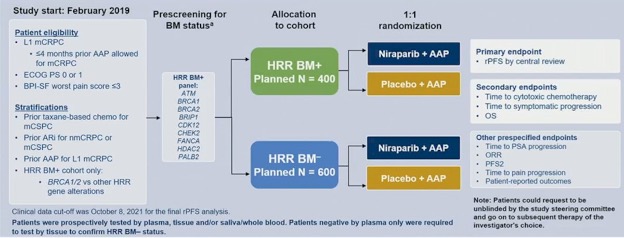
The preplanned futility analysis in 233 HRR biomarker negative patients showed no benefit of adding niraparib to abiraterone acetate/prednisone in the prespecified composite endpoint (first of PSA progression or rPFS, HR: 1.09, 95% CI: 0.75-1.59):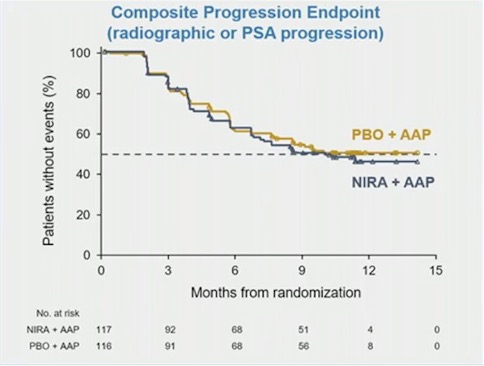
Conversely, in the HRRm and BRCA1/2 mutated cohorts, rPFS was significantly prolonged with the combination of niraparib + abiraterone acetate: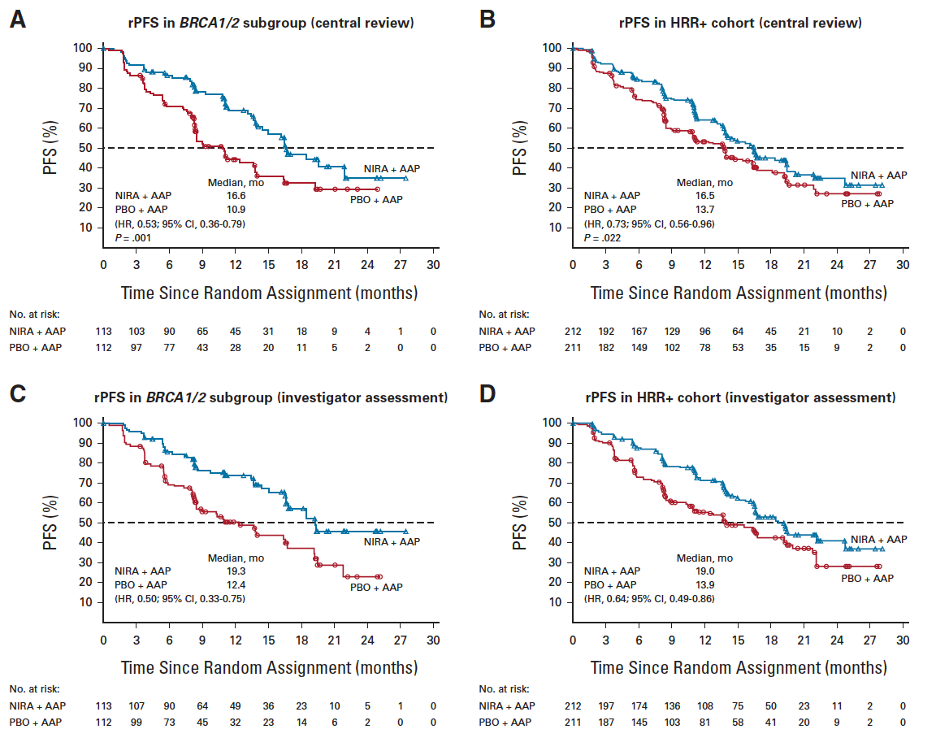
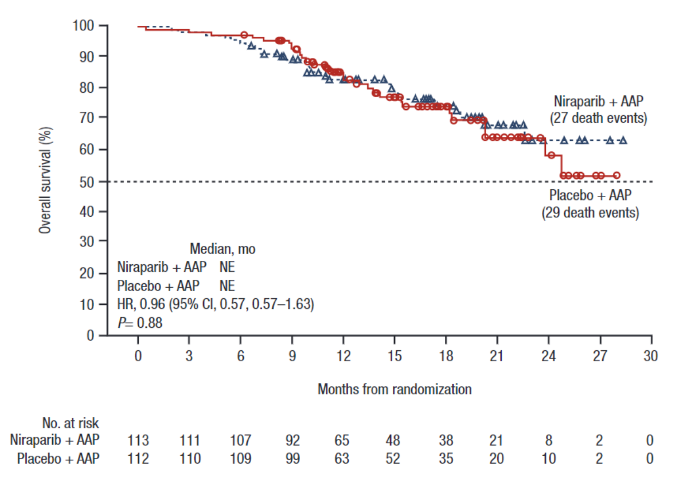
Overall survival data remains immature in this study (46.3%) with an OS HR of 0.94 (95% CI: 0.66 – 1.36, p=0.73) in the HRRm and 0.96 (95% CI: 0.57 – 1.63, p=0.88) in the BRCA1/2 mutated cohorts.
