(UroToday.com) Radical nephrectomy, surgical resection of renal cell carcinoma, has been widely accepted as the standard treatment for RCC. However, in patients with adverse pathology, the risk of recurrence is much greater. Often, adjuvant immunotherapies are utilized, postoperatively, to combat the risk that cancer may return. Through the S-TRAC trial, the anti-VEGF tyrosine kinase inhibitor agent, sunitinib, was approved for adjuvant purposes.1 However, lack of overall survival improvement and adverse effects restrict its practical application in clinical settings. Moreover, though the adjuvant capabilities of atezolizumab and nivolumab have been previously investigated with INmotion020 and KeyNote 564 trials, there seem to be contradictory findings as they did not show improvement.2,3
During the 2023 AUA Meeting, Dr. Harshit Garg, from the University of Texas delivered a fascinating presentation on the adjuvant role of ICI in high risk ccRCC. His team sought to explore real-world survival outcomes associated with adjuvant immunotherapy. They evaluated current patient trends from the National Center Database to contrast survival outcomes with adjuvant therapy versus targeted therapy.
Dr. Garg and his team performed a nationwide contemporary cohort study. Patients diagnosed with non-metastatic high-risk clear cell RCC undergoing a radical nephrectomy or metastatic disease undergoing cytoreductive nephrectomy and metastasectomy between 2015-2019 were included as a part of this study. Immunotherapy coding was characterized as having received ICI since 2015. High-risk was characterized as cT2 with Fuhrman grade 4 or cT3a with Fuhrman grade 3/4 or cT3b/T3c/T4 with any grade, or TxN+ any grade. Patients were divided into two groups. The first group, Group A, consisted of those who were receiving adjuvant ICI. In contrast, patients who did not receive adjuvant ICI (adjuvant targeted therapy) were put into Group B. Three thousand forty-seven patients met inclusion criteria with 933 in Group A and 2114 in Group B. In order to compare the overall survival (OS) between the groups, inverse probability weighting (IPW)-adjusted Kaplan Meier curves were applied. Furthermore, cox proportional hazard models were employed to recognize the predictors of overall survival.

Figure 1: This figure (above) depicts the process of patient selection for this study.
Table 1: This table displays the clinicodemographic profile of the study cohort.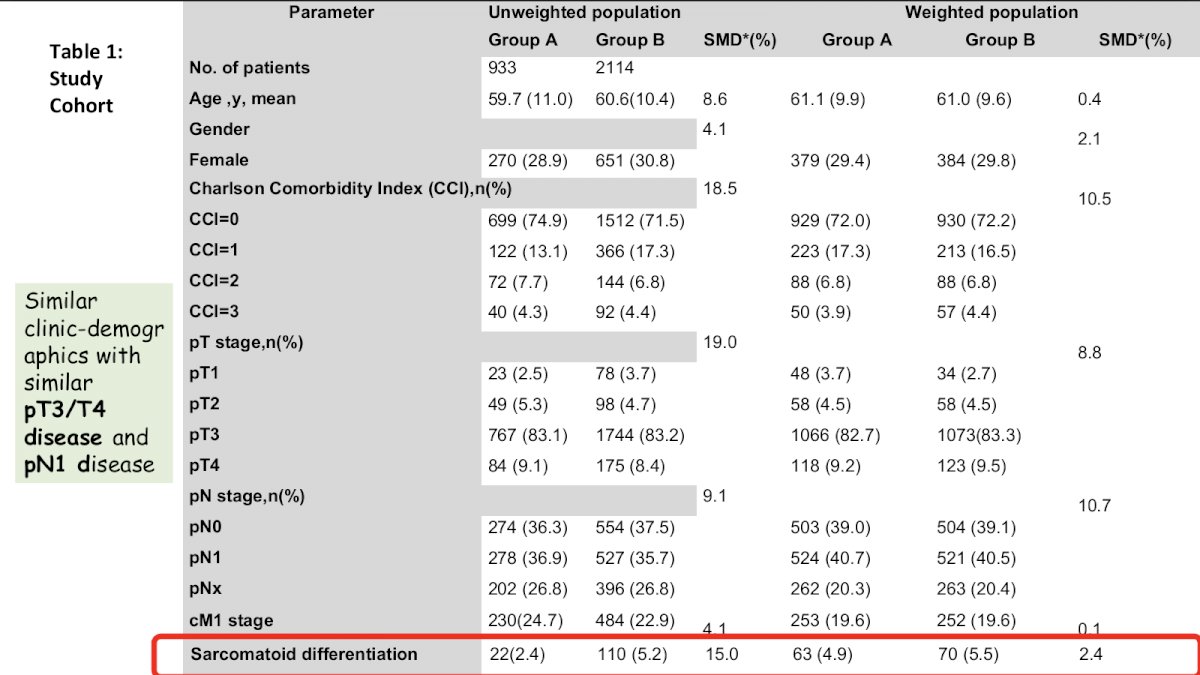
From their cohort study, Dr. Garg and his colleagues found that the use of adjuvant therapy has increased in recent years, with an increase from 1.3% in 2015 to 5.5% in 2018 and 4.8% in 2019. To add, the use of targeted therapy seemed to be very stable during the years 2015 to 2018 but declined in 2019. (Figure 2). He finds it very interesting to note that a large percentage of patients do not receive therapy following radical nephrectomy. The figure, below, depicts unadjusted and adjusted Kaplan-Meier estimates of overall survival in patients with high-risk kidney cancer undergoing a radical nephrectomy receiving adjuvant immunotherapy versus adjuvant targeted therapy. As seen in Figure 3 (below), Dr. Garg and his team found that, even following the IPW-adjusted cohort analysis, the three-year overall survival was similar between both groups. According to a multivariable cox-regression analysis, the application of adjuvant ICI does not seem to be an independent predictor for overall survival. This team concludes that despite a significant increase in the utilization of adjuvant ICI for ccRCC with a high risk of relapse, adjuvant ICI did not provide an advantage in terms of overall survival. To add, more research should be conducted to identify patients for benefit from adjuvant immunotherapy.

Figure 2: Utilization of Adjuvant Therapy in RCC

Figure 3: Unadjusted (2a) and adjusted (2b) Kaplan-Meier estimates of overall survival in patients with high-risk kidney cancer undergoing a radical nephrectomy with adjuvant immunotherapy versus adjuvant targeted therapy.
Following his presentation, the session attendees and speakers participated in a discussion. Dr. Garg emphasizes the importance of determining the role of adjuvant ICI as these therapies bestow a considerable financial burden on patients. With a substantial number of patients not receiving therapy postoperatively, it is pertinent to decipher which therapies are most effective for those with high risk for recurrence.
Presented by: Harshit Garg, MD, UT Health Science Center at San Antonio, @Garg_H on Twitter
Written by: Candices Tran, B.S., University of California, Irvine, @candicesmtran on Twitter during the 2023 American Urological Association (AUA) Annual Meeting, Chicago, IL, April 27 – May 1, 2023
References:
- Motzer, R. J, et al. Adjuvant Sunitinib for High-risk Renal Cell Carcinoma After Nephrectomy: Subgroup Analyses and Updated Overall Survival Results (2018)
- Pal, S. K, et al. Adjuvant atezolizumab versus placebo for patients with renal cell carcinoma at increased risk of recurrence following resection (IMmotion010): a multicentre, randomised, double-blind, phase 3 trial (2022)
- Choueiri, T. K, et al. KEYNOTE-564 Investigators Adjuvant Pembrolizumab after Nephrectomy in Renal-Cell Carcinoma (2021)