(UroToday.com) The 2023 AUA annual meeting included the Bladder Cancer Forum, featuring a debate discussing whether pathology or markers are more important. Dr. Yair Lotan started by presenting a case of a 73 year old man who presented with gross hematuria and was found to have a bladder tumor on a CT scan, a > 3 cm bladder mass with no evidence of metastases or upper tract lesions. This patient’s GFR was 70 mL/min/1.73 m2 and he had a 20 pack year smoking history. The initial TURBT showed high grade T1 and multifocal CIS, including 5% micropapillary differentiation, positive for lymphovascular invasion, with muscle in the specimen but negative for muscle invasion. Re-resection was completed 4 weeks later and pathology reveal high grade Ta disease.
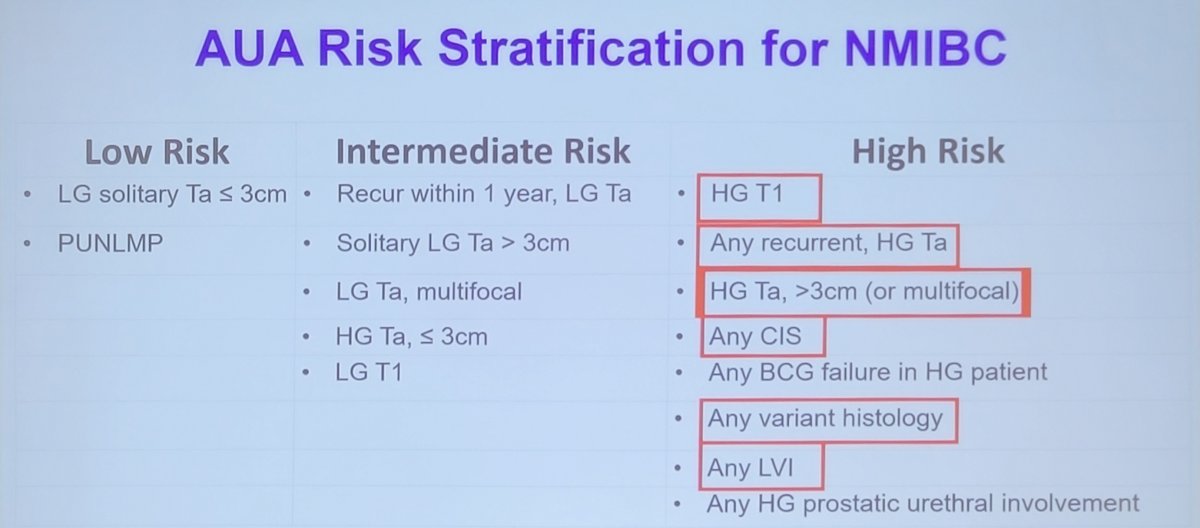
What can pathology offer this patient? Dr. Charles Guo, pathologist, notes that pathology not only establishes the definitive diagnosis of bladder cancer, but also provides histologic analysis to assist the optimal treatment, including (i) grade (high grade urothelial carcinoma), (ii) stage (pT1), (iii) variant histology (micropapillary 5%), (iv) lymphovascular invasion (yes), (v) muscularis propria involvement (no), and (vi) other (ie. CIS and prostatic urethral involvement). Many/most of the high-risk stratification system relies on accurate assessment from the pathologist:
Dr. Guo also discussed the difference between divergent differentiation versus histologic variants in the bladder cancer. Divergent differentiation is a separate lineage from urothelial carcinoma, with the 2022 WHO classification including squamous, glandular, trophoblastic, and Mullerian. Histologic variants are intrinsically urothelial carcinoma lineage but exhibit distinct morphology from conventional urothelial carcinoma. Based on the 2022 WHO classification, the term “variant” has been replaced by “subtype”, including micropapillary, nested, small cell carcinoma, plasmacytoid, sarcomatoid, microcystic, lymphoepithelioma-like, lipid-rich, clear cell, giant cell, and poorly differentiated.
Dr. Lotan noted that based on the EAU-ESMO Consensus on management of bladder cancer with variant histology, there was consensus that T1 high grade bladder urothelial cancer with micropapillary histology should be treated with immediate radical cystectomy and lymphadenectomy. This is also supported as a treatment option by the AUA guidelines:

If we assume the patient’s goal is organ preservation, Dr. Lotan poses the following questions:
- Do we have a therapeutic approach that will completely eliminate local disease?
- Do we have pre-treatment (predictive) biomarkers for that therapy? How accurate are they?
- Do we have robust methods to confirm efficacy?
Additionally, there are special challenges with organ preservation in micropapillary disease:
- We have insufficient data with mixed tumors to know how much micropapillary is bad: does all of the tumor share the same biology? Or just the part that looks micropapillary?
- BCG doesn’t work in micropapillary and we don’t know whether other local therapies are active either
- If there’s a strong motivation for bladder preservation, then a robust tool for detecting local minimal residual disease is needed
Dr. Lotan also notes that there are special considerations for systemic control of micropapillary disease. First, the disease has a propensity to metastasize, especially when lymphovascular invasion is present. Second, conventional imaging is not sensitive enough to identify micrometastases. Third, there are differences in local and distant control with local and systemic therapy. Fourth, a sensitive minimal residual disease assay should also be used to inform the plan.