In the HRRm population, treatment-emergent AEs were consistent with the known safety profile for each therapy, with grade 3+ anemia occurring in almost 30% of patients.
TALAPRO-2, recently presented at ASCO GU 2023, is a phase 3 study evaluating the efficacy and safety of talazoparib + enzalutamide versus enzalutamide in patients with mCRPC in the 1st line setting.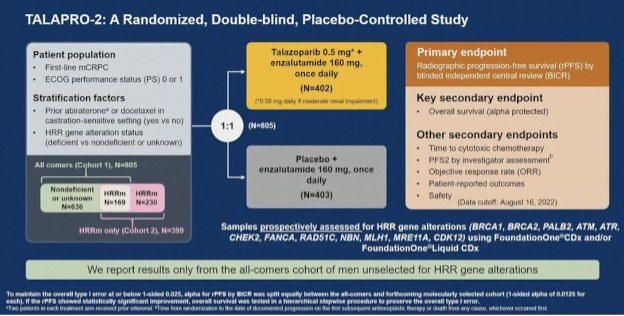
At a median follow up of nearly 25 months in both arms, the primary endpoint of rPFS, evaluated via blinded independent review, demonstrated a 37% decreased hazard of radiographic progression or death in the patients receiving talazoparib and enzalutamide, with a HR of 0.63 (95% CI: 0.51 - 0.78, p<0.001).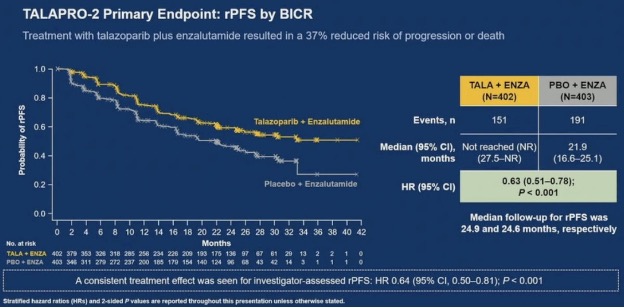
Significantly, rPFS was significantly prolonged with this combination in both the HRRm (HR: 0.56, 95% CI: 0.30 – 0.70) and non-HRRm/unknown cohorts (HR: 0.70, 95% CI: 0.54 – 0.89), albeit with a higher magnitude of effect in the HRRm cohort. 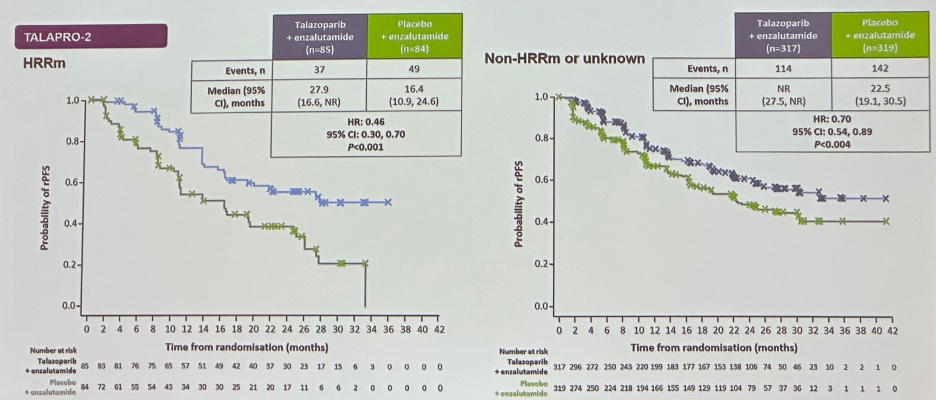
Similar to MAGNITUDE, OS data remains immature (31%) with a HR of 0.89 (95% CI: 0.69 – 1.14) in the intent-to-treat population.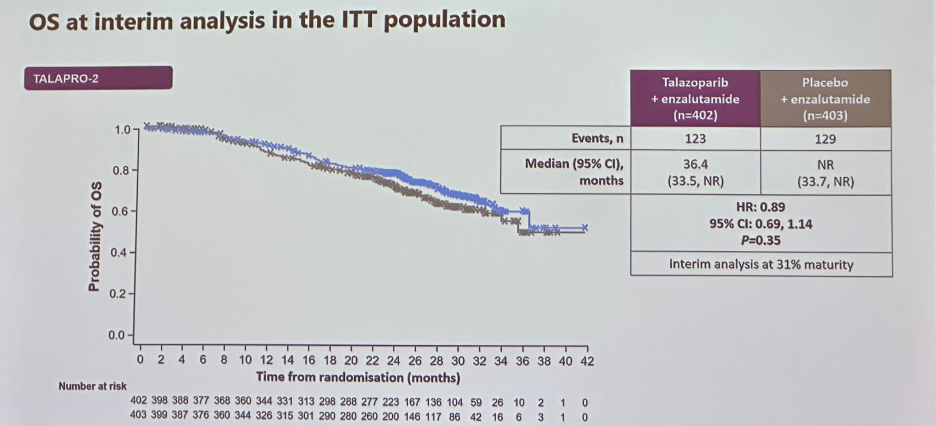
The AE profile was similar to MAGNITUDE, with grade 3+ anemia observed in 47% of patients in the combination arm.
