Dr. Shuch began by highlighting the growing incidence of RCC – specifically, a 2.5X increase in incidence compared to 3 decades ago, likely primarily driven by increased cross-sectional imaging and the obesity epidemic. BUT, rising incidence rates may not tell the whole story. As noted in multiple studies now, while the incidence has been rising, mortality and metastatic spread has remained relatively unchanged – suggesting that we are finding more indolent cancers that were unlikely to cause death or significant impact. This is similar to the story in thyroid cancers.
But, despite this, it is important to note that we have been likely overtreating some cT1 renal masses – and undertreating others. Not all cT1 renal masses should be treated equally. “To a man with a hammer, everything looks like a nail.”
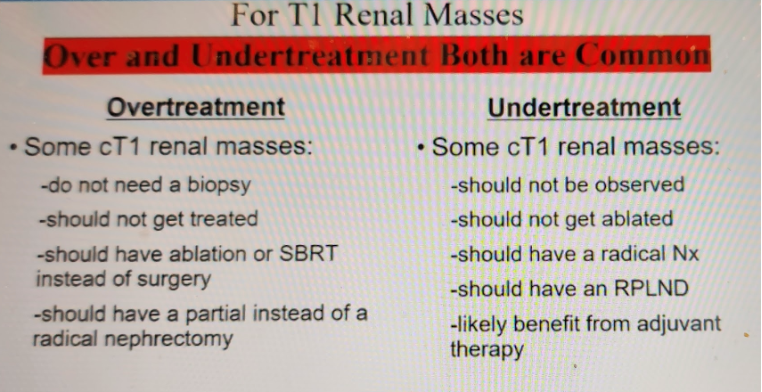
As Urologists, and specifically those with an expertise in kidney cancer, we should employ the tools we have in the right way. We have to thread the “therapeutic needle” to determine the optimal treatment strategy – and offering one treatment modality for all is NOT providing appropriate care.
As he then pointed out in the NCCN guidelines (which he is a part of), treatment guidelines are dictated by clinical staging – which ultimately for cT1-2 lesions is SIZE dependent.
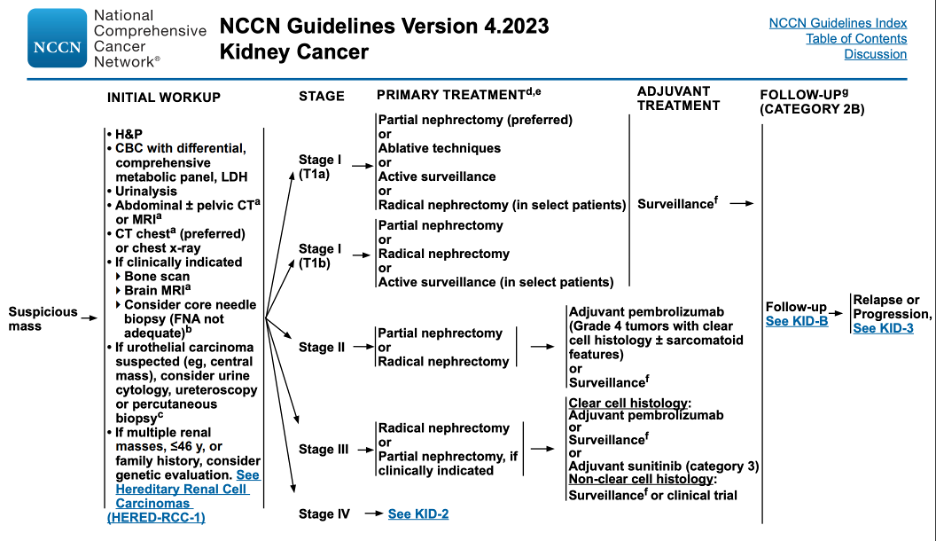
But, this ignores the biology of the tumor. Size doesn’t tell the whole story. And ultimately, Biology is KING.