Dr. Lotan then presented a second case of a 68 year old male referred for muscle invasive bladder cancer with TURBT showing high grade, muscle invasive disease resected on the left lateral wall and anterior wall. An exam under anesthesia suggested a mobile bladder and CT scan of the chest/abdomen/pelvis after TURBT showed no lymph node involvement or metastasis. His GFR was 82 mL/min/1.73 m2, with a normal cardiac history and liver function abnormalities. He notes that the patient opted for neoadjuvant chemotherapy. So, is pathology enough? Is there are benefit to molecular alterations and/or subtyping? Are there are other markers?
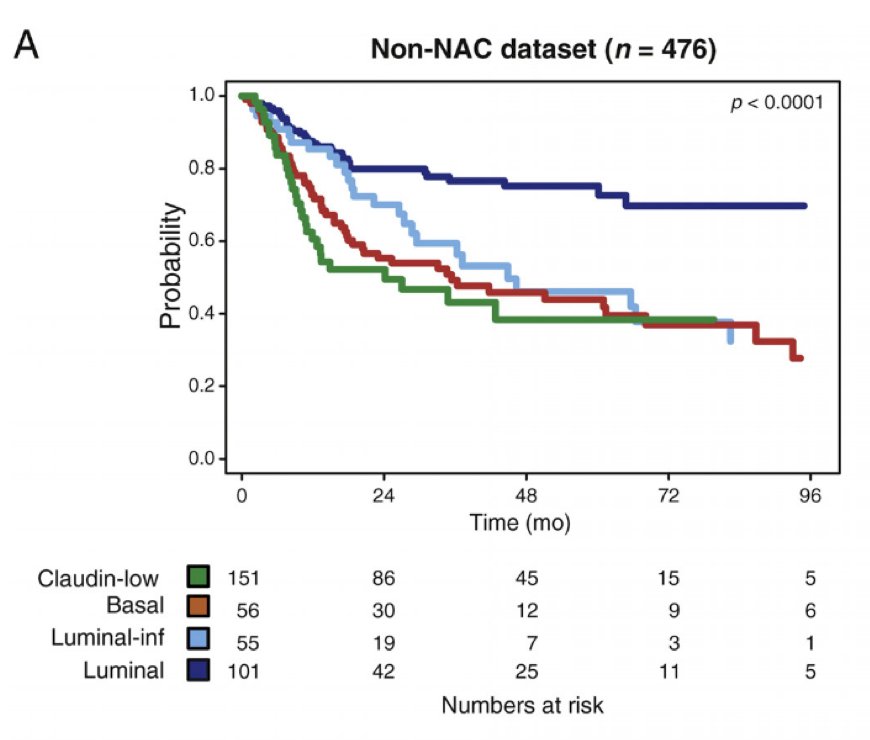
With regards to the role of subtyping, Dr. David McConkey notes that the luminal molecular subtype appears to have less aggressive clinical presentation (in many cases), reflected by good outcomes, with data indicating that luminal tumors are more likely to be organ-confined (pT1-2N0) at surgery. Non-organ confined tumors have greater benefit from neoadjuvant chemotherapy. Seiler et al. assessed pre-neoadjuvant chemotherapy transurethral specimens from 343 patients with muscle-invasive bladder cancer.1 Overall survival according to subtype was analyzed and compared with OS in 476 non-neoadjuvant chemotherapy cases (published datasets). Luminal tumors had the best overall survival with and without neoadjuvant chemotherapy:
The SWOG S1314 COXEN clinical trial was a biomarker validation trial, whereby among 167 evaluable patients the OR for pT0 with the gemcitabine-cisplatin gene expression model score in gemcitabine-cisplatin treated patients was 2.63 (95% CI 0.82-8.36]; for the dose dense MVAC COXEN gene expression model score with dose dense MVAC treatment, the OR was 1.12 (95% CI 0.42-2.95).2 The gemcitabine-cisplatin gene expression model score was applied to pooled arms (gemcitabine-cisplatin and dose dense MVAC) for downstaging with an OR of 2.33 (95% CI, 1.11-4.89).
Dr. McConkey notes that molecular subtypes do not clearly distinguish responders from non-responders (downstaging), although those with alterations appear to do much better with immunotherapy (SWOG SUBTYP trial). DDR alterations are better but are not perfect, and the verdict is still out on DDR mutations and TMT/radiation (with data pending). Urine DNA should be used to confirm local control if bladder preservation is the patient’s goal.