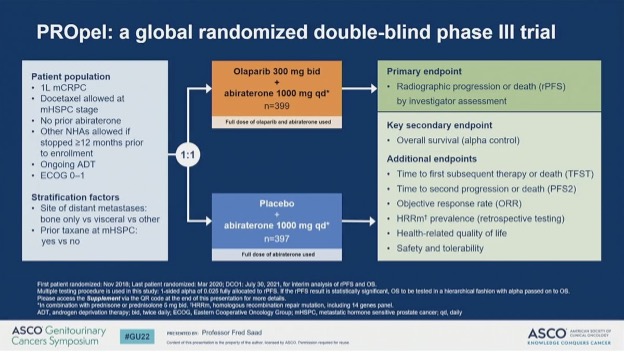
PROpel is a double-blind, phase 3 trial of abiraterone and olaparib versus abiraterone and placebo in mCRPC patients in the first-line setting. Patients were enrolled irrespective of HRRm status, which was determined following enrollment by tumor tissue and circulating tumor DNA tests. Patients were randomly assigned (1:1) to receive abiraterone (1000 mg once daily) plus prednisone or prednisolone with either olaparib (300 mg twice daily) or placebo. The primary endpoint was imaging-based progression-free survival by investigator assessment, with OS a key secondary endpoint.
As demonstrated in the figure below, approximately 30% of patients had known HRR mutations, whereas 70% were non-HRRm. PROpel met its primary endpoint with the addition of olaparib to abiraterone resulting in a 34% reduction in the rate of progression or death (HR: 0.66, 95% CI: 0.54 - 0.81; p<0.0001). The addition of olaparib improved median rPFS by 8.2 months (24.8 versus 16.6 months).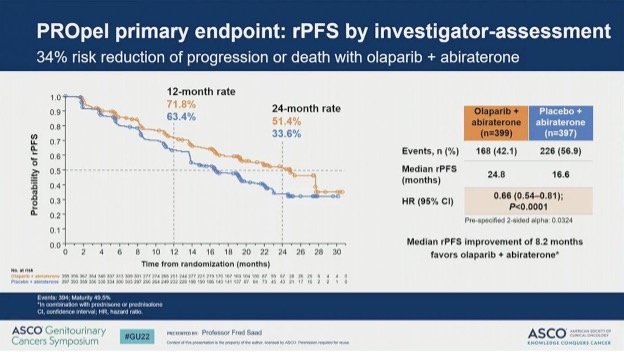
This finding was confirmed on blinded independent central review, on which olaparib resulted in a 39% improvement in rPFS rate and an 11.2-month improvement in median rPFS. 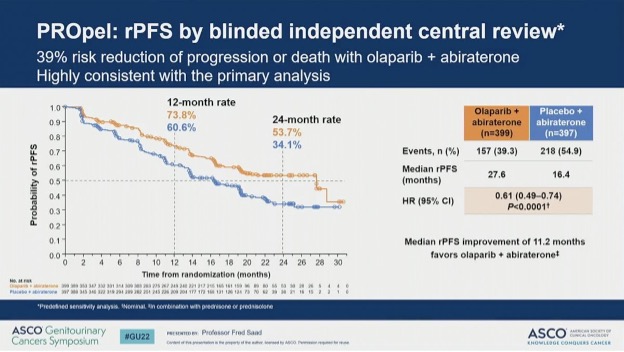
Subgroup analyses demonstrated an expected, pronounced rPFS benefit in the HRRm subgroup (HR: 0.50, 95% CI: 0.34 – 0.73):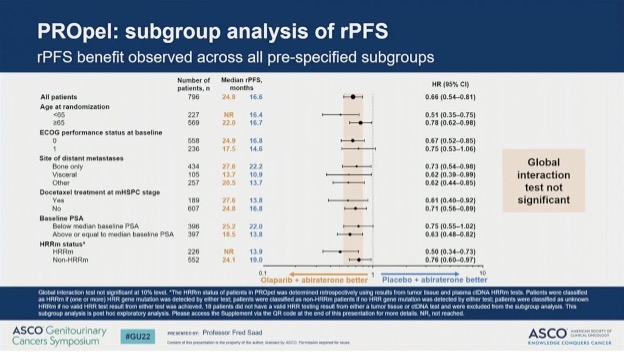
Evaluation of rPFS in the non-HRRm subgroup demonstrated consistent rPFS benefits, albeit with a lower magnitude of effect (HR: 0.76, 95% CI: 0.60 – 0.97). The final OS analysis of PROpel was recently presented at ASCO GU 2023, with data maturity of 47.9%. There appeared to be a trend towards an OS benefit in the combination arm with median OS improved from 34.7 to 42.1 months (HR: 0.81, 95% CI: 0.67 – 1.00 p=0.054). 