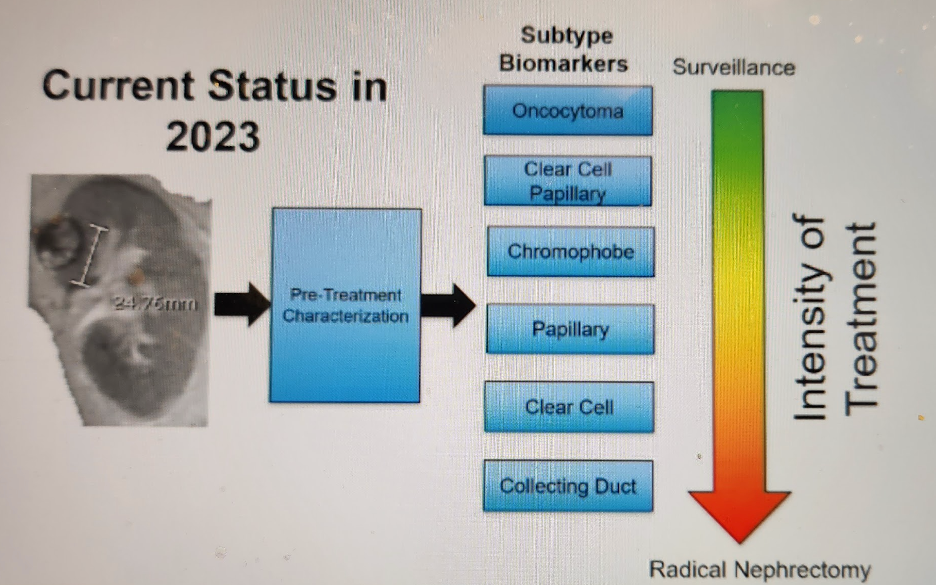
Our goal for treatment should be to match biology with treatment intensification. The current status is 2023 looks something like this:
Our understanding of RCC has drastically evolved – with the latest WHO classification breaking it down into morphologically defined subtypes and molecularly defined subtypes.
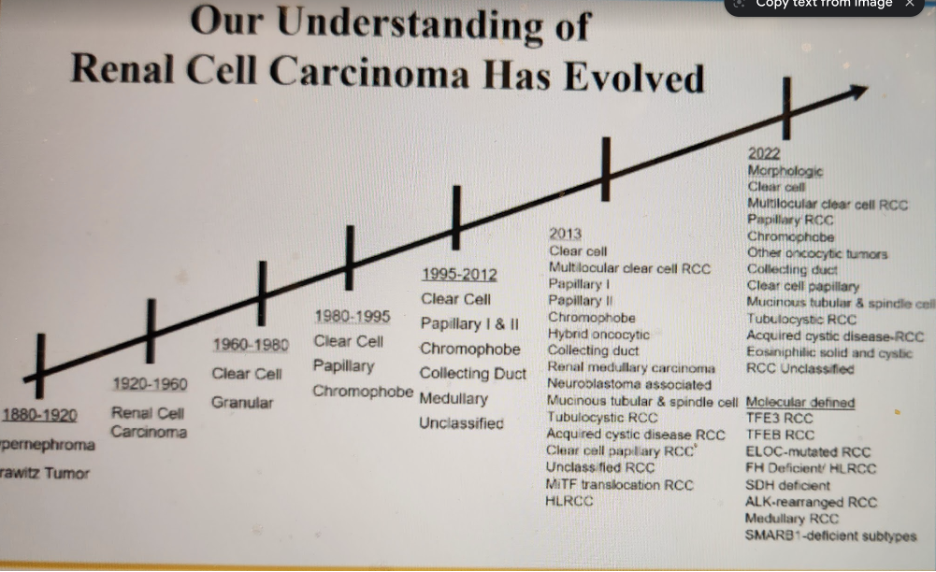
But, this also includes a greater number of benign renal tumors beyond just oncocytomas and AML – includes papillary adenomas (<1.5 cm now), renomedullary interstitial cell tumors, metanephric adenomas, Leiomyomas, mixed epithelial and stromal tumors (MESTs).
