(UroToday.com) The 2023 AUA annual meeting included an advanced prostate cancer session, featuring a presentation by Dr. Craig Jones discussing clinical fracture incidence in metastatic hormone sensitive prostate cancer (mHSPC) and risk reduction following the addition of zoledronic acid to ADT with or without docetaxel in the STAMPEDE platform. Long-term ADT is recommended for men with mHSPC, however, bone loss and increased fracture risk are known complications. The STAMPEDE trial compared ADT ± docetaxel ± zoledronic acid, whereby adding zoledronic acid did not improve overall survival1 but long-term effects of bisphosphonate treatment on skeletal health were not formally collected as part of the trial. Accessible, high quality, routinely-collected healthcare data enables analysis of outcome data beyond standard trial follow-up to evaluate long-term treatment toxicity and clinical efficacy of zoledronic acid as a bone protective agent in mHSPC. Additionally, the Hospital Episode Statistics database provides routinely-collected healthcare data for patients in England and Wales.
Hospital Episode Statistics data up to 2018 were obtained for patients randomized 2:1 between ADT (Arm A) and ADT+ zoledronic acid (Arm B), or ADT+ docetaxel (Arm C) or ADT+ docetaxel + zoledronic acid (Arm E). Zoledronic acid (4 mg) was six 3-weekly cycles, then 4-weekly for 2 years:
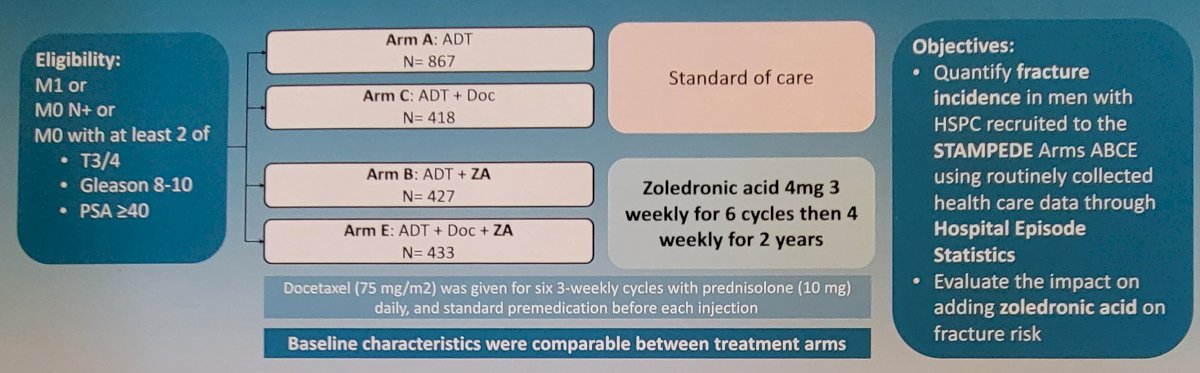
Clinical fracture events were identified using a bespoke pre-specified coding framework ICD 10 diagnosis and Classification of Interventions and Procedures (OPCS 4) procedure codes. Multivariate Cox regression models were developed to adjust for age, N stage, WHO performance status, Gleason score, and NSAID use to determine the impact of zoledronic acid on fracture risk.