The AE profile was similar to the trials of the other two combinations; however, we note that the proportion of patients experiencing grade 3 or worse anemia was 16%, compared to 30% and 46% in MAGNITUDE and TALAPRO-2.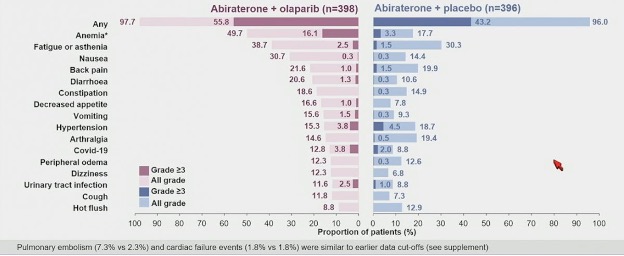
Dr. Saad concluded his presentation as follows:
- Three phase III trials have confirmed that PARPi + ARSs are effective in patients with HRR mutations
- Two phase III trials confirm that this combination works in patients without HRRm
- PROpel (most mature study of combination PARPi/ARSI to date) shows:
- 11-month rPFS advantage by BICR and a 7.4 months OS advantage in all-comers
- Encouraging results in the HRRm and BRCAm cohorts
- Now approved in Europe and several other countries
- Deciding who we treat that are non-HRRm or unknown will depend on risk factors for early progression on ARSIs alone and will be a shared decision with the patients.
Presented by: Fred Saad, MD, FRCS, Professor and Chief of Urology, Director of GU Oncology, University of Montreal Endowed Chair in Prostate Cancer, University of Montreal Hospital Center, Montreal, Quebec
Written by: Rashid K. Sayyid, MD, MSc – Society of Urologic Oncology (SUO) Clinical Fellow at The University of Toronto, @rksayyid on Twitter during the 2023 American Urological Association (AUA) Annual Meeting, Chicago, IL, April 27 – May 1, 2023
References:- Rathkopf DE, Smith MR, de Bono JS, et al. Updated interim efficacy analysis and long-term safety of abiraterone acetate in metastatic castration-resistant prostate cancer patients without prior chemotherapy (COU-AA-302). Eur Urol. 2014;66(5):815-825.
- Sweeney C, Bracarda S Sternberg CN, et al. Ipatasertib plus abiraterone and prednisolone in metastatic castration-resistant prostate cancer (IPATential150): a multicentre, randomised, double-blind, phase 3 trial. Lancet. 2021;398(10295):131-142.
- Hussain M, Mateo J, Fizazi K, et al. Survival with Olaparib in Metastatic Castration-Resistant Prostate Cancer. N Engl J Med. 2020 Dec 10;383(24):2345-2357.
- Clarke N, Wiechno P, Alekseev B, et al. Olaparib combined with abiraterone in patients with metastatic castration-resistant prostate cancer: a randomised, double-blind, placebo-controlled, phase 2 trial. Lancet Onco.l 2018; 19: 975-86.
- Chi KN, Rathkopf DE, Smith MR, et al. Phase 3 MAGNITUDE study: First results of niraparib (NIRA) with abiraterone acetate and prednisone (AAP) as first-line therapy in patients (pts) with metastatic castration-resistant prostate cancer (mCRPC) with and without homologous recombination repair (HRR) gene alterations. J Clin Oncol. 2023.
- Clarke N, Armstrong AJ, Thiery-Vuillemin A, et al. Abiraterone and olaparib for metastatic castration-resistant prostate cancer. NEJM Evidence. 2022.EVIDoa2200043.