Newer emerging renal tumor entitities include:
- Biphasic hyalizing psammomatous tumors (BHP) RCC (NF2 mutated)
- Biphasic squamoid alveolar
- Papillary renal neoplasm with reverse polarity
- Warthin-like papillary RCC
- Thyroid-like follicular RCC
- Eosinophilic vacuolated tumor
He breaks these down into buckets of aggressiveness – which can in turn dictate treatment.
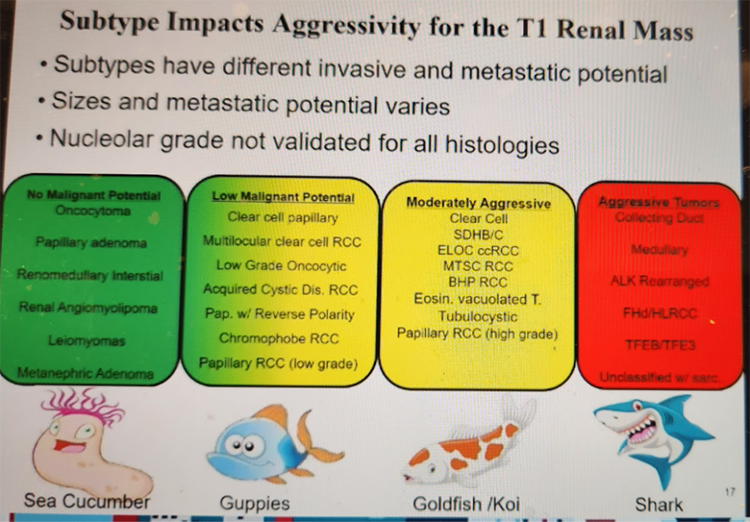
Those on the far right, even at smaller sizes, may require radical nephrectomy. Those on the far left, even at larger sizes, may not require any treatment.
We know from prior data that histology predicts behavior. Indolent histology can always have safe initial (and long-term) monitoring – while rare aggressive variants can spread at a small size.
Summarizing treatment outcomes in 2023:
- Active surveillance has outstanding outcomes
- Ablation for < 3 cm renal masses has excellent long-term outcomes
- SBRT has good short term local control (2-3 years)
- Partial nephrectomy is safe for most larger masses - but sometimes when you play with fire, you will get burnt!
- We have an effective adjuvant immunotherapy for high risk RCC – and the FDA label does NOT mention histology or stage
He specifically spent time noting that it can, and should be, considered for more aggressive variants even at small sizer and earlier stage. They have had success getting it approved.
As treatment intensification is associated is associated with increased rate of treatment related immediate side effects and potential long-term effects, he will discuss additional stratification tools with each patient as below to help guide best therapy:
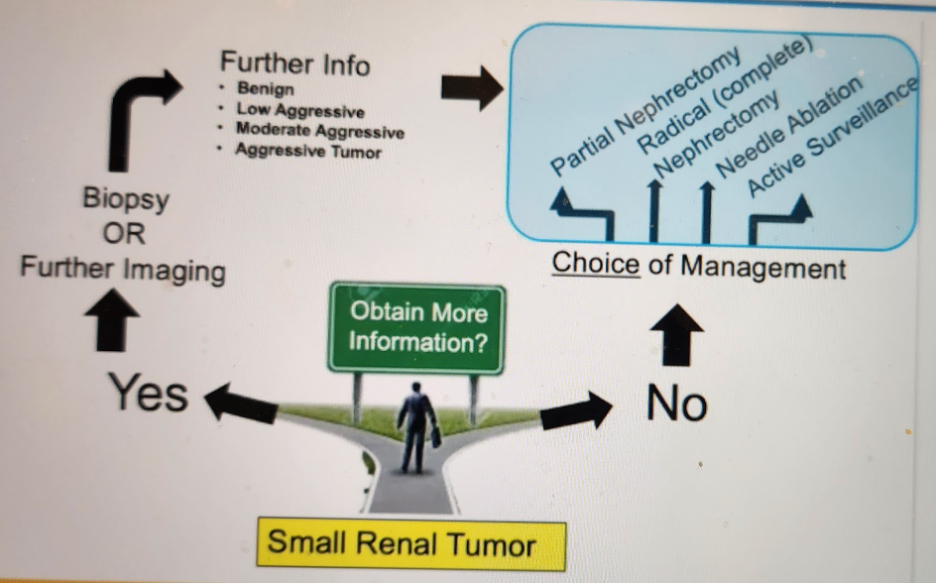
What are different methods of identifying histology prior to treatment decision, as of 2023?