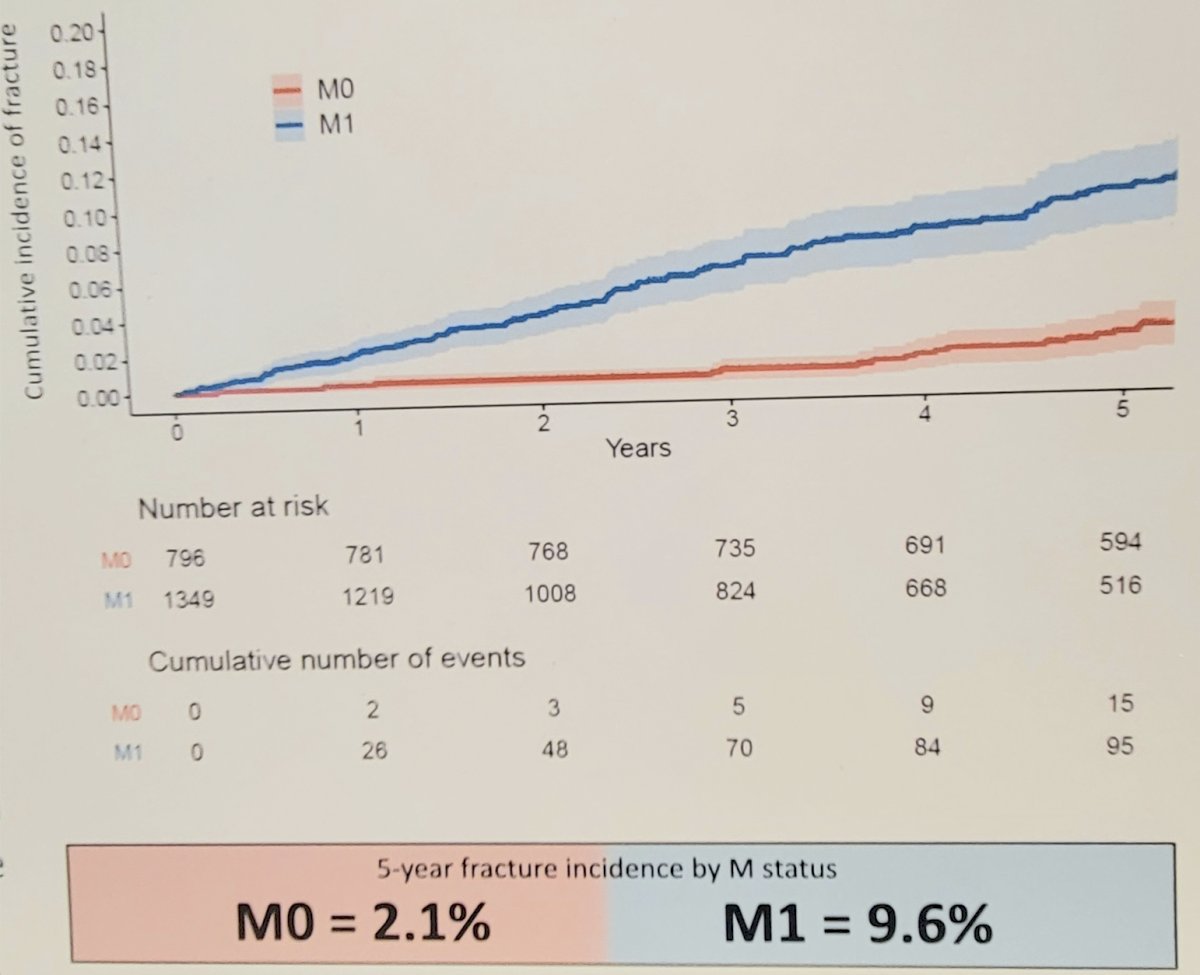
For this study, connected datasets were available for 2,145 eligible patients (796 M0, 1,349 M1) of 2,962 (72%). Overall, 5-year fracture incidence was 6.4% and higher in M1 patients (9.6% in M1 vs 2.1% in M0, p<0.0001):
and lower amongst M1 patients allocated zoledronic acid (4.5% with zoledronic acid vs 12.9% without zoledronic acid, p<0.0001). As follows is the cumulative fracture incidence within STAMPEDE arms A, B, C, and E (M1 only):
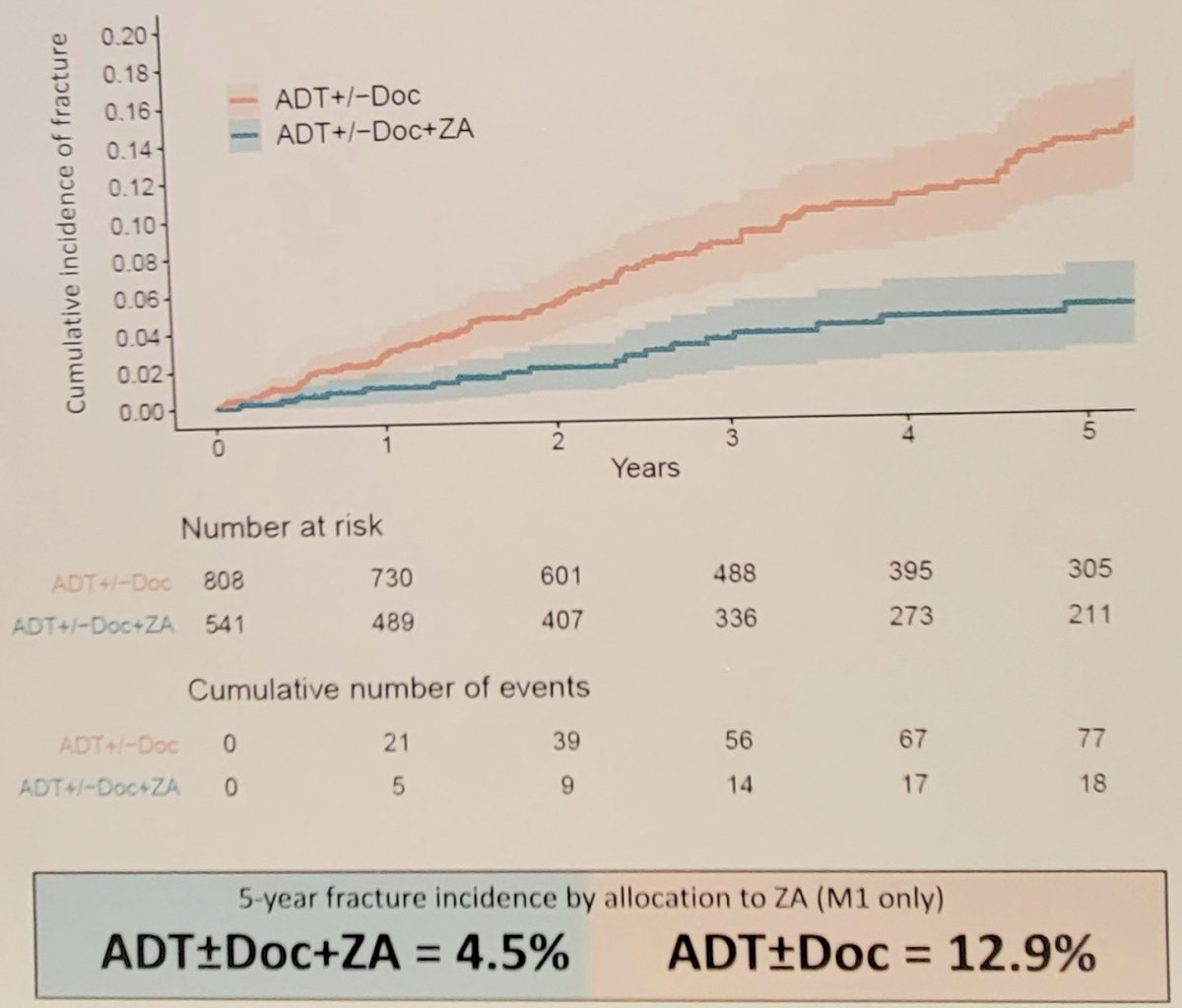
Zoledronic acid significantly reduced fracture risk in M1 patients (HR 0.36, 95% CI 0.22-0.57, p < 0.0005) but not in M0 patients (HR 0.67, 95% CI 0.32-1.39, p = 0.28).
Dr. Jones concluded his presentation by discussing clinical fracture incidence in mHSPC and risk reduction following the addition of zoledronic acid to ADT with or without docetaxel in the STAMPEDE platform with the following take-home messages:
- By accessing routinely-collected healthcare data, this study evaluated long-term fracture events amongst patients in STAMPEDE
- Fracture rates were clinically notable in M1 and reduced significantly in patients allocated zoledronic acid with ADT ± docetaxel
- These data support using bone protective agents to reduce clinically significant fractures in mHSPC
Presented by: Craig Jones, MD, Salford Royal and Christie Hospitals, Manchester, UK
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Assistant Professor of Urology, Georgia Cancer Center, Augusta University/Medical College of Georgia, @zklaassen_md on Twitter during the 2023 American Urological Association (AUA) Annual Meeting, Chicago, IL, April 27 – May 1, 2023
References:
- James ND, Sydes MR, Clarke NW, et al. Addition of docetaxel, zoledronic acid, or both to first-line long-term hormone therapy in prostate cancer (STAMPEDE): survival results from an adaptive, multiarm, multistage, platform randomised controlled trial. Lancet. 2016;387(10024):1163-1177.