Dr. Lotan notes that this patient received 4 cycles of dose dense MVAC and post-treatment imaging was consistent with persistent bladder wall thickening without evidence of metastatic disease. He then underwent an uncomplicated cystectomy with pathology pT3a, negative nodes, and negative margins, and ultimately went on to receive adjuvant therapy. Dr. Guo highlighted that there are several predictive biomarkers provided by pathology at MD Anderson Cancer Center:
- For immune checkpoint inhibitor therapy: NGS for tumor mutational burden, IHC for MSI, and IHC for PD-L1
- For pemetrexed therapy: IHC for MTAP
- For Herceptin: IHC and FISH for Her2 test
- For the antibody drug conjugate enfortumab vedotin: IHC for nectin-4
- For adjuvant chemotherapy: IHC for CKS/6 and GATA3 for molecular subtyping
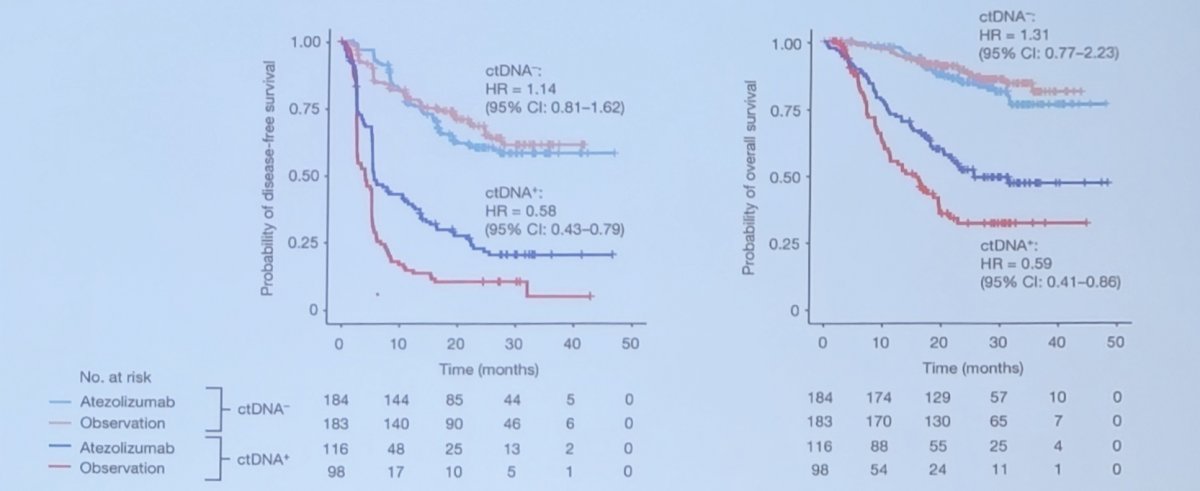
In the adjuvant setting, circulating tumor DNA is prognostic and predictive after adjuvant atezolizumab.3 Among 581 patients, ctDNA testing at the start of therapy (cycle 1 day 1) identified 214 (37%) patients who were positive for ctDNA and who had poor prognosis (observation arm HR 6.3, 95% CI 4.45-8.92). Notably, patients who were positive for ctDNA had improved disease-free survival and OS in the atezolizumab arm versus the observation arm (disease-free survival HR 0.58, 95% CI 0.43-0.79, OS HR 0.59, 95% CI 0.41-0.86):
To conclude this session, Dr. Lotan suggested the following take-home points for molecular markers and adjuvant therapy:
- Existing response biomarkers are not robust enough to withhold immunotherapy from patients whose tumors do not express them
- PET tracers that target PDL1 and other predictive immune biomarkers reveal inter-lesional heterogeneity
- Single-cell and spatial whole transcriptome studies visualize more heterogeneity and complexity and are exciting for discovery, but they’re not necessarily yielding better predictive biomarkers than bulk sequencing studies
- Minimal residual disease should be measured longitudinally via ctDNA, potentially holding off on adjuvant immunotherapy until ctDNA is detected
Moderator: Yair Lotan, MD, UT Southwestern Medical Center, Dallas, TX
Debater: Charles Guo, MD, MD Anderson Cancer Center, Houston, TX
Debater: David McConkey, MD, PhD, Johns Hopkins Greenberg Bladder Cancer Institute, Baltimore, MD
Written By: Zachary Klaassen, MD, MSc – Urologic Oncologist, Assistant Professor of Urology, Georgia Cancer Center, Augusta University/Medical College of Georgia, @zklaassen_md on Twitter during the 2023 American Urological Association (AUA) Annual Meeting, Chicago, IL, April 27 – May 1, 2023
References:
- Seiler R, Al Deen Ashab H, Erho N, et al. Impact of molecular subtypes in muscle-invasive bladder cancer on predicting response and survival after neoadjuvant chemotherapy. Eur Urol. 2017 Oct;72(4):544-554.
- Flaig TW, Tangen CM, Daneshmand S, et al. A randomized phase II study of Coexpression Extrapolation (COXEN) with Neoadjuvant Chemotherapy for Bladder Cancer (SWOG S1314; NCT02177695). Clin Cancer Res. 2021 May 1;27(9):2435-2441.
- Powles T, Assaf ZJ, Davarpanah N, et al. ctDNA guiding adjuvant immunotherapy in urothelial carcinoma. Nature. 2021 Jl;595(7867):432-437.