1) Renal mass biopsy + IHC panel
2) Multi-phased CT and MRI
3) SPECT/CT MIBI
4) Upcoming – Zircon PET/CT
5) Upcoming – Hyperpolarized C13 MRI
Renal mass biopsy (RMB) – this is well established and commonly utilized. Certain high volume centers use it routinely. It oftens leads to unnecessary surgery – and is very safe in the modern setting. BUT, his take home point, is that you should work with your pathologist to send these tissue biopsies for IHC panel testing to better identify known and emerging renal mass entitities. “When in doubt, send it out.”

These above findings may help negate need for therapy.
He briefly discussed multi-phased CT MRI and noted that by looking at various phases, there is data to support better identification of different histologic subtypes, as they often have different vascularity.
- While there is overlap between histologies, specificity for papillary RCC is 85%
Sestamibi SPECT/CT scans have shown excellent promise in identifying mitochondrial avid lesions – chromophobe RCC and oncocytomas.
- These cases are ideal for observation or ablation
- Specificity is ~96% on meta-analyses
A very promising new option is a Zircon PET/CT (89Zr-TLX-250) for clear cell RCC. He just led a prospective open label phase III study, in which patients were tested and then underwent surgery. He presented this at GU ASCO.
Importantly, the patients that were false positives with papillary type tumors that expressed carbonic anhydrase IX (CAIX) – arguably patients that also needed treatment. When they were included, PPV approached 100%.
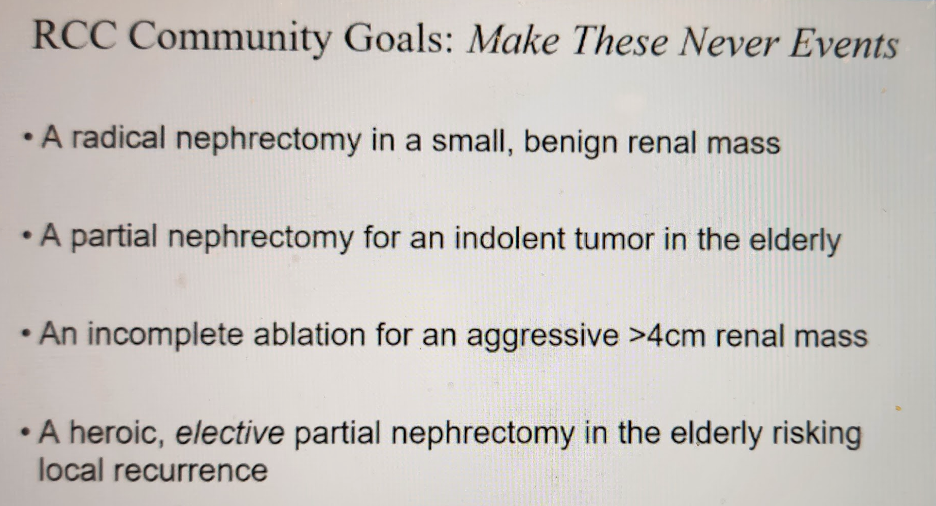
He ended the session by stating that the RCC community should make the following situations never events:
Presented by: Brian Matthew Shuch, MD, David Geffen School of Medicine at UCLA
Written by: Thenappan (Thenu) Chandrasekar, MD – Urologic Oncologist, Associate Professor of Urology, University of California, Davis @tchandra_uromd @UCDavisUrology on Twitter during the 2023 American Urological Association (AUA) Annual Meeting, Chicago, IL, April 27 – May 1, 2023